Catheter ablation has become one of the main strategies in the treatment of symptomatic atrial fibrillation (AF)1, either as a first line or after failing an antiarrhythmic medication. Peri-procedural anticoagulation is critical, as the risk of stroke is heightened due to intracardiac catheter manipulation, endothelial inflammation, or damage2 and restoration of sinus rhythm with atrial stunning3–5. Traditionally, vitamin K antagonists (VKA), as warfarin or other derivatives, such as phenprocoumon, acenocoumarol, marcoumar (with a longer half-life), have been used, either continuously or interrupted with heparin bridging, as the anticoagulation strategy. Although no standardized protocol exists, it has been suggested that an uninterrupted VKA protocol, with the procedure performed during therapeutic INR, might be superior6,7 to a bridging strategy.
The direct oral anticoagulants (DOACS) including the direct thrombin inhibitor, dabigatran (D) approved by the FDA in 2010, and the factor Xa factor inhibitors, rivaroxaban (R) approved in 2011, apixaban (A) in 2013, and edoxaban (E) in 2015, have been shown in large studies to be at least as effective as VKA in reducing the risk of stroke in patients with non-valvular AF8–11. Currently, these agents are the preferred anticoagulation strategy for peri-procedural anticoagulation for AF ablation, avoiding the disadvantages of frequent INR checks, additional need for transesophageal echocardiograms, or postponing procedures due to nontherapeutic anticoagulation with VKA. Despite widespread adoption of the DOACS, a significant number of procedures are still performed while patients are on VKA. On the other hand, there is only a trifling experience with the approved reversal agents for DOACS 12 in the procedural settings due to the low incidence of life-threatening bleeding in general, high cost, and short shelf life. In addition, different responses to intraprocedural heparin administration 13,14 could lead to increased periprocedural thromboembolic events.
Multiple small series have compared DOACS with various VKA agents as anticoagulation strategies for AF ablation, examining both interrupted and uninterrupted strategies, and concerns have been raised regarding a possible higher incidence of peri-procedural embolic and bleeding rates for DOACS compared with warfarin (W) 15–17. However, given the low procedural complication rates, these studies may be too small to compare different anticoagulation regimens and agents accurately.
The objective of the current meta-analysis is to review all the available studies to date that compare the thromboembolic and bleeding complications of DOACS versus VKA regimens and to identify the safety of different peri-ablation anticoagulation strategies, including (1) uninterrupted and interrupted regimens, (2) individual DOACS (dabigatran, rivaroxaban, or apixaban) vs. uninterrupted VKA, and (3) DOACS vs. non-warfarin VKA.
A comprehensive search was conducted in PubMed Central, EMBASE, and Ovid-Medline databases from October 2010 to October 2023, dating back to the FDA approval of dabigatran in the USA. The keywords used were “DOACS”, “dabigatran”, “rivaroxaban”, “apixaban” or “edoxaban” and “VKA”, “warfarin”, “phenprocoumon”, “acenocoumarol” and “atrial fibrillation”, “atrial fibrillation ablation”, “ablation”, “catheter ablation”, “pulmonary vein isolation”, “PVI”, “AFib ablation”, “AF ablation”. No language restriction was used.
The studies were included in the analysis if they enrolled patients undergoing AF ablation, had two arms as peri-procedural anticoagulation strategies: DOACS (D, R, A or E), and VKA (either continuous or interrupted with heparin bridging), and compared periprocedural bleeding and/or thromboembolic complications, up to 30 days, between the two anticoagulation strategies. Studies with the change of pre-vs post-procedure anticoagulation strategy were excluded.
The study selection strategy following PRISMA guidelines is presented in Figure 1. Of 2746 studies, after a thorough screening and evaluation process, 53 full-text13–65 studies were included.
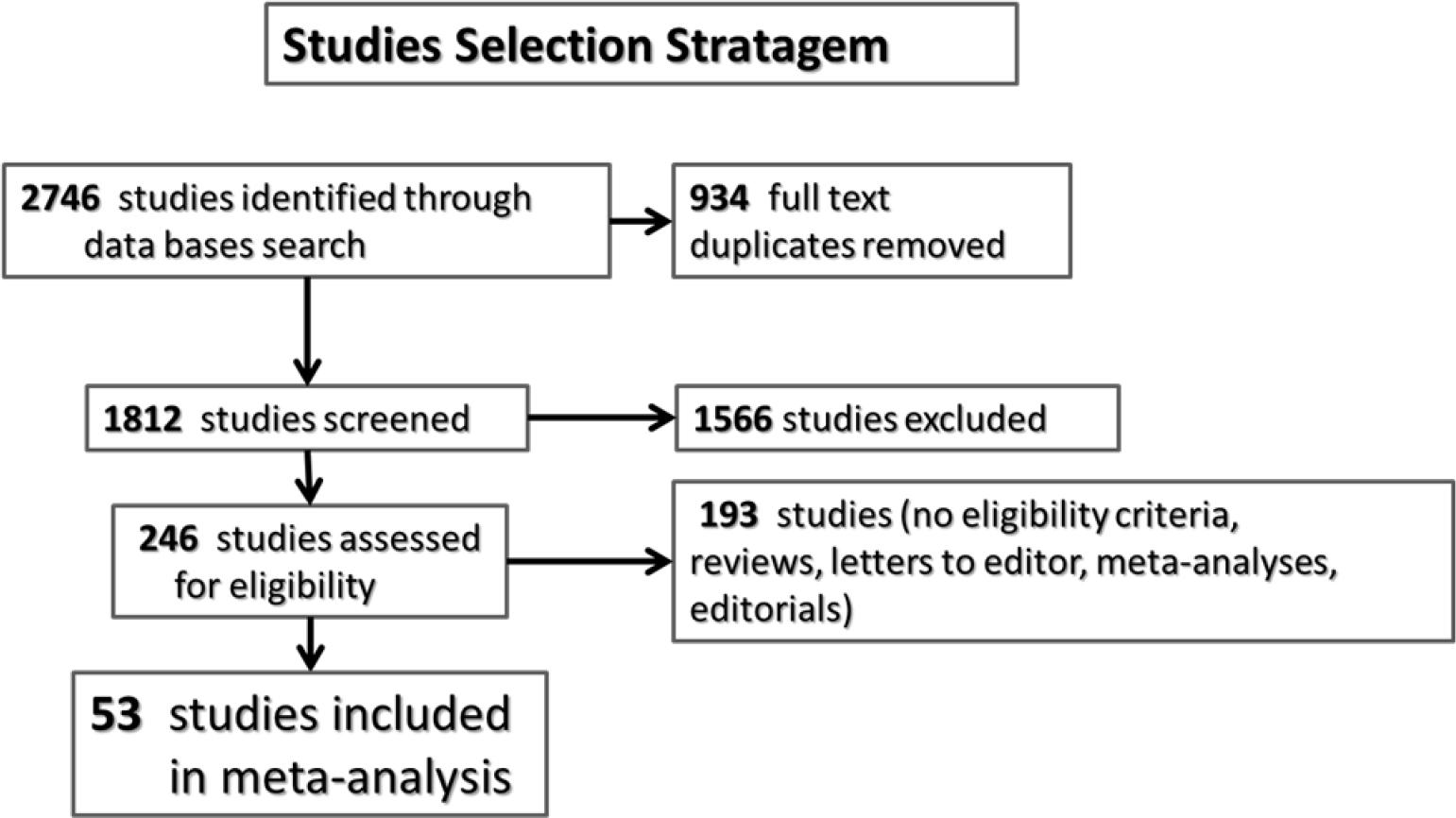
Studies selection Stratagem.
The strength of evidence of the studies was evaluated based on the type of study (randomized, observational, prospective, retrospective, etc.), study limitations, directness, consistency, precision, and risk for bias66. Using the GRADE suggested ratings, the studies were categorized into: High, Moderate, Low, or Insufficient, based on the confidence that the estimated effect is close to the true one for the outcome66.
The studies were reviewed for design, inclusion criteria, total number of patients, number of patients in each group, baseline characteristics including age, gender, CHADS2 and CHA2DS2VASc scores, prior stroke, use of antiplatelet medication, left ventricular function and left atrial dimensions, details regarding holding and restarting the anticoagulation in the D, R, A and E arms, the bridging strategy for VKA patients, and INRs for patients on uninterrupted VKA, the ablation strategy, and peri-procedural complications (up to 30 days post procedure) in each group. Complications were categorized into:
- –
Thromboembolic (TE) complications: stroke or transient ischemic attack [TIA], other systemic TE, and deep vein thrombosis (DVT) with or without pulmonary embolism)
- –
Major bleeding complications: any significant bleeding that required intervention (cardiac tamponade, access site bleeding, etc) or any significant bleeding (GI, hemoptysis, etc.) with hemoglobin fall > 2g/l or required blood product transfusion
- –
Minor bleeding complications: no intervention necessary, including pericardial effusions that were conservatively managed or small groin hematomas
The primary outcomes for this study included total complications, thromboembolic and composite, major and minor bleeding complications in patients treated with the DOACS regimen vs patients on VKA.
The secondary outcomes included:
Thromboembolic, major and minor bleeding of interrupted and uninterrupted DOACS versus uninterrupted VKA.
Thromboembolic, major, and minor bleeding of DOACS versus interrupted VKA.
Thromboembolic and bleeding of D, R, A compared to uninterrupted VKA (evaluation of E versus VKA could not be performed due to a low number of patients)
Thromboembolic, major, and minor bleeding comparison between DOACS and uninterrupted non warfarin VKA
Meta-analysis data were reported as odds ratio (OR) with the 95% confidence interval (CI). The Mantel-Haenszel random effect model was used to pool the study results, and a random effects model was used to pool heterogeneous samples/results. The RevMan 5.3 software [Review Manager (RevMan) Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014] was used for the analysis. A p < 0.05 was considered statistically significant.
Statistical heterogeneity among included studies was assessed using chi2 and I2. The I2 statistic describes the proportion of variation in the treatment estimate unrelated to sampling error. A zero value indicates no heterogeneity, 25–49% low, 50–74% moderate, and > 75% a high degree of heterogeneity. A funnel plot was used to assess the potential for publication bias in the dataset (Figure 2).67
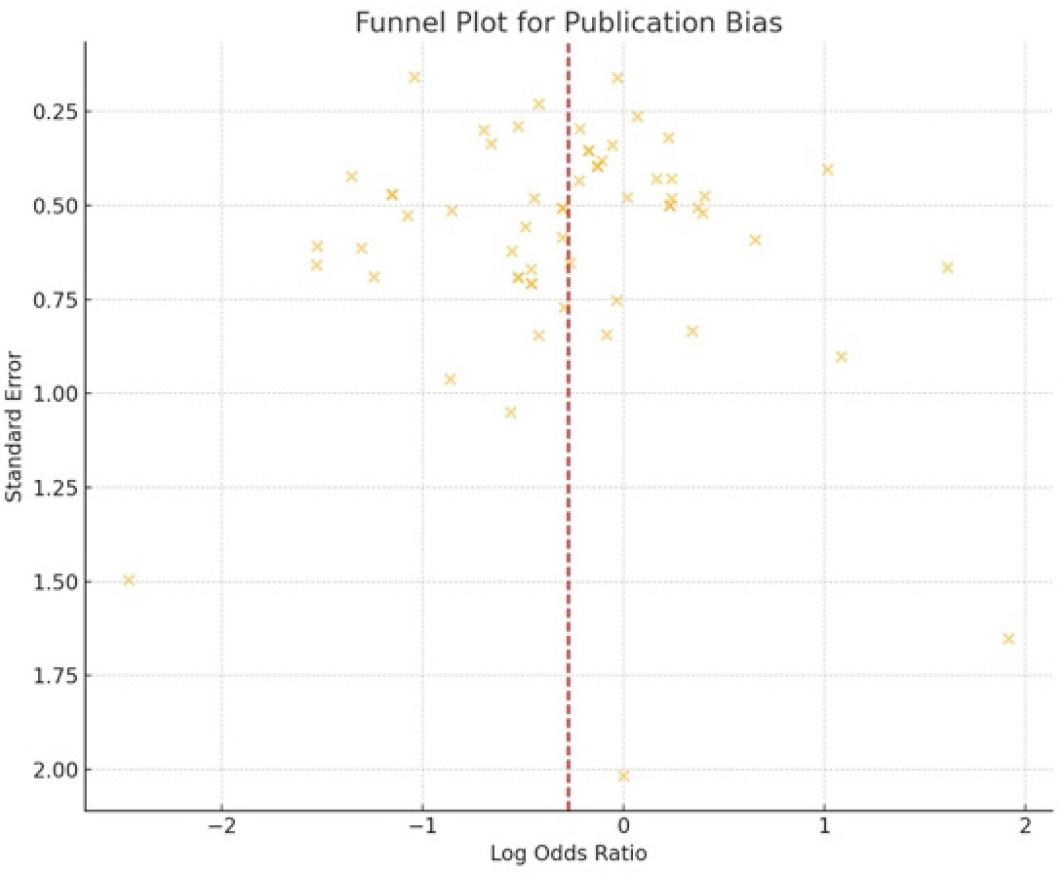
Funnel Plot for publication bias.
