
Artificial intelligence (AI) refers to computational systems capable of performing tasks typically associated with human intelligence, such as learning, problem-solving, and making data-driven decisions based on available data.1 Across industries worldwide, enthusiasm for AI is rapidly expanding, and healthcare is no exception. In cardiovascular imaging, AI has found applications at every step of the workflow—from determining the indication and protocol of a study, through image acquisition and reconstruction, to post-processing, analysis, and quantitative assessment. This shift from image interpretation toward holistic disease characterization represents a paradigm shift: imaging is no longer a standalone diagnostic tool but part of an integrated framework that can inform prevention, personalize therapy, and predict outcomes. At the same time, the growing role of AI in cardiovascular imaging must be considered in the context of escalating demand, rising healthcare costs, and workforce burnout. As imaging volumes rise, clinicians and imaging specialists face increasing demands for speed and accuracy. AI may help by reducing time spent on manual tasks, improving efficiency across the imaging pathway, and enabling smarter allocation of healthcare resources. Beyond image interpretation, AI serves as a bridge that connects imaging findings with genomics, circulating biomarkers, and clinical data, thereby functioning as an integrative tool in modern medicine.
Over time, AI has demonstrated its utility across a wide range of imaging modalities: from detecting coronary artery disease2 or left ventricular (LV) systolic dysfunction3 on chest X-rays, to identifying coronary calcifications on cardiac computed tomography (CT) and on CT scans performed for lung cancer screenings.4 Its applications extend to the automated quantification of chamber size, function, and strain in echocardiography and cardiovascular magnetic resonance (CMR),5 as well as to myocardial tissue characterization with CMR, including late gadolinium enhancement and parametric mapping. AI has also been applied to myocardial perfusion assessment in single-photon emission CT.6
Beyond these specific use cases, the real value of AI lies in its ability to standardize image interpretation and minimize inter-observer variability, which has historically limited reproducibility in cardiovascular imaging. Algorithms can also process vast amounts of imaging data more rapidly than humans, making them particularly suited for high-volume clinical environments where efficiency is critical. Emerging approaches such as radiomics extract high-dimensional features from routine scans, enabling a more nuanced characterization of myocardial tissue and vascular structures. While many applications are still in the research phase, some AI-enabled tools have already reached clinical practice, where they assist in streamlining workflows, reducing reporting times, and supporting earlier disease detection. Moreover, machine learning can be used to combine imaging-derived variables into predictive risk scores that outperform conventional models. This advantage becomes even more pronounced in multimodal settings, where data from multiple imaging modalities are available for the same patient.7
According to the 2022 ESC Guidelines on cardio-oncology, baseline cardiac evaluation is essential in patients scheduled to receive potentially cardiotoxic agents—particularly anthracyclines, HER2-directed therapies, or in those with high or very high cardiovascular risk prior to chemotherapy.8 Transthoracic echocardiography (TTE) remains the first-line imaging tool for this purpose, given its accessibility and reproducibility. The diagnosis of cancer therapy–related cardiac dysfunction is primarily based on reductions in LV ejection fraction (LVEF) and/or alterations in global longitudinal strain. CMR serves as a valuable alternative when echocardiography is inconclusive, technically limited, or when detailed tissue characterization is required. In selected cases, nuclear imaging may also be considered a third-line option in this diagnostic pathway.
The potential for cardiovascular complications from radiotherapy should also be considered. For individuals with known cardiovascular disease (CVD), an echocardiographic evaluation should be performed before treatment if the planned radiation field involves the heart. Moreover, in patients undergoing thoracic irradiation, longer-term surveillance is recommended, as cardiovascular toxicity can manifest years after completion of therapy. This includes not only cardiomyopathy, but also accelerated atherosclerosis, valvular disease, and pericardial involvement, all of which may benefit from early detection through structured imaging protocols.
Cardio-oncology relies heavily on serial imaging and biomarkers to detect subclinical dysfunction long before symptoms occur. More recently, AI has entered the field of cardio-oncology imaging, offering new opportunities for precision and early detection. AI excels where (i) subtle imaging changes must be detected reproducibly, (ii) longitudinal patterns need interpretation, and (iii) multimodal data (imaging, biomarkers, clinical data, genomics) must be integrated.
