The selection of an appropriate guidewire is critical in the management of complex coronary anatomies. In tortuous coronary vessels, standard guidewires may exert excessive force on the vessel wall, leading to the concertina effect. In severe cases, straightening of the vessel can result in marked ischemia [1] and even hemodynamic instability [2]. Another major concern when wiring such tortuous and typically fragile vessels is the risk of dissection, which can have catastrophic consequences in this context. The Suoh 03 (Asahi Intecc) is an exceptionally soft and flexible 0.014” guidewire specifically designed for navigating highly tortuous collateral channels during chronic total occlusion (CTO) interventions. Its ultra-low tip load of 0.3 gf and unique distal rope coil construction provide excellent trackability and atraumatic vessel navigation, minimizing the risk of vessel injury. Although originally developed for retrograde collateral crossing, the Suoh 03 has also demonstrated effectiveness in managing coronary artery dissections [3], particularly when conventional wires fail to re-enter the true lumen. Its combination of exceptional flexibility, hydrophilic coating, and precise torque response makes it an invaluable tool for navigating complex anatomies where precision and vessel preservation are critical. We present a case in which the anticipated risk of the concertina effect and wire-induced dissection in a severely tortuous LAD was successfully managed through the upfront use of the Suoh 03 guidewire.
The patient was a 62-year-old woman with a history of type 2 diabetes, hypertension, hypercholesterolemia, and peripheral artery disease who underwent cardiologic evaluation prior to planned endovascular repair of the abdominal aorta. She reported exertional angina of six months’ duration, now classified as Canadian Cardiovascular Society (CCS) class III. Electrocardiography and echocardiography were unremarkable. Given her high-risk profile, typical symptoms, and the impending vascular surgery, the decision was made to proceed directly to coronary angiography. The angiogram revealed a markedly tortuous left anterior descending (LAD) artery with two tight tandem stenoses (~90% diameter narrowing) in the mid-to-distal segments (Figure 1). Coronary spasm was excluded following the intracoronary administration of nitroglycerin. The right coronary and circumflex arteries demonstrated only mild atherosclerotic disease. The severe tortuosity of the LAD raised concerns regarding the risk of concertina effect and wire-induced dissection during intervention.
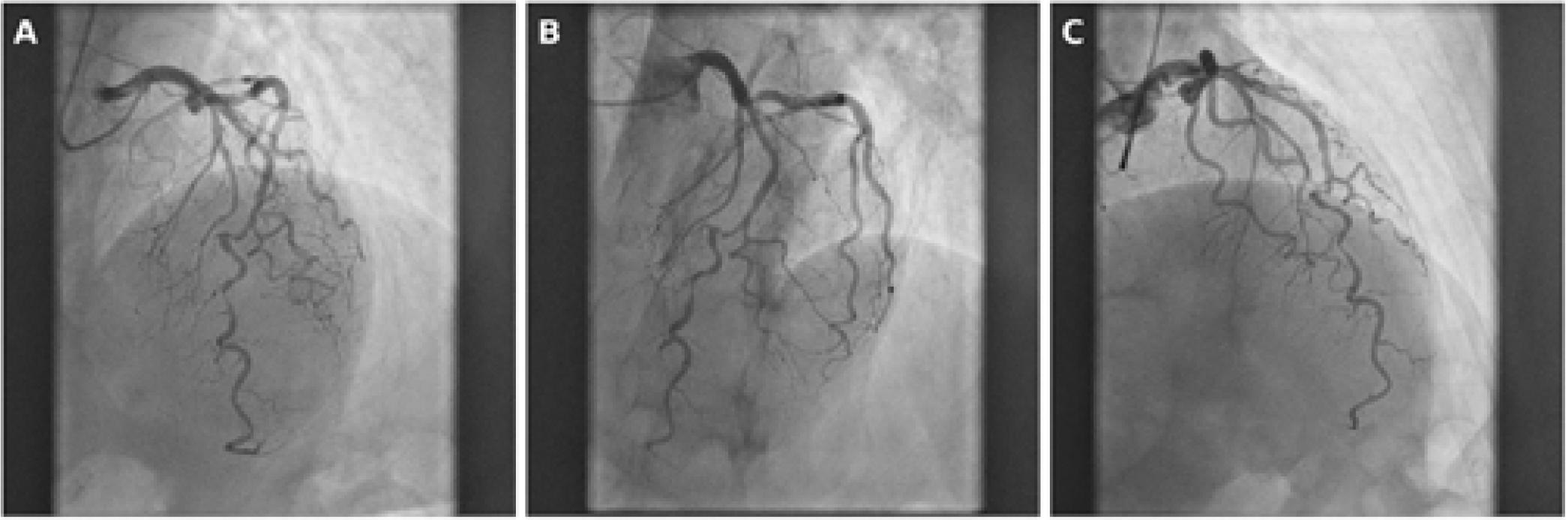
Diagnostic coronary angiography in three standard projections. A: AP cranial view. B: LAO cranial view. C: RAO cranial view. All views show a highly tortuous mid-to-distal LAD with tight tandem lesions in the medial segment.