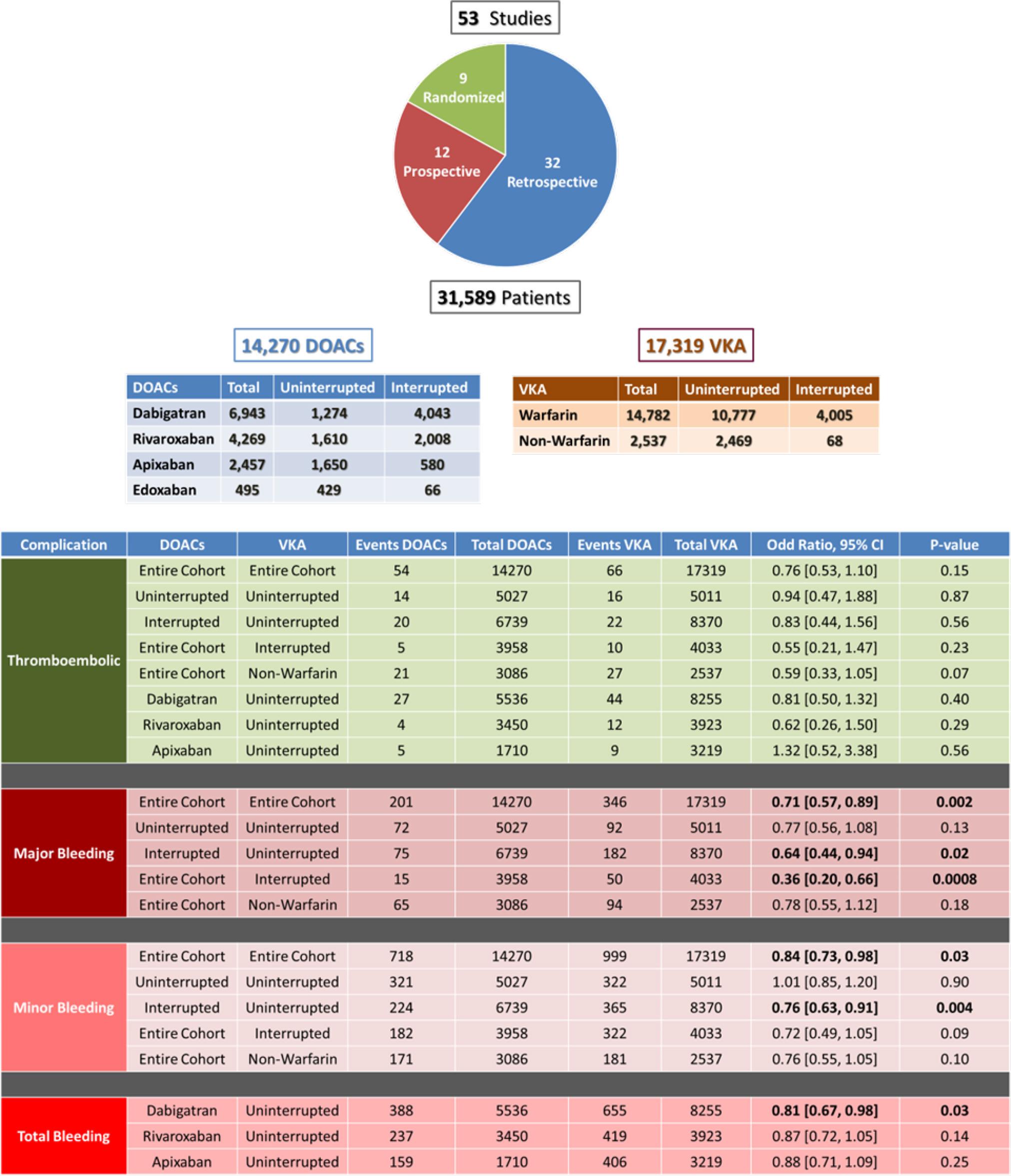
Central Figure.
The 53 studies included 31589 patients of which 14270 patients were on DOACS [6943 (49%) on D, 4269 (30 %) on R, 2457 (17%) on A and 495 (3%) on E] and 17319 were on VKA [13246 (76 %) uninterrupted, 2469 (14%) non-warfarin VKA]. In some studies, lower doses of D (110 mg vs 150 mg)26,35,51,60 and R (15 mg and 10 mg vs 20 mg)37,60 were used as recommended by the health systems of specific countries. The characteristics of the studies are shown in Table 1. The majority of the studies (32 studies) were retrospective series, including 3 case-matched and one survey; the other 21 were prospective studies, including 9 randomized trials and one case-matched. There were 13 multicenter studies with up to 104 participating centers and a survey with data from 179 sites. A funnel plot used to assess the potential for publication bias in the dataset showed no evidence of significant bias.67 (Figure 2)
Studies’ Characteristics.
| No. | Author Journal, Year | Year | No. of centers | Study period | Type of study | GRADE Quality Rating | Number of patients | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | DOAC | D | R | A | E | UVKA | IVKA | |||||||
| 1 | Armbruster HL et al. Annals of Pharm 2015 | 2015 | 1 | Jan 2012-Dec 2013 | Retrospective analysis | Moderate | 374 | 201 | 123 | 61 | 17 | 173 | ||
| 2 | Arshad A et al. PACE 2014 | 2014 | 4 | Oct 2010-Oct 2012 | Retrospective analysis | Moderate | 882 | 374 | 374 | 276 | 232 | |||
| 3 | Bassiouny M et al. Circ Arrhythmia EP 2013 | 2013 | 1 | Dec 2010-Jul 2012 | Prospective registry | Moderate | 999 | 376 | 376 | 623 | ||||
| 4 | Calkins H et al. NEJM 2017 | 2017 | 104 | April 2015-July 2016 | Prospective randomized | High | 635 | 317 | 317 | 318 | ||||
| 5 | Cappato R et al. European Heart Journal 2015 | 2015 | 37 | Feb 2013-Sep 2014 | Prospective randomized | High | 248 | 124 | 124 | 124 | ||||
| 6 | De Heide J et al. J Int Card Electrophys 2018 | 2018 | 1 | Jan 2013-Apr 2017 | Retrospective analysis | Low | 637 | 117 | 68 | 14 | 30 | 5 | 520 | |
| 7 | DiBiase L et al. Heart Rhythm 2015 | 2015 | 4 | June 2013-July 2014 | Prospective match cohort | High | 400 | 200 | 200 | 200 | ||||
| 8 | Dillier R et al. Circ Arrhythmia EP 2014 | 2014 | 1 | Feb 2012 May 2013 | Retrospective analysis-matched | Moderate | 544 | 272 | 272 | 272 | ||||
| 9 | Efremidis M et al. J of Electrocardiology 2015 | 2015 | 1 | June 2013-Sep 2014 | Prospective registry | Moderate | 149 | 64 | 64 | 85 | ||||
| 10 | Enriquez AD et al. PACE 2017 | 2017 | 1 | Jan 2013-Nov 2014 | Retrospective analysis | Low | 471 | 258 | 258 | 213 | ||||
| 11 | Garcia LI et al. J Afib 2014 | 2014 | 1 | Jul 2011-Oct 2012 | Retrospective analysis | Low | 325 | 126 | 126 | 199 | ||||
| 12 | Gjermeni D et al. European Heart Journal 2023 | 2023 | 1 | Jan 2011 May 2017 | Retrospective analysis | Moderate | 2219 | 1290 | 697 | 399 | 194 | 929 | ||
| 13 | Gunawardene et al. Clin Res Cardiol 2017 | 2017 | 1 | Jan 2011-Dec 2014 | Retrospective analysis | Moderate | 1440 | 441 | 147 | 253 | 41 | 488 | 511 | |
| 14 | Haines DE et al. J Int Card Electrophys 2013 | 2013 | 4 | Nov 2010-Nov 2011 | Retrospective analysis | Low | 404 | 202 | 202 | 162 | 40 | |||
| 15 | Hohnloser SH et al. European Heart Journal 2019 | 2019 | 58 | March 2017-Sep 2018 | Prospective randomized | High | 553 | 375 | 375 | 178 | ||||
| 16 | Ichiki H et al. PACE 2013 | 2013 | 1 | Apr 2010-Jul 2012 | Prospective registry | Low | 237 | 36 | 36 | 201 | ||||
| 17 | Imamura K et al. J Int Card Electrophys 2013 | 2013 | 1 | Apr 2011-Nov 2012 | Prospective analysis | Moderate | 227 | 101 | 101 | 126 | ||||
| 18 | Kaess BM at al. Am J Cardiol 2015 | 2015 | 1 | Mar 2014 | Retrospective case matched | Moderate | 315 | 105 | 105 | 210 | ||||
| 19 | Kaiser D et al. J Int Card Electrophys 2013 | 2013 | 1 | Jan 2011-Aug 2012 | Retrospective analysis | Low | 257 | 122 | 122 | 135 | ||||
| 20 | Kaseno K et al. Circ Journal Jap 2012 | 2012 | 1 | Apr 2011-Jan 2012 | Retrospective analysis | Moderate | 211 | 110 | 110 | 101 | ||||
| 21 | Kim JS et al. Heart Rhythm 2013 | 2013 | 1 | Jan 2011-Aug 2012 | Case-control analysis | Moderate | 763 | 191 | 191 | 572 | ||||
| 22 | Kimura T et al. JACC 2018 | 2018 | 2 | Jul 2014-Jan 2016 | Prospective randomized | High | 127 | 64 | 64 | 63 | ||||
| 23 | Kirchhof P et al. European Heart Journal 2018 | 2018 | 49 | Feb 2015-Apr 2017 | Prospective randomized | High | 633 | 318 | 318 | 315 | ||||
| 24 | Kochhauser S et al. Can J of Card 2014 | 2014 | 1 | Oct 2010-Oct 2013 | Retrospective analysis | Moderate | 680 | 361 | 220 | 141 | 319 | |||
| 25 | Koetkuerk B et al. Cardiovasc Therap 2016 | 2016 | 1 | Aug 2012 May 2015 | Retrospective analysis | Moderate | 409 | 259 | 48 | 193 | 18 | 150 | ||
| 26 | Konduru SV et al. J Int Card Electrophys 2012 | 2012 | 1 | Jan 2011-Aug 2011 | Retrospective analysis | Moderate | 76 | 24 | 24 | 52 | ||||
| 27 | Kuwahara T et al. J of Card Electrophys 2016 | 2016 | 3 | NR | Prospective randomized | High | 200 | 100 | 100 | 100 | ||||
| 28 | Lakkireddy D et al. JACC 2012 | 2012 | 8 | Jan 2010-Jul 2011 | Prospective registry | Moderate | 290 | 145 | 145 | 145 | ||||
| 29 | Lakkireddy D et al. JACC 2014 | 2014 | 8 | Jan 2012-Mar 2013 | Prospective registry | Moderate | 642 | 321 | 321 | 321 | ||||
| 30 | Lin J et al. J Afib 2014 | 2014 | 1 | Jan 2010-Dec 2012 | Retrospective analysis | Low | 324 | 181 | 181 | 143 | ||||
| 31 | Maddox W et al. J Card Electrophysiol 2013 | 2013 | 1 | Nov 2010-Jan 2012 | Retrospective analysis | Low | 463 | 212 | 212 | 251 | ||||
| 32 | Mugnai G et al. American J of Card 2017 | 2017 | 2 | Jun 2013-Sep 2015 | Retrospective analysis | Moderate | 454 | 164 | 60 | 71 | 33 | 290 | ||
| 33 | Muller P et al. J Interv Card Electro 2016 | 2016 | 1 | NR | Prospective cohort | Moderate | 192 | 106 | 43 | 43 | ||||
| 34 | Murakawa Y et al. J of Arrhythmia 2015 | 2015 | 179 | Sep 2011-Sep2012 | Retrospective survey | Low | 2349 | 541 | 504 | 37 | 1808 | |||
| 35 | Nagao T et al. Heart Rhythm 2015 | 2015 | 1 | April 2012 Aug 2014 | Retrospective analysis | Moderate | 869 | 499 | 239 | 102 | 158 | 370 | ||