Cardiovascular imaging is a cornerstone in detecting and monitoring the cardiotoxic effects of oncological therapies, and AI can enhance this role by improving the accuracy of conventional measures, while also enabling the identification of novel biomarkers and subtle imaging alterations that may otherwise go unnoticed (Figure 1). In cancer survivors, CVD has become the predominant cause of illness and death unrelated to cancer itself.
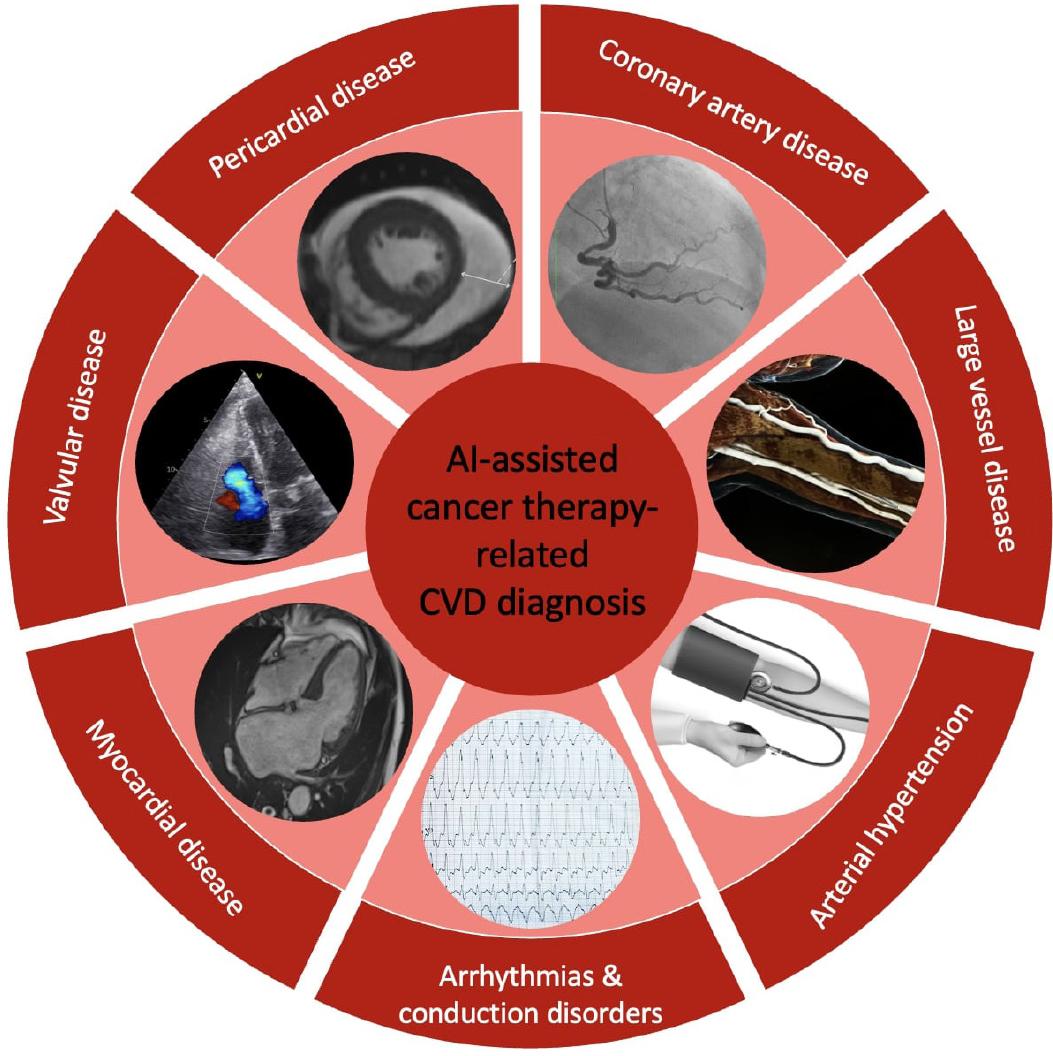
Detection of cancer therapy-related CVD using AI in cardiovascular imaging (original content).