We proceeded with PCI of the LAD tandem stenoses to achieve relief of angina symptoms. To mitigate the aforementioned risks, an ASAHI Suoh 03 guidewire was selected from the outset. This wire, featuring a 0.3 gram-force tip and high flexibility, was expected to follow the vessel’s natural curvature without exerting traumatic force on the vessel wall. The Suoh 03 successfully navigated the tortuous LAD and easily crossed both stenoses (Figure 2). Postwiring angiography confirmed the absence of a significant concertina effect and demonstrated TIMI III flow (Figure 4A), while the patient remained hemodynamically stable.
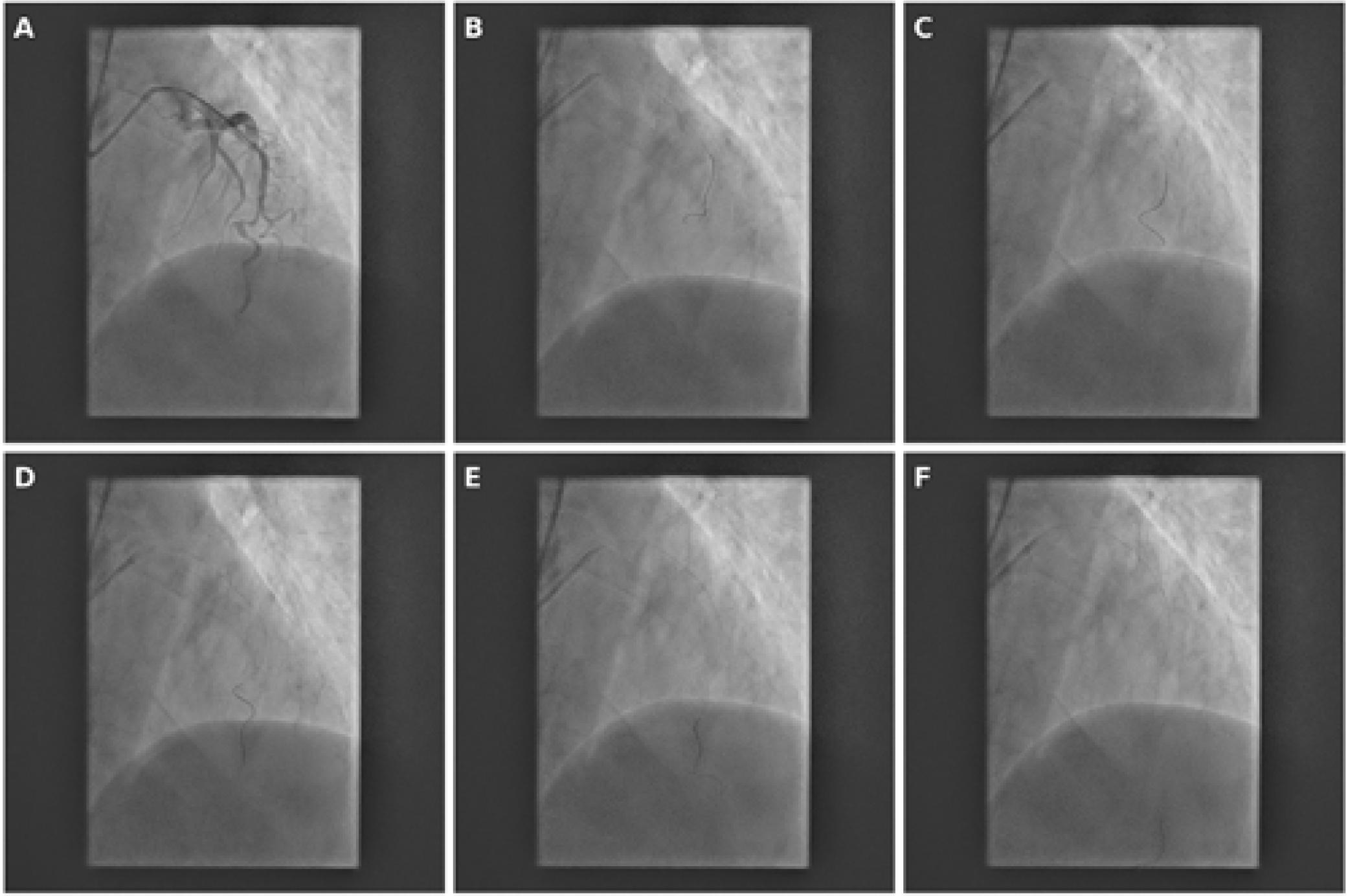
Stepwise navigation of a Suoh 03 wire through a tortuous LAD. A–F: Sequential advancement of the Suoh 03 wire shows safe progression through sharp angulations while minimizing trauma to the vessel wall.