| 36 | Nagao T et al. PACE 2015 | 2015 | 1 | April 2013 Mar 2014 | Retrospective analysis | Moderate | 342 | 105 | 105 | 237 | ||||
| 37 | Nagao T et al. Internal Med 2015 | 2015 | 1 | April 2012 Nov 2013 | Retrospective analysis | Moderate | 363 | 173 | 173 | 190 | ||||
| 38 | Nin T et al. PACE 2013 | 2013 | 1 | Apr 2011 May 2012 | Prospective randomized | High | 90 | 44 | 44 | 46 | ||||
| 39 | Nogami A et al. JAMA 2019 | 2019 | 28 | May 2014-Sep 2015 | Prospective randomized | High | 442 | 220 | 220 | 222 | ||||
| 40 | Okishige K et al. J of Card 2017 | 2017 | 1 | NR | Prospective registry | Moderate | 257 | 238 | 66 | 81 | 30 | 61 | 19 | |
| 41 | Reynolds MR et al. JACC EP 2018 | 2018 | 18 | Dec 2015-Jan 2017 | Retrospective analysis | Moderate | 590 | 295 | 295 | 295 | ||||
| 42 | Rilling A et al. JCE 2016 | 2016 | 1 | Oct 2013-Oct 2014 | Prospective registry | Moderate | 444 | 324 | 51 | 193 | 80 | 120 | ||
| 43 | Snipelisky D et al. J Int Card Electrophys 2012 | 2012 | 1 | Jan 2011-Dec 2011 | Retrospective analysis | Low | 156 | 31 | 31 | 125 | ||||
| 44 | Snipelisky D et al. J Int Card Electrophys 2014 | 2014 | 1 | Jan 2011 -2014 | Retrospective analysis | Moderate | 217 | 130 | 90 | 40 | 87 | |||
| 45 | Somani R et al. Cardiovasc Therap 2014 | 2014 | 1 | Nov 2010-Jan 2012 | Retrospective analysis | Moderate | 207 | 43 | 43 | 95 | 69 | |||
| 46 | Stepanyan G et al. J Int Card Electrophys 2014 | 2014 | 1 | Jan 2011-Sep 2013 | Retrospective analysis | Moderate | 301 | 187 | 89 | 98 | 114 | |||
| 47 | Tang l et al. Frontiers in Med 2020 | 2020 | 1 | Jan 2010-Dec 2018 | Retrospective analysis | Low | 4520 | 1876 | 865 | 1011 | 796 | 1848 | ||
| 48 | Tao S et al. J Int Card Electroph 2017 | 2017 | 1 | Nov 2012-Mar 2014 | Prospective cohort | Moderate | 147 | 76 | 76 | 71 | ||||
| 49 | Tscholl V et al. Clinical Cardio 2017 | 2017 | 1 | NR | Retrospective analysis | Low | 200 | 153 | 31 | 67 | 55 | 47 | ||
| 50 | Vlachos K et al. Clinical Cardio 2017 | 2017 | 1 | June 2013-Dec 2016 | Prospective cohort | Moderate | 474 | 338 | 114 | 110 | 114 | 136 | ||
| 51 | Yamaji H et al. Clin Drug Inv 2013 | 2013 | 1 | Mar 2009-Dec 2011 | Retrospective analysis | Moderate | 503 | 106 | 106 | 203 | 194 | |||
| 52 | Yanagisawa S et al. JACC Clin Electrpph 2018 | 2018 | 1 | Jan 2009-Jun 2017 | Retrospective analysis | Moderate | 2164 | 1129 | 333 | 228 | 514 | 54 | 1035 | |
| 53 | Yoshimura et al. Journal of Card 2017 | 2017 | 1 | Mar 2013-Dec 2014 | Prospective randomized | High | 174 | 105 | 55 | 50 | 69 | |||
The clinical baseline characteristics of the studied patients are displayed in Table 2.
Patients Baseline Characteristics, *p value < 0.05; W – warfarin; BMI – body mass index; TIA - transient ischemic attack; LVEF – left ventricular ejection fraction; LA – left atrium; NR – not reported.
| No. | Author | Age (yrs) | Male (%) | BMI | Prior stroke/TIA (%) | CHADS2 | CHA2DS2-VASc | Parox AF (%) | LVEF (%) | LA dimension | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DOAC | VKA | DOAC | VKA | DOAC | VKA | DOAC | VKA | DOAC | VKA | DOAC | VKA | DOAC | VKA | DOAC | VKA | DOAC | VKA | ||
| 1 | Armbruster HL et al. | 60 ± 10 | 64 ± 10* | 76 | 72 | 30 ± 6 | 29 ± 7 | 6 | 11 | NR | NR | ≥ 2 - 51 % | ≥ 2 - 66 % | NR | NR | NR | NR | NR | NR |
| 2 | Arshad A et al. | 61 ± 12 | 62 ± 11 | 71 | 67 | 29 ± 6 | 31 ± 6* | 10 | 8 | 1.1 ± 1.1 | 1.3 ± 1.2* | NR | NR | 56 | 60 | 56 ± 10 | 55 ± 10 | 45 ± 9 mm | 44 ± 8 mm |
| 3 | Bassiouny M et al. | 59 ± 11 | 63 ± 10* | 75 | 73 | 30 ± 5 | 31 ± 6 | 6 | 8 | ≥ 2 - 20 % | ≥ 2 - 29 %* | NR | NR | 57 | 55 | 55 | 55 | 32 ml/m2 | 34 ml/m2 |
| 4 | Calkins H et al | 59 ± 10 | 59 ± 10 | 73 | 77 | 29 | 29 | 3 | 3 | NR | NR | 2 | 2.2 | 67 | 69 | NR | NR | NR | NR |
| 5 | Cappato et al. | 59 ± 10 | 60 ± 10 | 69 | 73 | 30 ± 6 | 29 ± 6 | 0 | 2 | 0.7 + 0.7 | 0.8 ± 0.9 | 1.5 ± 1.3 | 1.5 ± 1.3 | 77 | 70 | NR | NR | NR | NR |
| 6 | DiBiasi L et al. | 66 ± 10 | 66 ± 10 | 71.5 | 71.5 | 29 ± 6 | 30 ± 6 | 6 | 5 | 1.3 ± 0.9 | 1.3 ± 0.8 | 2.3 ± 1.4 | 2.3 ± 1.4 | 16.5 | 16.5 | 56 ± 9 | 57 ± 11 | 45 ± 8 mm | 45 ± 9 mm |
| 7 | De Heide J et al. | 60 ± 9 | 60 ± 10 | 72 | 68 | 27 ± 3 | 28 ± 4 | NR | NR | NR | NR | ≥ 2 - 34 % | ≥ 2 - 47 % | 74 | 76 | NR | NR | 43 ± 7 | 42 ± 6 |
| 8 | Dillier R at al. | 62 ± 11 | 64 ± 10 | 68 | 68 | 27 ± 4 | 27 ±4 | 6 | 7 | 0.9 ± 0.8 | 1.0 ± 0.9 | 1.8 ± 1.4 | 2.0 ± 1.5 | 49 | 46 | 60 ± 37 | 56 ± 7 | 44 ± 6 | 45 ± 7 |
| 9 | Efremidis et al. | 57 ± 12 | 58 ± 9 | 70 | 69 | 27 ± 3 | 27 ± 3 | NR | NR | 0.7 ± 0.8 | 0.8 ± 0.9 | 1.1 ± 1.1 | 1.2 ± 1.2 | 65 | 63 | 61 ± 6 | 59 ± 6 | NR | NR |
| 10 | Enriquez AD et al | 61 ± 10 | 60 ± 10 | 71 | 72 | NR | NR | NR | NR | NR | NR | 1.6 ± 1.4 | 1.9 ± 1.3 | 65 | 53 | NR | NR | NR | NR |
| 11 | Garcia LI et al. | 62 (55-69) | 65 (58-72)* | 72 | 66 | 31 ± 6 | 30 ± 7 | 9 | 19 | 0.98 ± 1.5 | 1.2 ± 1.4* | 2.1 ± 0.3 | 2.7 ± 0.2* | 28 | 29 | 57 ± 10 | 55 ± 10 | NR | NR |
| 12 | Gjermeni D. et al. | 62 ± 10 | 65 ± 10 | 69 | 64 | 28 ± 5 | 29 ± 7 | 7 | 10 | NR | NR | ≥ 2 - 42 % | ≥ 2 - 58 % | 76 | 65 | NR | NR | NR | NR |
| 13 | Gunawardene el al. | 64 ± 10 | 64 ± 10 | 71 | 66 | 27 ± 4 | 27 ± 4 | 9 | 12 | 1 (1;2) | 1 (1;2) | 2 (1;3) | 2 (1;3) | 0 | 0 | 57 ± 8 | 58 ± 8 | NR | NR |
| 14 | Haines DE et al. | 60 ± 10 | 60 ± 11 | 74 | 69 | NR | NR | 7 | 9 | NR | NR | 1.6 ± 1.3 | 1.9 ± 1.4 | 58 | 52 | 56 ± 10 | 57 ± 9 | 44 ± 7 mm | 44 ± 9 mm |
| 15 | Hohnloser SH et al. | 60 (53-67) | 61 (52-67) | 71 | 73 | 28(25–31) | 28(26–31) | 5 | 5 | NR | NR | ≥ 2 - 50 % | ≥ 2 - 50 % | 68 | 69 | NR | NR | NR | NR |
| 16 | Ichiki H et al. | 57 ± 11 | 60 ± 10 | 83 | 78 | NR | NR | NR | NR | 1.1 ± 1.1 | 1.0 ± 1.0 | NR | NR | 70 | 50* | 65 ± 8 | 64 ± 11 | 65 ± 24 ml/m2 | 70 ± 24 ml/m2 |
| 17 | Imamura K et al. | 61 ± 10 | 62 ± 8 | 75 | 71 | NR | NR | 6 | 8 | 0.9 ± 0.9 | 1.1 ± 1.0 | 1.6 ± 1.2 | 1.8 ± 1.2 | 56 | 49 | 63 ± 8 | 62 ± 9 | 41 ± 7 mm | 42 ± 7 mm |
| 18 | Kaess BM et al. | 63 ± 12 | 64 ± 10 | 67 | 67 | 27 ± 5 | 27 ± 4 | 8 | 7 | 1.2 ± 1.1 | 1.0 ± 0.9 | 2.1 ± 1.8 | 2.0 ± 1.5 | 54 | 54 | 58 ± 7 | 56 ± 6 | 44 (39,49) | 44 (40,49) |
| 19 | Kaiser D et al. | 58 ± 11 | 64 ± 10* | 64 | 68 | 31 ± 6 | 31 ± 6 | 7 | 6 | 1.2 ± 1 | 1.6 ± 1* | 1.8 ± 1.4 | 2.5 ± 1.4* | 69* | 47 | 62 ± 8* | 59 ± 11 | 38 ± 9 mm | 43 ± 8 mm |