Abbreviations: AI: artificial intelligence; CVD: cardiovascular disease.
A recent systematic review by Mushcab H. and colleagues summarized the applications of imaging-based AI in cardio-oncology for cardiotoxicity assessment.9 The authors identified seven studies published between 2018 and 2023, in which machine learning (ML) and deep learning approaches were applied to echocardiography (including transesophageal studies), CMR and chest CT. These studies demonstrated the potential of AI to enable earlier detection of cardiovascular complications related to cancer therapies, particularly in breast cancer and diffuse large B-cell lymphoma. Compared with traditional manual approaches, AI achieved greater accuracy and efficiency in detecting therapy-induced cardiac dysfunction.
A narrative review by Ravera F et al. has highlighted the broader applications of AI in cardio-oncology, including a dedicated focus on cardiovascular imaging.10 ML models can predict subsequent LVEF decline by analyzing baseline strain and strain rate patterns. Such predictive capability provides an opportunity to identify high-risk patients, enabling closer surveillance and timely initiation of preventive strategies. AI can also assist non-cardiology healthcare professionals—such as oncologists and even nurses—in obtaining accurate measurements of LVEF. This is particularly valuable, since in cardio-oncology, patients are typically seen by cardiologists only at specific intervals or when clinically indicated, whereas they are followed much more frequently by their treating oncologist. AI-assisted tools could empower non-cardiology healthcare providers to reliably monitor cardiac function at the point of care, even outside specialized cardiovascular clinics, and facilitate timely referral for expert evaluation.
Beyond describing the role of TTE in monitoring LV functional parameters, the authors also examine studies using CT. They illustrate how convolutional neural networks can be applied to identify CVD and estimate cardiovascular mortality risk, based on coronary or even thoracic aortic calcium scoring, particularly in patients exposed to radiotherapy. The calcium score is an easily accessible parameter, requiring only a short protocol without the need for contrast injection, yet it yields substantial information on coronary risk. A key point is that AI-driven automated calcium scoring can be derived directly from radiotherapy planning CT scans, without requiring a dedicated coronary CT. This approach minimizes unnecessary radiation exposure and lowers procedural costs, while still providing valuable cardiovascular risk information.
Overall, these results pave the way for a new era where imaging in cardio-oncology evolves from being primarily descriptive to becoming predictive and integrative (Figure 2). The convergence of AI with longitudinal clinical data could enable comprehensive models of cardiotoxicity risk, moving the field from reactive management to proactive prevention. Another important consideration is the potential for AI to improve equity and sustainability in healthcare systems. Automated analysis may reduce dependency on highly specialized expertise and streamline workflows, which is critical in resource-limited settings or overburdened imaging services. By lowering the barrier to advanced cardiovascular monitoring, AI could make cardio-oncology care more accessible to patients worldwide.