The lesions were pre-dilated using a 2.5 mm non-compliant balloon (Boston Scientific Emerge). Post-PTCA angiography revealed pseudo-lesions consistent with a mild concertina effect, but without flow limitation (Figure 4B). Two drug-eluting stents (2.5 × 30 mm and 3.0 × 20 mm; Promus Elite, Boston Scientific) were then deployed, followed by post-dilation with a 3.0 mm non-compliant balloon (Figure 3). The final angiogram demonstrated excellent stent expansion and TIMI III flow (Figure 5). The patient remained hemodynamically stable and was discharged on dual antiplatelet therapy. Her planned vascular surgery proceeded uneventfully at a later date.
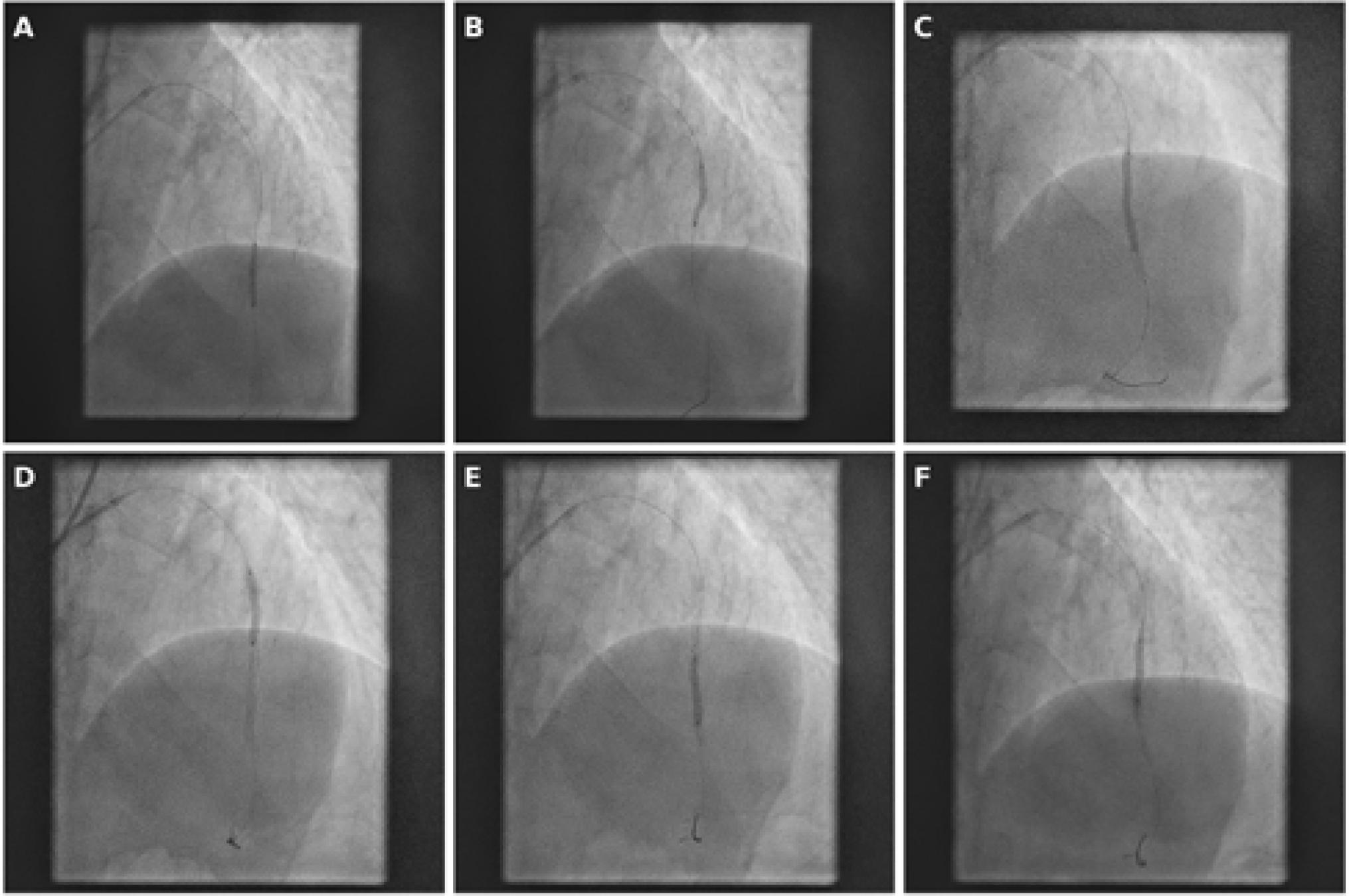