| 20 | Kaseno K et al. | 59 ± 10 | 62 ± 8 | 75 | 79 | 24 ± 3 | 24 ± 4 | 4 | 5 | ≥ 2 - 8% | ≥ 2 - 14% | NR | NR | 83* | 55 | 64 ± 10 | 63 ± 10 | 39 ± 6 mm | 43 ± 7 mm |
| 21 | Kim JS et al. | 61 ± 10 | 61 ± 10 | 80 | 74 | 31 ± 6 | 32 ± 6 | 3 | 8 | 1.0 ± 0.9 | 1.1 ± 1.0 | 1.6 ± 1.3 | 1.7 ± 1.3 | 53 | 48 | 58 ± 9 | 57 ± 11 | 43 ± 7 mm | 44 ± 7 mm |
| 22 | Kimura T et al. | 59 (52-65) | 62 (53-67) | 53 | 53 | 24(22–25) | 24(22–26) | NR | NR | NR | NR | NR | NR | 63 | 67 | 56(51-58) | 56(52-57) | 39 (35-42.5) | 37 (33-43) mm |
| 23 | Kirchhof P et al. | 64 (57,70) | 64 (58,70) | 69 | 65 | 28(25,32) | 28(26,32) | 7.5 | 7.3 | NR | NR | 2.4(1.2) | 2.4(1.2) | NR | NR | NR | NR | NR | NR |
| 24 | Kochhauser S et al. | 60 ± 10 | 62 ± 11 | 76 | 73 | NR | NR | NR | NR | 0.9 ± 0.6 | 0.8 ± 0.5 | 1.5 ± 0.8 | 1.4 ± 0.8 | 74 | 69 | NR | NR | 41 ± 5 mm | 42 ± 6 mm |
| 25 | Koetkuerk B et al. | 61 ± 10 | 62 ± 10 | 62 | 53 | NR | NR | NR | NR | NR | NR | 1.5 ± 1.0 | 2.1 ± 1.5 | 62* | 47 | 61 ± 10 | 58 ± 9 | 33 ± 11 mm | 35 ± 13 mm |
| 26 | Konduru SV et al. | 57 ± 10 | 61 ± 10 | 79 | 67 | NR | NR | 0 | 0 | NR | NR | NR | NR | 79 | 56 | NR | NR | NR | NR |
| 27 | Kuwahara T et al. | 65 ± 9 | 66 ± 8 | 75 | 72 | NR | NR | NR | NR | NR | NR | 2.1 ± 1.3 | 2.4 ± 1.4 | 59 | 60 | 64 ± 9 | 62 ± 9 | 41 ± 7 mm | 42 ± 6 mm |
| 28 | Lakkireddy D at al. | 60 ± 10 | 60 ± 10 | 79 | 79 | NR | NR | 3 | 6 | ≥ 2 - 23% | ≥ 2 - 19% | 1.6 ± 1.4 | 1.5 ± 1.3 | 57 | 57 | 56 ± 10 | 56 ± 10 | 45 ± 25 mm | 44 ± 8 mm |
| 29 | Lakkireddy D et al. | 63 ± 10 | 63 ± 10 | 69 | 69 | 30 ± 6 | 30 ± 6 | 11 | 8 | 1.2 ± 1 | 1.2 ± 1 | 2.2 ± 1.6 | 2.2 ± .2 | 51 | 51 | 58 ± 8 | 57 ± 8 | 44 ± 8 mm | 43 ± 8 mm |
| 30 | Lin J et al. | 60 ± 9 | 60 ± 10 | 80 | 75 | NR | NR | 5 | 8 | ≥ 2 - 13% | ≥ 2 - 25%* | NR | NR | 75 | 69 | NR | NR | NR | NR |
| 31 | Maddox W et al. | 62 ± 12 | 63 ± 10 | 76* | 67 | NR | NR | 4 | 4 | 0.9 ± 0.9 | 0.9 ± 0.9 | 1.7 ± 1.5 | 1.7 ± 1.3 | 63 | 57 | 53 ± 4 | 54 ± 5 | NR | NR |
| 32 | Mugnai G et al. | 63 ± 10* | 59 ± 11 | 72 | 71 | 27 ± 4 | 27 ± 5 | NR | NR | NR | NR | 1.8 ± 1.3 | 1.5 ± 1.3 | NR | NR | 57 ± 9 | 58 ± 7 | 44 ± 9 mm | 44 ± 9 mm |
| 33 | Muller P et al. | 63 ± 1 | 64 ± 2 | 64 | 58 | NR | NR | 5 | 10 | NR | NR | 2.3 ± .2 | 2.2 ± 1.3 | 44 | 58 | 58 ± 1 | 57 ± 1 | 44 ± 1 mm | 44 ± 1 mm |
| 34 | Murakawa Y et al. | 60 ± 11 | 63 ± 10* | 76 | 76 | NR | NR | NR | NR | NR | NR | 1.5 ± 1.3 | 1.9 ± 1.5* | 70* | 61 | 65 ± 9* | 63 ± 10 | 40 ± 6 mm | 41 ± 6* mm |
| 35 | Nagao T et al. | 60 ± 12 | 61 ± 11 | 74 | 74 | 24 ± 3 | 24 ± 3 | 5 | 5 | 0.8 ± 1 | 0.8 ± 0.9 | 1.5 ± 1.5 | 1.5 ± 1.5 | 75 | 73 | 62 ± 8 | 61 ± 9 | 39 ± 7 mm | 40 ± 7 mm |
| 36 | Nagao T et al. | 61 ± 13 | 62 ± 8 | 73 | 73 | 24 ± 4 | 24 ± 4 | 6 | 6 | 0.8 ± 1.1 | 0.8 ± 0.9 | NR | NR | 76 | 81 | 62 ± 9 | 62 ± 9 | 37 ± 6 mm | 40 ± 2 mm |
| 37 | Nagao T et al. | 59 ± 13 | 59 ± 9 | 77 | 77 | 24 ± 4 | 24 ± 3 | 4 | 5 | 0.6 ± 0.9 | 0.7 ± 0.9 | 1.2 ± 1.2 | 1.3 ± 1.4 | 72 | 64 | 62 ± 7 | 61 ± 7 | 38 ± 6 mm | 39 ± 7 mm |
| 38 | Nin T et al.36 | 61 ± 11 | 61 ± 6 | 84 | 80 | 24 ± 4 | 24 ± 3 | 4 | 11 | ≥ 2 - 18% | ≥ 2 - 20% | NR | NR | 76 | 71 | 61 ± 7 | 62 ± 8 | 39 ± 7 mm | 40 ± 8 mm |
| 39 | Nogami A et al. | 65(59-71) | 66(59-71) | 78 | 72 | 24(22-26) | 24(22-26) | 7 | 5 | NR | NR | 2 (1-3) | 2 (1-3) | 63 | 62 | 66(60-71) | 65(60-70) | NR | NR |
| 40 | Okishige K et al. | 64 ± 12 | 65 ± 11 | 68 | 74 | 24 | 25 | NR | NR | 1 ± 1 | 1.9 ± 1* | NR | NR | NR | NR | 64 ± 10 | 68 ± 8 | 40 ± 7 mm | 42 ± 6 mm |
| 41 | Reynolds MR et al. | 64 ± 10 | 64 ± 10 | 67 | 68 | 31 ± 6 | 32 ± 7* | 3 | 5 | NR | NR | 2.3 ± 1.6 | 2.6 ± 1.5 | 65 | 64 | 57 ± 9 | 55 ± 10 | NR | NR |
| 42 | Rilling A et al. | 65 ± 10 | 67 ± 11 | 58 | 66 | 28 ± 14 | 28 ± 4 | 7 | 11 | NR | NR | 2 (1,3) | 3 (2,4)* | 40 | 43 | NR | NR | NR | NR |
| 43 | Snipelisky D et al. | 61 | 65 | 81 | 74 | NR | NR | NR | NR | 0.84 | 1.22 | NR | NR | 68 | 46 | NR | NR | NR | NR |
| 44 | Snipelisky D et al. | 66 | 66 | 69 | 62 | 29 | 30 | 8 | 5 | 1 | 1.4 | NR | NR | NR | NR | NR | NR | NR | NR |
| 45 | Somani R et al. | 60 ± 10 | 62 ± 8 | 84 | 77 | NR | NR | 2 | 7 | 0.6 ± 0.7 | 0.8 ± 0.9 | NR | NR | 70 | 66 | NR | NR | 34 ± 13 ml/m2 | 39 ± 12 ml/m2 |
| 46 | Stepanyan G et al. | 60 ± 11 | 63 ± 10 | 62 | 67 | NR | NR | 7 | 10 | ≥ 2 - 7% | ≥ 2 - 7% | NR | NR | 77* | 63 | NR | NR | NR | NR |
| 47 | Tang l et al. | 59 ± 11 | 58 ± 11 | 66 | 66 | NR | NR | 7 | 6 | NR | NR | ≥ 2 - 44 % | ≥ 2 - 43 % | 80 | 79 | NR | NR | NR | NR |
| 48 | Tao S et al. | 66 ± 9 | 66 ± 11 | 74 | 66 | 24 ± 4 | 24 ± 4 | 11 | 7 | 1.3 ± 1 | 1.5 ± 1.1 | 2.2 ± 1.3 | 2.5 ± 1.5 | 72 | 77 | 67 ± 8 | 64 ± 11 | 40 ± 5 mm | 41 ± 6 mm |
| 49 | Tscholl V et al. | 63 ± 1 | 68 ± 9* | 59 | 47 | 28 ± 6 | 30 ± 5 | 6 | 4 | NR | NR | 2.6 ± 1.7 | 3.1 ± 1.2 | 53 | 38 | 64 ± 8 | 64 ± 7 | 43 ± 3 mm | 42 ± 7 mm |
| 50 | Vlanchos K et al. | 58 ± 12 | 59 ± 10 | 68 | 70 | 28 ± 14 | 32 ± 40 | NR | NR | NR | NR | 1.3 ± 1.2 | 1.4 ± 1.1 | 65 | 58 | 60 ± 7 | 59 ± 7 | NR | NR |
| 51 | Yamaji H et al. | 60 ± 8 | 62 ± 8 | 75 | 76 | NR | NR | 5 | 4 | NR | NR | 1.8 ± 1.6 | 1.7 ± 1.5 | 65 | 62 | 60 ± 6 | 60 ± 8 | 43 ± 6 mm | 41 ± 5 mm |
| 52 | Yanagisawa et al. | 63 ± 8 | 63 ± 8 | 73 | 75 | 24 ± 5 | 24 ± 4 | 7 | 9 | 1.1 ± 1 | 1.1 ± 1 | 1.9 ± 1.3 | 1.9 ± 1.2 | 68 | 68 | 62 ± 8 | 60 ± 10 | 39 ± 7 mm | 40 ± 7 mm |
| 53 | Yoshimura et al. | 59 ± 11 | 61 ± 8 | 82 | 75 | 24 ± 4 | 25 ± 4 | 14 | 10 | 1.1 ± 1.1 | 1.0 ± 1.0 | 1.7 ± 1.4 | 1.5 ± 1.3 | 61 | 51 | 64 ± 9 | 64 ± 9 | 42 ± 6 mm | 44 ± 6 mm |
In general, the patients included in the studies were relatively young (DOACS 61 ± 10 years vs VKA 62 ± 10 years), with only 6 studies having older patients in the VKA group, and one study with older patients in the DOACS group. There was a male predominance (DOACS 72% vs VKA 70%), with the majority of the patients having a CHADS2 and CHA2DS2VASc score less than 2, and only a few studies indicating that the VKA group had a slightly higher score. The majority of patients had paroxysmal atrial fibrillation, with 6 studies indicating that DOACS had a higher percentage of paroxysmal atrial fibrillation than VKA, with only three series enrolling mostly non-paroxysmal atrial fibrillation24,28,30. In the series that reported, the left ventricular function was normal with a mildly to moderately enlarged left atrium.