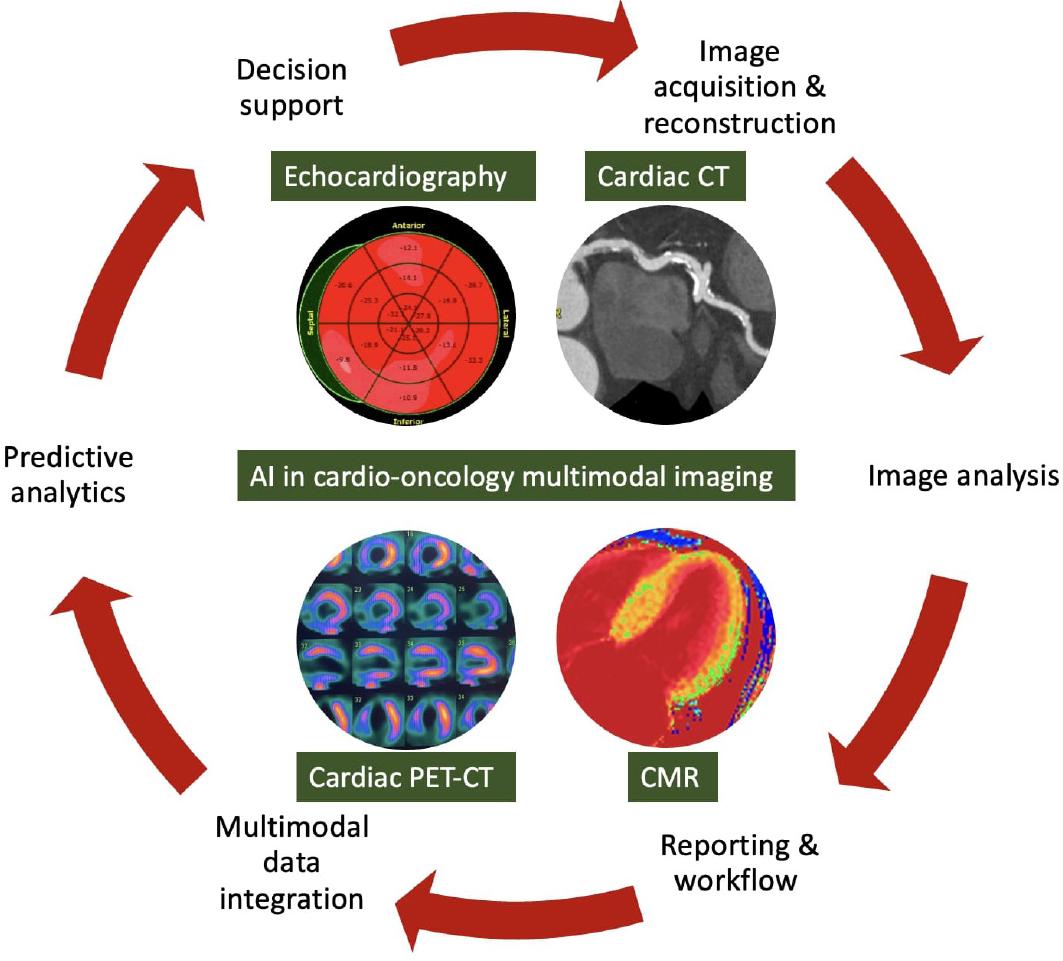
Steps and applications of AI in cardio-oncology imaging (original content).
Abbreviations: AI: artificial intelligence; CMR: cardiovascular magnetic resonance; CT: computed tomography; PET:c positron emission tomography.
Despite this promise, several hurdles must be addressed before AI becomes a routine part of cardio-oncology practice. Current studies are limited by small cohorts, heterogeneous imaging protocols, and variability across vendors and platforms, all of which restrict generalizability. Standardization of acquisition and reporting, coupled with large-scale, multicenter validation, will be essential to establish reliability. Beyond technical issues, ethical considerations—including data privacy, algorithmic transparency, and equitable access—are critical to ensure responsible implementation. Importantly, AI should be viewed not as a replacement for clinical expertise, but as a partner that enhances efficiency and precision. The success of AI in cardio-oncology will depend on collaborative ecosystems that bring together cardiologists, oncologists, imaging specialists, data scientists, and regulators. Such partnerships will be key to transforming AI from a promising innovation into a trusted component of patient-centered care.
AI is rapidly transforming the landscape of cardiovascular imaging, moving beyond automation and efficiency gains toward redefining how we detect, monitor, and ultimately prevent cardiovascular complications in oncology patients. By enabling earlier recognition of subclinical dysfunction, integrating multimodal data, and extending cardiovascular expertise to non-specialist clinicians, AI has the potential to shift cardio-oncology from managing complications to preventing them. At the same time, responsible integration requires rigorous validation, transparency, and collaboration across disciplines to ensure equitable access and trust. If these challenges are met, AI can serve not only as a powerful tool for precision imaging but also as a catalyst for more personalized, sustainable, and patient-centered cardio-oncology care.