PTCA and stenting of the mid-to-distal LAD segment. A–B: Pre-dilatation with balloon angioplasty. C–D: Deployment of two drug-eluting stents. E–F: Final post-dilatation to ensure optimal stent apposition.
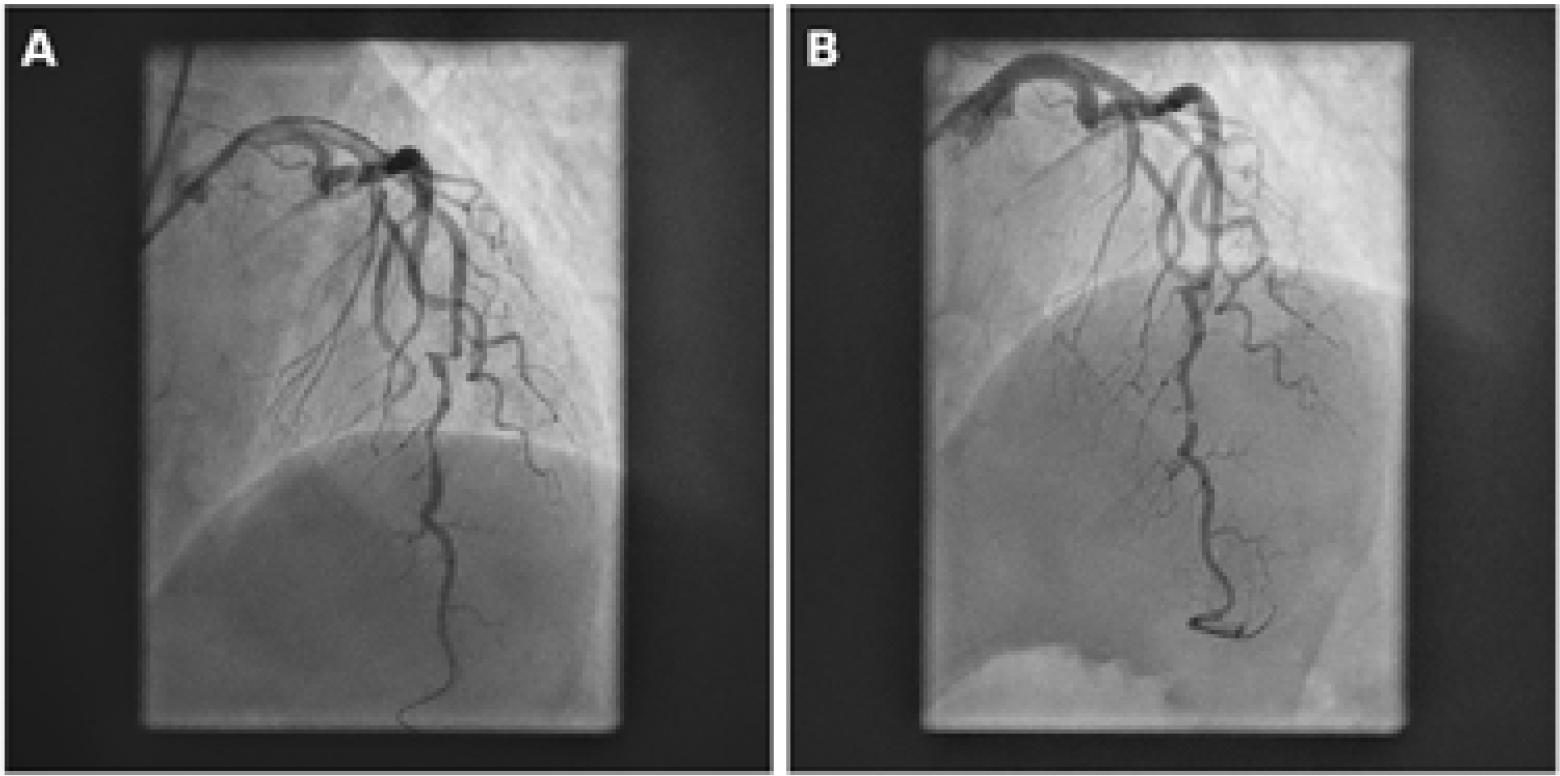
Angiographic assessment of the concertina effect. A: After successful wiring, no concertina effect is visible with TIMI III flow. B: After PTCA, the vessel shows minimal concertina effect, still maintaining TIMI III flow.
This case underscores the importance of selecting guidewires tailored to anticipated anatomic and procedural challenges. The concertina effect is a well-recognized phenomenon in tortuous vessels, resulting from vessel straightening by stiff equipment, which can mimic dissection or true stenosis. Differentiating this from true pathology is essential to avoid unnecessary or potentially harmful interventions. While commonly associated with stiff wires, there are reports describing severe manifestations of this effect even with workhorse wires [4]. In addition, severely tortuous vessels are inherently fragile and technically challenging to wire. Repeated attempts may induce dissections, complicating true lumen re-entry and potentially leading to serious complications. In this case, the Suoh 03 wire was selected upfront for its ability to navigate tortuous anatomy atraumatically. Its ultra-soft tip minimizes the risk of concertina effect and significantly reduces the likelihood of vessel injury compared to standard wires. The successful use of this wire enabled smooth lesion crossing, limited pseudo-lesion formation, and preservation of distal coronary flow.