The anticoagulation was usually started 3-4 weeks before the procedure, with the uninterrupted VKA group targeting an INR of 2-3 on the day of ablation. In the interrupted group, the VKA was usually stopped 3-5 days prior, and either unfractionated heparin or low molecular weight heparin was used for bridging, which was continued after the procedure until the INR was therapeutic. The period for which the DOACS were stopped before the procedure varied among the studies: 21 studies14,17,21,22,24,25,27,33,37,38,41,42,44,46,48–50,54,62,64,65 included 5027 patients using an uninterrupted DOACS regimen, 31 studies13,18–20,23,26,28,30,31,34–36,39,40,42,43,45–47,51–55,58–63,65 included 77691 patients for whom the DOACS were interrupted, including 15 studies18,19,28,30,31,34–36,39,43,45,51,55,58,59 with 3071 patients for whom the DOACS were stopped > 24h before the procedure. The rest of the studies had variations in the time DOACS were held, but the majority were held 12-48 hours before the procedure. There was usually no heparin bridging when the DOACS were interrupted. In the majority of studies, DOACS were resumed a few hours after hemostasis or the night of the procedure, with a smaller number the next morning; in the vast majority of cases, DOACS were restarted within 24 hours post-procedure, with only a minority of studies reporting the use of short heparin bridging. (Table 3)
Anticoagulation Characteristics; D – dabigatran; R – rivaroxaban; W – warfarin; N/A -not applicable; NR – not reported; CW – continuous warfarin; TEE – transesophageal echocardiogram; UFH – unfractionated heparin; LMWH – low molecular weight heparin
| No. | Author | Pre procedure anticoagulation | Antiplatelets (%) | DOAC | VKA Type | VKA bridging protocol | INR (CVKA) | Pre-procedureTEE | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DOAC | VKA | DOAC | VKA | Stop pre | Start post | Pre | Post | DOAC | VKA | ||||
| 1 | Armbruster HL et al. Annals of Pharm 2015 | NR | NR | 20 | 27 | 3 doses D 1-2 doses R | 4h post procedure | Warfarin | Uninterrupted | 2.6 ± 0.7 | For persistent AF | For persistent AF | |
| 2 | Arshad A et al. PACE 2014 | ≥ 4 weeks | ≥ 4 weeks | 28.6* | 16.1 | 12-48 h | Evening of procedure | Warfarin | Uninterrupted or W stopped 5 days with LMWH | W night of procedure; LMWH 0.5-0.6 mg/kg | 2.4 ± 0.4 | TEE at 3/4 centers; as needed 1/4 centers | TEE at 3/4 centers;as needed 1/4 centers |
| 3 | Bassiouny M et al. Circ Arrhythmia EP 2013 | ≥ 4 weeks | ≥ 4 weeks | 33 | 39* | 12-24 h | Immediate post-procedure | Warfarin | Uninterrupted | 2.4 | As needed 12% | As needed 25%* | |
| 4 | Calkins H et al. NEJM 2017 | ≥ 4 weeks | ≥ 4 weeks | 19 | 23 | Uninterrupted | Uninterrupted | Warfarin | Uninterrupted | 2.3 | 100% | 100% | |
| 5 | Cappato R et al. European Heart Journal 2015 | ≥ 3 weeks or 1-7 days - TEE or ICE | ≥ 3 weeks or 1-7 days - TEE or ICE | 30 | 23 | Uninterrupted | VKA | Uninterrupted | NR | If necessary | If necessary | ||
| 6 | De Heide J et al. J Int Card Electrophys 2018 | ≥ 3 weeks | ≥ 3 weeks | NR | NR | >24h; 1-2 doses held | Evening of procedure | Marcoumar Acenocoumarol | Uninterrupted | NR | 100% | 100% | |
| 7 | DiBiase L et al. Heart Rhythm 2015 | ≥ 3 weeks | ≥ 3 weeks | 30.5 | 38.5 | Uninterrupted | Uninterrupted | Warfarin | Uninterrupted | 2.5 ± 0.5 | Not mandated | Patients in AF and INR < 2.0 | |
| 8 | Dillier R et al. Circ Arrhythmia EP 2014 | ≥ 4 weeks | ≥ 4 weeks | 16 | 15 | Uninterrupted | 12- 22 h | Phenprocoumon | Uninterrupted | 2.1 ± 0.4 | 100% TEE or CT | 100% TEE or CT | |
| 9 | Efremidis M et al. J of Electrocardiology 2015 | ≥ 3 weeks | ≥ 3 weeks | NR | NR | 24h | Immediate post-procedure | Acenocoumarol | Uninterrupted | 2.4 ± 0.2 | 100% | 100% | |
| 10 | Enriquez AD et al. PACE 2017 | NR | NR | NR | NR | Uninterrupted | Uninterrupted | Warfarin | Uninterrupted | 2.3 ± 0.4 | NR | NR | |
| 11 | Garcia LI et al. J Afib 2014 | NR | NR | 15 | 23 | 96 h | Next AM with LMWH 0.5 mg/kg × 3 doses; UFH IV 4-6h post | Warfarin | Uninterrupted | 2.2 (1.8-2.5) | 100% | 100% | |
| 12 | Gjermeni D et al. European Heart Journal 2023 | NR | NR | NR | NR | <48h (prior to 2015) post 2015- uninterrupted | Evening of procedure | Phenprocoumon | Uninterrupted | NR | At physician discretion | At physician discretion | |
| 13 | Gunawardene et al. Clin Res Cardiol 2017 | NR | NR | NR | NR | 48 h | Evening of procedure | VKA | Uninterrupted or LMWH | Uninterrupted or LMWH | NR | 100% | 100% |
| 14 | Haines DE et al. J Int Card Electrophys 2013 | NR | NR | 65 | 47 | <12-48 h 22% bridge LMWH | 12 ± 10 h | Warfarin | Uninterrupted in 80% LMWH bridge | LMWH | 2.3 ± 0.7 | Pts not on continuous AC | Pts not on continuous AC |
| 15 | Hohnloser SH et al. European Heart Journal 2019 | ≥ 3 weeks | ≥ 3 weeks | NR | NR | Uninterrupted | Uninterrupted | VKA | Uninterrupted | NR | 100% TEE or ICE | 100% TEE or ICE | |
| 16 | Ichiki H et al. PACE 2013 | NR | NR | NR | NR | Morning of procedure | Evening of procedure | Warfarin | Uninterrupted | 1.99 ± 0.6 | 100% | 100% | |
| 17 | Imamura K et al. J Int Card Electrophys 2013 | ≥ 4 weeks | ≥ 4 weeks | 8 | 7 | 24 h for CHADS 0-1; 12 h CHADS >1 | 3h post-procedure | Warfarin | W stopped 3 days; UFH bridge | UFH + W 3 h post procedure | N/A | 100% | 100% |
| 18 | Kaess BM at al. Am J Cardiol 2015 | ≥ 4 weeks | ≥ 4 weeks | 22 | 15 | Uninterrupted | Uninterrupted | Phenprocoumon | Uninterrupted | 2.1 ± 0.4 | 100% TEE or CT | 100% TEE or CT | |
| 19 | Kaiser D et al. J Int Card Electrophys 2013 | NR | NR | 58 | 51 | 24-30 h CrCl > 50 ml/min 3-5 days CrCl 15-30 ml/min | Immediate post-procedure | Warfarin | Uninterrupted | Uninterrupted; 24% UFH bridge | ≥ 1.5 | S-TEE per operator; AF-TEE 100% | AF-TEE 100% |
| 20 | Kaseno K et al. Circ Journal Jap 2012 | 26 ± 43 days | ≥ 4 weeks | NR | NR | Morning of procedure | Morning after procedure 10000 UFH first 24h | Warfarin | Uninterrupted | Uninterrupted + 10000 UFH first 24h | 2.4 ± 0.4 | 100% | 100% |
| 21 | Kim JS et al. Heart Rhythm 2013 | ≥ 4 weeks | ≥ 4 weeks | 36 | 43 | 24-30 h | Immediate post-procedure | Warfarin | Uninterrupted | 2.4 ± 0.3 | 100% | 100% | |
| 22 | Kimura T et al. JACC 2018 | ≥ 4 weeks | ≥ 4 weeks | NR | NR | Uninterrupted | Uninterrupted | Warfarin | Uninterrupted | 2.2 (1.7-2.8) | 100% | 100% | |
| 23 | Kirchhof P et al. European Heart Journal 2018 | ≥ 4 weeks | ≥ 4 weeks | 3.5 | 6 | Uninterrupted | Uninterrupted | VKA | Uninterrupted | NR | 87% | 87% | |
| 24 | Kochhauser S et al. Can J of Card 2014 | ≥ 4 weeks | ≥ 4 weeks | NR | NR | > 24 h | 8 h | Warfarin | W stopped 4 days, LMWH bridge 2 days | W night of procedure + LMWH bridging | NR | 100% | 100% |
| 25 | Koektuerk B et al. Cardiovasc Therap 2016 | NR | NR | NR | NR | 24 h | Evening of procedure | Phenprocoumon | Uninterrupted | NR | 100% | 100% | |
| 26 | Konduru SV et al. J Int Card Electrophys 2012 | NR | NR | 54 | 29* | Uninterrupted or 24 h | Evening of procedure | Warfarin | Uninterrupted | 2.2 ± 0.3 | 100% | 100% | |
| 27 | Kuwahara T et al. J of Card Electrophys 2016 | ≥ 30 days | ≥ 30 days | NR | NR | Uninterrupted | Uninterrupted | Warfarin | Uninterrupted | 2.2 ± 0.6 | NR | NR | |
| 28 | Lakkireddy D et al. JACC 2012 | ≥ 4 weeks | ≥ 4 weeks | 34 | 34 | Morning of procedure | 3 h post hemostasis | Warfarin | Uninterrupted | 2.0-3.5 | 100% | none | |
| 29 | Lakkireddy D et al. JACC 2014 | ≥ 4 weeks | ≥ 3 weeks | 31 | 26 | Uninterrupted | ≥ 3 h post hemostasis | Warfarin | Uninterrupted | 2.3 ± 0.4 | 100% | Only for low INR | |
| 30 | Lin J et al. J Afib 2014 | NR | NR | NR | NR | 36 h | Morning after procedure | Warfarin | W stopped 3-5 days; LMWH bridge | W night of, LMWH morning post procedure | N/A | Most of patients | Most of patients |
| 31 | Maddox W et al. J Card Electrophysiol 2013 | ≥ 4 weeks | ≥ 4 weeks | NR | NR | Uninterrupted | Uninterrupted | Warfarin | Uninterrupted | 2.3 ± 0.5 | 100% | 100% | |
| 32 | Mugnai G et al. American J of Card 2017 | NR | NR | NR | NR | > 24-36 h | Evening of procedure | Warfarin Acenocoumarol | W stopped > 24 h, if INR<2, bridged w LMWH | LMWH same day of procedure | NR | 100% | 100% |
| 33 | Muller P et al. J Interv Card Electro 2016 | NR | NR | NR | NR | Uninterrupted or 24 h | Evening of procedure | VKA | VKA stopped 5-7 days, bridged w LMWH | heparin infusion 4 h initial and LMWH day after procedure | NR | 100% | 100% |
| 34 | Murakawa Y et al. J of Arrhythmia 2015 | NR | NR | NR | NR | 0-24h | NR | Warfarin | Uninterrupted | NR | NR | NR | |
| 35 | Nagao T et al. Heart Rhythm 2015 | ≥ 4 weeks | ≥ 4 weeks | 9 | 7 | Uninterrupted | Uninterrupted | Warfarin | Uninterrupted | NR | 100% | 100% | |
| 36 | Nagao T et al. PACE 2015 | ≥ 4 weeks | ≥ 4 weeks | 11 | 11 | Uninterrupted | Uninterrupted | Warfarin | Uninterrupted | 2.2 ± 0.5 | 100% | 100% | |
| 37 | Nagao T et al. Internal Med 2015 | ≥ 4 weeks | ≥ 4 weeks | 9 | 9 | Uninterrupted | Uninterrupted | Warfarin | Uninterrupted | 2.2 ± 0.5 | 100% | 100% | |
| 38 | Nin T et al. PACE 2013 | ≥ 3 weeks | ≥ 3 weeks | NR | NR | > 24 h | Immediate post-procedure | Warfarin | W stopped > 24 h | ≥ 4 h post procedure hemostasis | 1.8 ± 0.4 | 100% | 100% |
| 39 | Nogami A et al. JAMA 2019 | ≥ 4 weeks | ≥ 4 weeks | NR | NR | 1-2 doses withheld, UFH bridging if > 24 h | 8 h post procedure | Warfarin | Uninterrupted | NR | 86% | 84% | |
| 40 | Okishige K et al. J of Card 2017 | ≥ 4 weeks | ≥ 4 weeks | NR | NR | 12-24 h, one dose held | Evening of procedure | Warfarin | Uninterrupted | NR | NR | NR | |
| 41 | Reynolds MR et al. JACC EP 2018 | ≥ 3 weeks | ≥ 3 weeks | 24 | 32 | Uninterrupted Morning of procedure | Evening of procedure | Warfarin | Uninterrupted | 2.3 ± 0.5 | 46% | 69% | |
| 42 | Rilling A et al. JCE 2016 | NR | NR | 3 | 2 | > 36 h | Evening of procedure | Phenprocoumon | Uninterrupted | 2.3 (2.1,2.5) | 100% | 100% | |
| 43 | Snipelisky D et al. J Int Card Electrophys 2012 | NR | ≥ 30 days | NR | NR | Morning of procedure | Evening of procedure | Warfarin | W stopped > 24 h | Evening of procedure | 2-3 | NR | NR |
| 44 | Snipelisky D et al. J Int Card Electrophys 2014 | NR | NR | 4 | 10 | R night prior D morning of procedure | Evening of procedure | Warfarin | W stopped > 24 h | Evening of procedure | NR | NR | NR |
| 45 | Somani R et al. Cardiovasc Therap 2014 | ≥ 4 weeks | ≥ 4 weeks | NR | NR | > 24-30h | Immediate post-procedure | Warfarin | Uninterrupted; W stopped 1 week - LMWH until 24-30h prior procedure | Uninterrupted; LMWH 1/2 dose 4h post hemostasis; 12h full dose | NR | 100% | 100% |
| 46 | Stepanyan G et al. J Int Card Electrophys 2014 | ≥ 1 week | NR | NR | NR | > 24-36 h | Morning after procedure; UFH infusion 6 h post procedure | Warfarin | Uninterrupted | NR | PeAF and inconsistent AC last 30 days | PeAF and inconsistent AC last 30 days | |
| 47 | Tang l et al. Frontiers in Med 2020 | NR | NR | NR | NR | Morning of procedure | Evening of procedure | Warfarin | Uninterrupted; W stopped 35 days; LMWH bridge | Uninterrupted; W night of procedure, LMWH bridge | NR | 100% | 100% |
| 48 | Tao S et al. J Int Card Electroph 2017 | ≥ 4 weeks | ≥ 4 weeks | 8 | 14 | Uninterrupted | Uninterrupted | Warfarin | Uninterrupted | 2.2 | 100% | 100% | |
| 49 | Tscholl V et al. Clinical Cardio 2017 | NR | NR | NR | NR | Morning of procedure | Uninterrupted | Phenprocoumon | Uninterrupted | 1.8 ± 0.5 | 100% | 100% | |
| 50 | Vlachos K et al. Clinical Cardio 2017 | ≥ 2 months | NR | NR | NR | Uninterrupted R Morning of procedure D, A | Uninterrupted Evening of procedure | Acenocoumarol | Uninterrupted | NR | 100% | 100% | |
| 51 | Yamaji H et al. Clin Drug Inv 2013 | ≥ 30 days | ≥ 30 days | NR | NR | Morning of procedure | 3 h post hemostasis | Warfarin | Uninterrupted; W stopped 48 h; UFH subcutaneous bid | Uninterrupted; ; UFH subcutaneous until INR ≥ 2.0 | 2-3 | 100% | 100% |
| 52 | Yanagisawa S et al. JACC Clin Electrpph 2018 | ≥ 3 weeks | ≥ 3 weeks | 9 | 16 | Uninterrupted | Uninterrupted | Warfarin | Uninterrupted | 2.0 ± 0.6 | 100% | 100% | |
| 53 | Yoshimura et al. Journal of Card 2017 | NR | NR | NR | NR | R uninterrupted A morning of procedure | Evening of procedure | Warfarin | Uninterrupted | 2.0 ± 0.6 | 100% | 100% | |
More than half of the centers reported using pre-procedural TEE or CT angio to exclude intracardiac thrombus, and there were no significant differences between the two groups.
The primary ablation strategy for AF was pulmonary vein isolation using radiofrequency energy, with cryoballoon technology being used in 7 studies21,40,45,53,57,60,61. Additional linear and CFAE ablation was performed based on operator preference, mostly in patients with persistent atrial fibrillation. Additional atrial flutter ablation was performed in a significant minority of the patients.
In all the studies that reported intra-procedural anticoagulation, heparin bolus, fixed or weight-based, was used either before or after the trans-septal puncture. The majority of the studies also employed continuous heparin infusion. The target ACT was usually > 300 secs, generally achieved in both groups. Several studies reported lower levels of ACT despite higher requirements for heparin in the DOACS group. Intracardiac echo to guide the trans-septal puncture and ablation was not used routinely. Partial or full reversal of heparin with protamine was utilized for many patients. (Table 4)
Procedural Characteristics; W – warfarin; TS –transseptal puncture; ACT – activated clotting time.
In the 31589 patients, there were a total of 2384 (7.5%) complications, with 973 (6.8%) complications in the DOACS group representing a significantly lower rate than 1411 (8.1%) complications in the VKA group (OR = 0.80, CI 0.69-0.93, I2 = 48%, p = 0.004) (Figure 3).
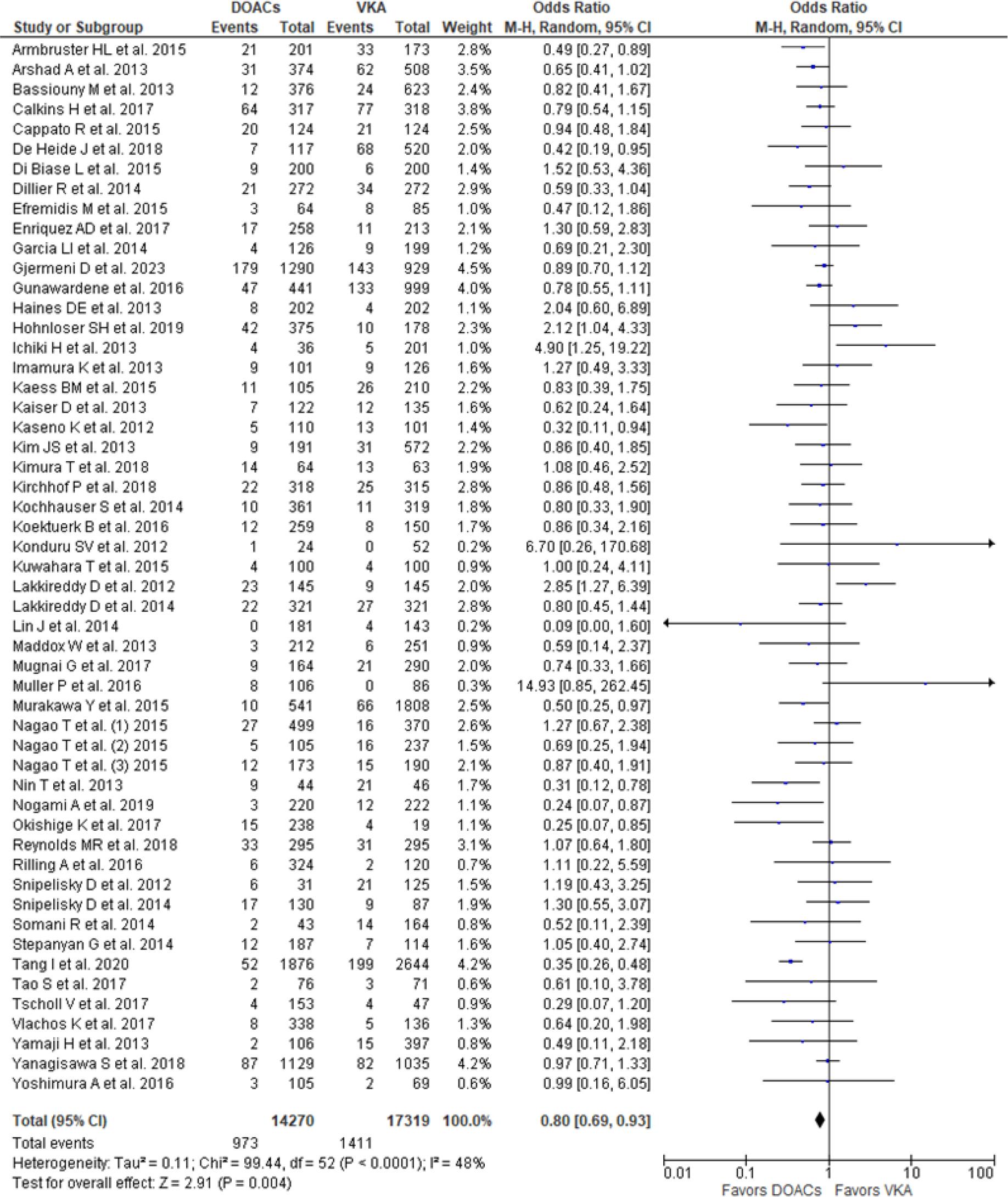
Total Complications – Entire Cohort.
The thromboembolic complication rates were similar between the groups, 54 (0.38%) for patients on DOACS vs. 66 (0.38%) for patients on VKA (OR 0.76, 95% CI 0.53-1.10, I2 = 0%, p = 0.15) (Figure 4), with significantly lower total bleeding complications in the DOACS group 919 (6.4%) patients vs. VKA group 1345 (7.8%) patients (OR 0.80, 95% CI 0.69-0.93, I2 = 46%, p = 0.003) (Figure 5), driven by a lower incidence in both major bleeding [201 (1.4%) vs. 346 (2.0%)] and minor bleeding [718 (5%) vs. 999 (5.8%)] rates in DOACS group compared to VKA group(OR 0.71, CI 0.57-0.89, I2 = 11%, p = 0.002 and OR 0.84, CI 0.73-0.98, I2 = 31%, p = 0.03) (Figure 6).
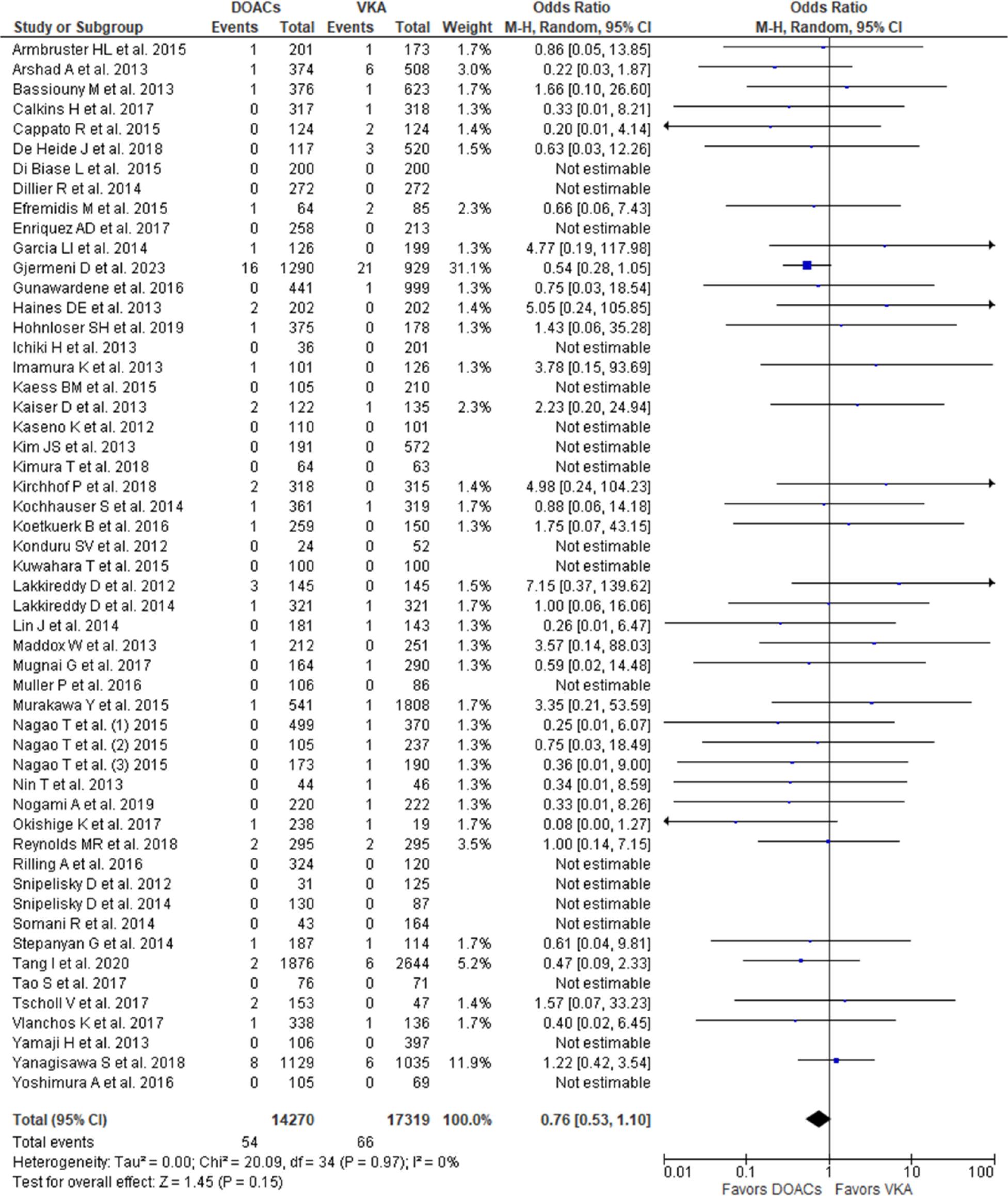
Thromboembolic Complications – Entire Cohort.