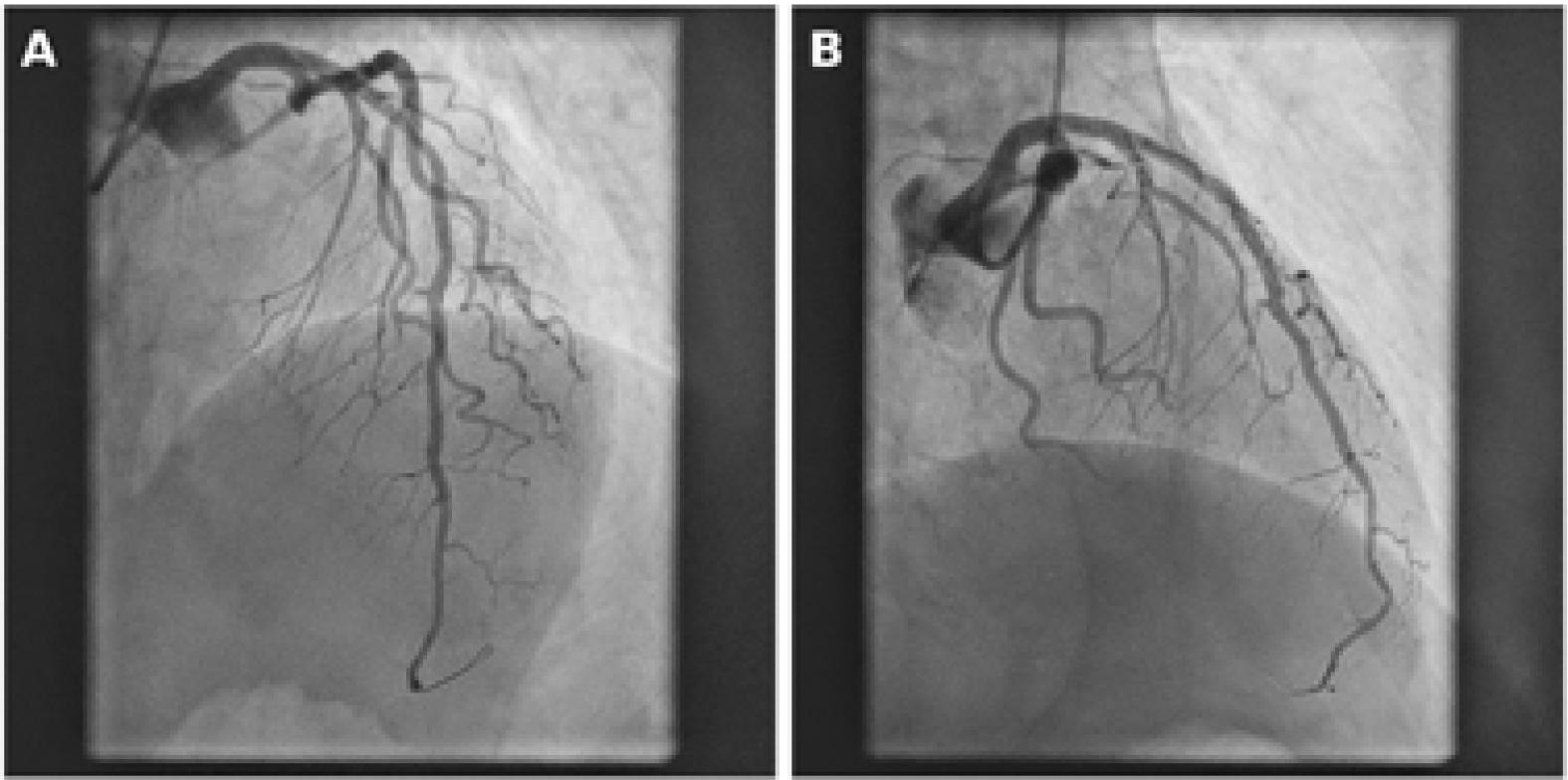
Final angiographic result, showing fully expanded stents. A: AP cranial view. B: RAO cranial view.
In patients with tortuous coronary anatomy undergoing PCI, careful procedural planning and the selection of appropriate guidewires are essential for success. In this case, the upfront use of the Suoh 03 wire enabled safe navigation through a severely tortuous LAD, minimized the concertina effect, and prevented dissection—effectively transforming a complex and potentially high-risk PCI into a straightforward and safe procedure. This case highlights the critical role of strategic guidewire selection in optimizing outcomes in complex coronary interventions.