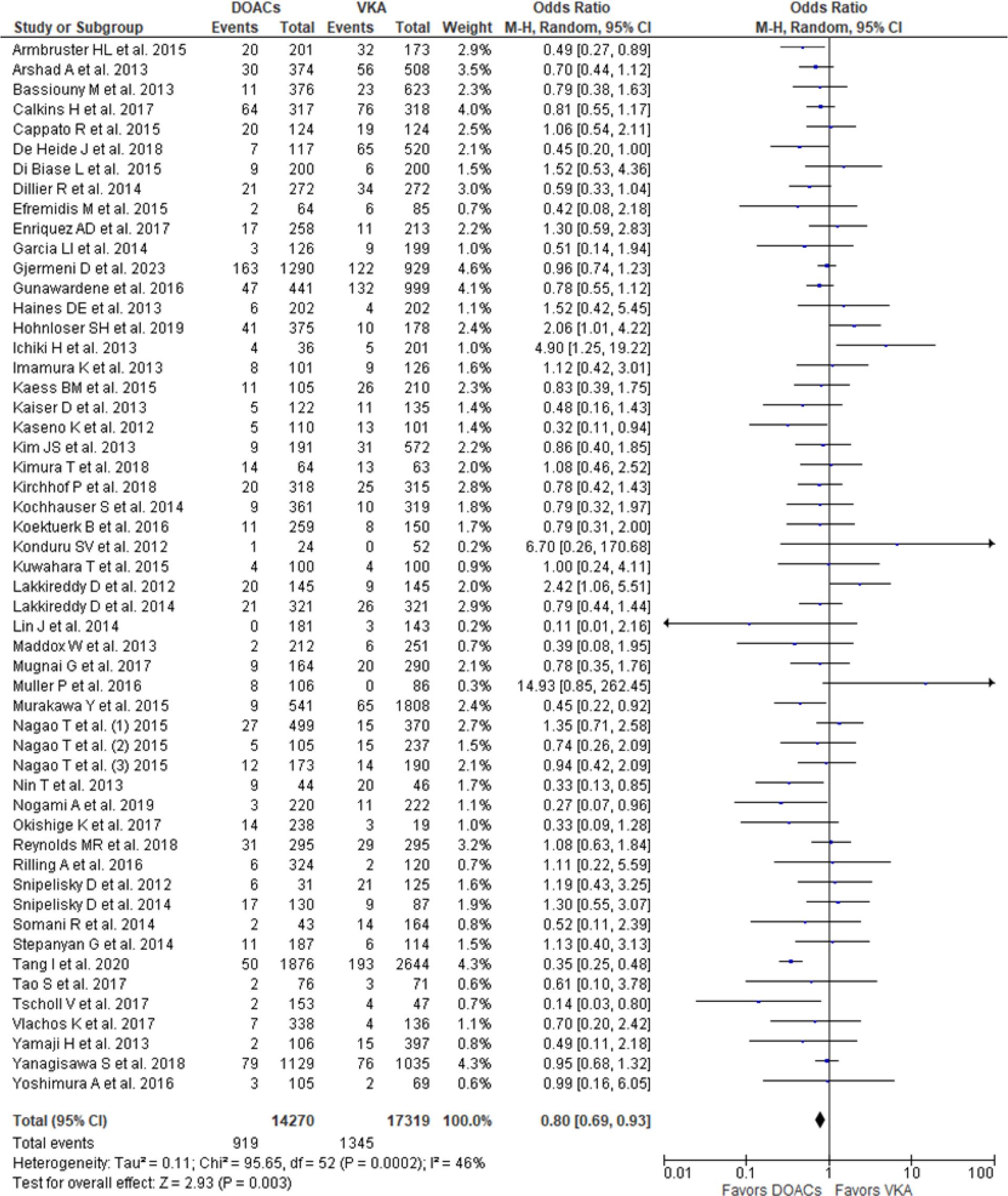
Total Bleeding Complications – Entire Cohort.
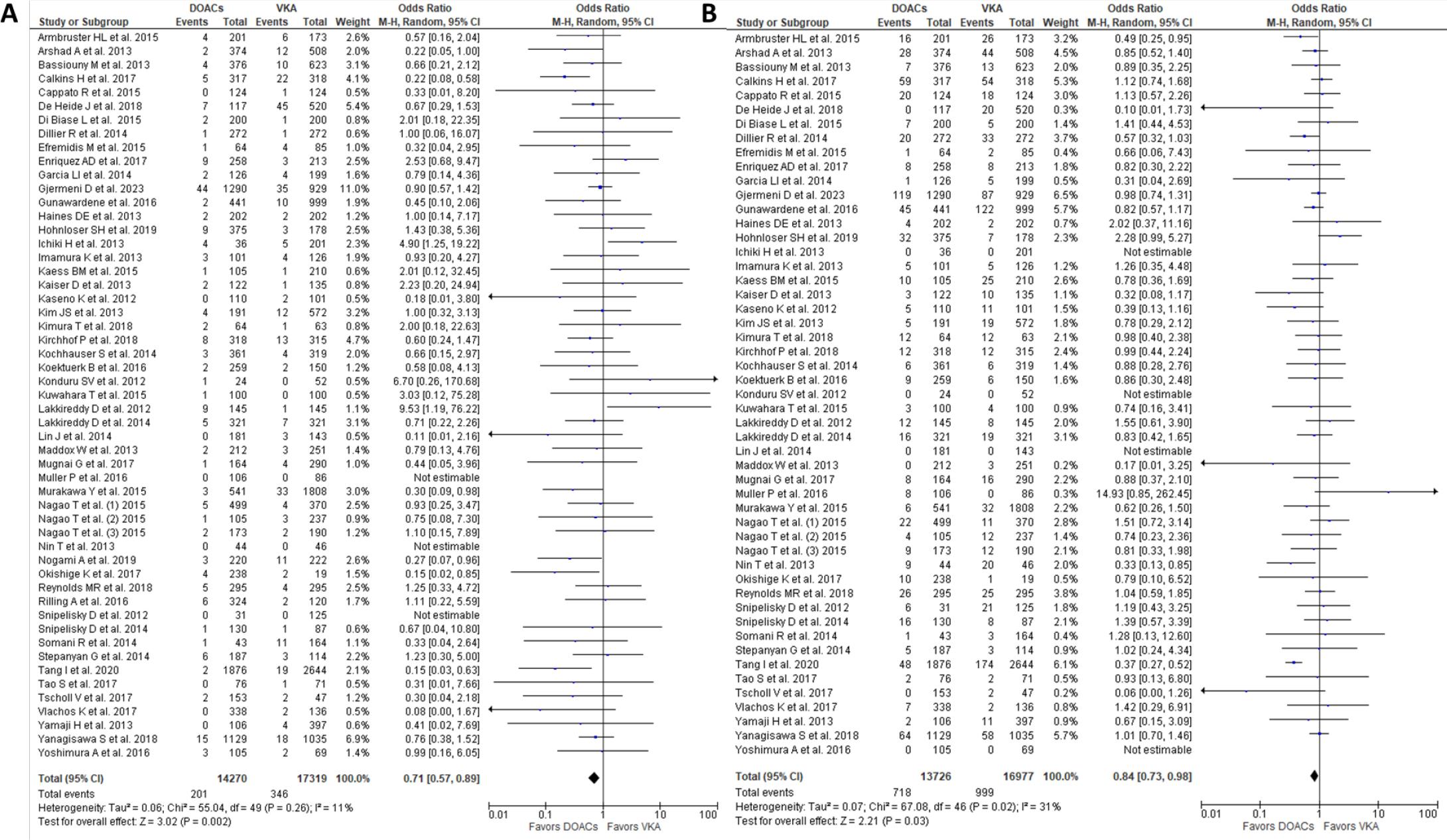
Major (A) and Minor (B) Bleeding Complications – Entire Cohort.
Interrupted and uninterrupted peri-procedural anticoagulation with either DOACS or VKA are used in the current practice. Continuous VKA has been suggested to be superior to interrupted VKA1,6; however, the optimal peri-procedural DOACS strategy still remains unclear54,68,69. In order to evaluate the safety of different strategies, we have evaluated the complications of (1) interrupted and (2) uninterrupted DOACS strategies compared to continuous VKA, as well as (3) DOACS (both interrupted and uninterrupted) with interrupted W subgroups separately. One study31 did not report complications separately for each W group and was not included in this analysis.
- (1)
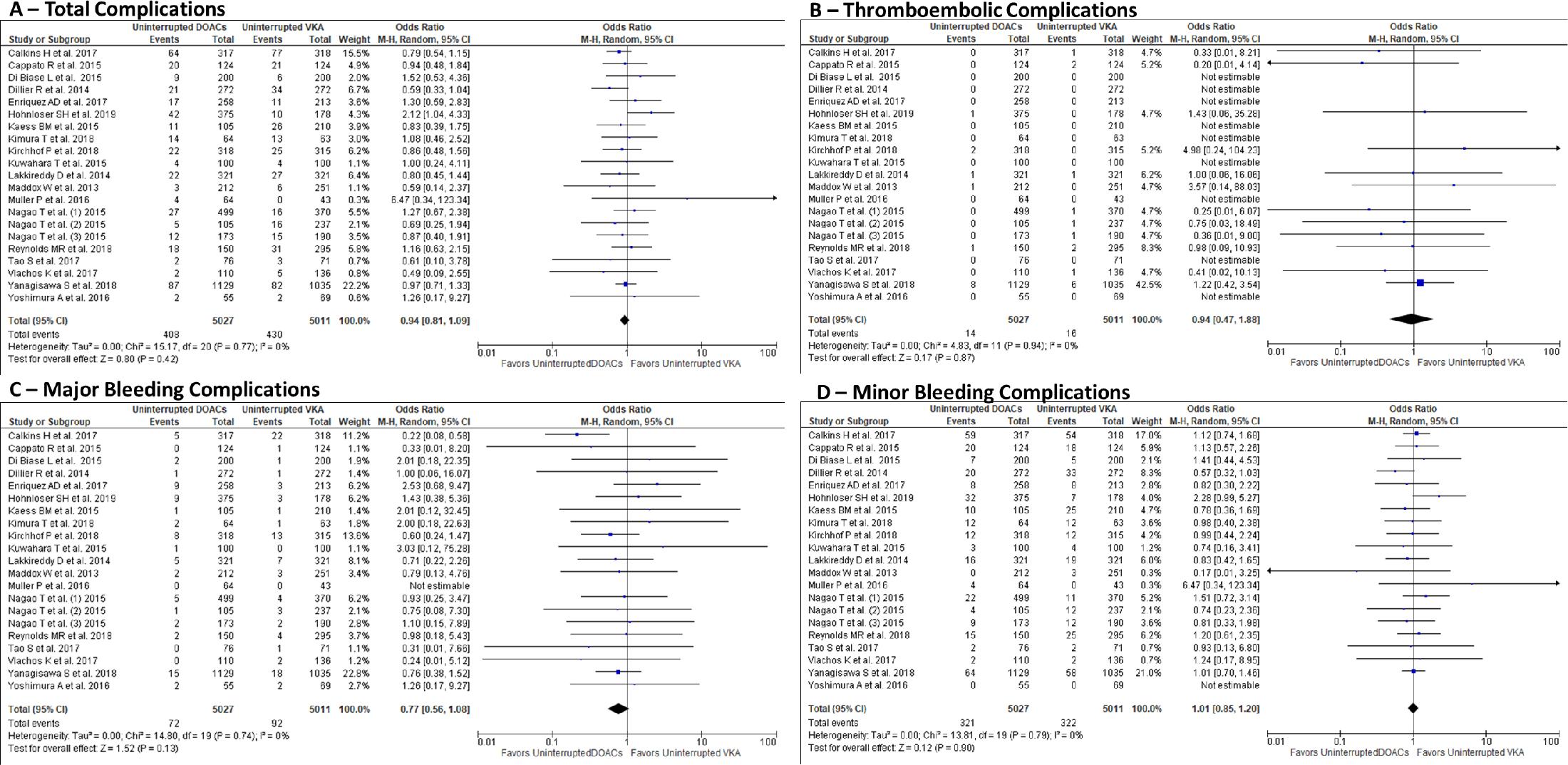
There were 21 studies14,17,21,22,24,25,27,33,37,38,41,42,44,46,48–50,54,62,64,65 including 10038 patients on uninterrupted anticoagulation (5027 on uninterrupted DOACS and 5011 patients on continuous VKA). The overall complication numbers were similar between the 2 uninterrupted anticoagulation strategies 408 (8.1%) for patients on DOACS and 430 (8.6%) for patients on VKA with no differences in thromboembolic events 14 (0.3%) for DOACS vs. 16 (0.3%) for VKA (OR 0.794, CI 0.47-1.88, I2 = 0%, p = 0.87), major or minor bleedings 72 (1.4%) for DOACS vs. 92 (1.8%) for VKA (OR 0.77, CI 0.56-1.08, I2 = 0%, p = 0.13) and 321 (6.4%) for DOACS vs. 322 (6.4%) for VKA (OR 1.01, CI 0.85-1.20, I2 = 0%, p = 0.90), respectively. (Figure 7 A, B, C, D)
- (2)
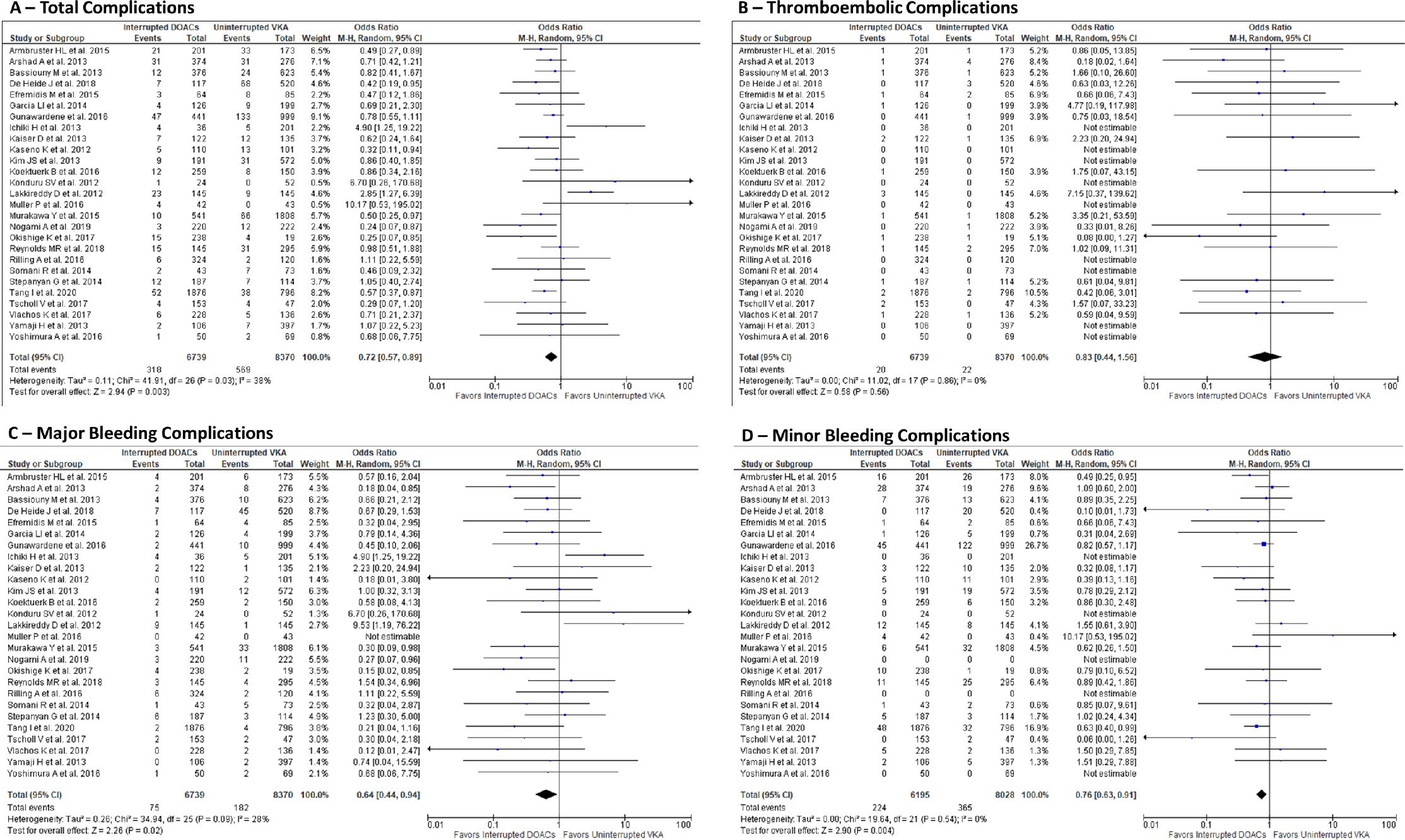
Interrupted DOACS strategy (≥ 1 doses held) compared with uninterrupted VKA was evaluated in 27 studies13,15,16,18–20,23,26,28,30,34–36,40,46,47,52–55,58–63,65 that included 15109 patients (6739 patients on interrupted DOACS and 8370 patients on uninterrupted VKA). The total number of complications was lower in the interrupted DOACS strategy with 318 (4.7%) events compared with uninterrupted VKA 569 (6.8%) events (OR 0.72, CI 0.57-0.89, I2 = 38%, p = 0.003). The superiority of the interrupted DOACS regimen was driven by lower rates of both major and minor bleedings [75 (1.1%) DOACS vs. 182 (2.2%) VKA (OR 0.64, CI 0.440.94, I2 = 28%, p = 0.02) and 224 (3.3%) DOACS vs 365 (4.4%) VKA (OR 0.76, CI 0.63-0.91, I2 = 0%, p = 0.004), respectively], with no difference in thromboembolic complications 20 (0.3%) DOACS vs. 22 (0.3%) VKA (OR 0.83, CI 0.44-1.56, I2 = 0%, p = 0.56). (Figure 8 A, B, C, D)
- (3)
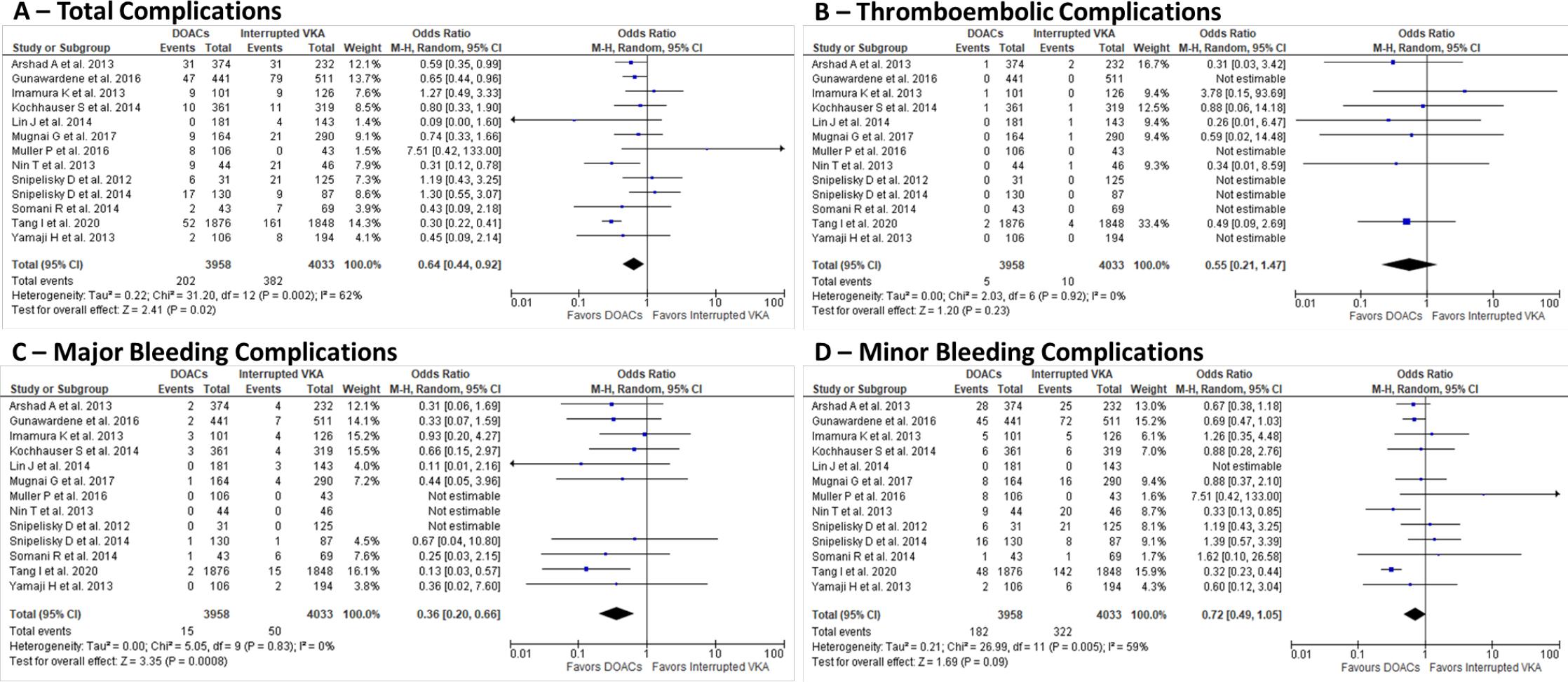
There were 13 trials19,30,32,39,43,45,46,51,56–58,60,63 that included an interrupted VKA group, 7 of them32,39,43,45,51,56,57 had interrupted the VKA group only, with a total of 7991 patients. On comparing the 3958 patients on DOACS with 4033 patients on interrupted VKA, there was a lower total complication rate 202 (5%) DOACS vs. 382 (9.5%) VKA (OR 0.64, CI 0.44-0.92, I2 = 62%, p = 0.02), driven by a decrease in major bleeding complications, 15 (0.4%) DOACS vs. 50 (1.2%) VKA (OR 0.36, CI 0.20-0.66, I2 = 0%, p = 0.0008), with lower numerical but no difference in thromboembolic and minor bleeding events, 5 (0.1%) DOACS vs. 10 (0.2%) VKA (OR 0.55, CI 0.21-1.47, I2 = 0%, p = 0.23) and 182 (4.6%) DOACS vs. 322 (8.0%) VKA (OR 0.72, CI 0.49-1.05, I2 = 59%, p = 0.09). (Figure 9 A, B, C, D)
Complications Uninterrupted DOACS vs. Uninterrupted VKA.
Complications Interrupted DOACS vs. Uninterrupted VKA.
Complications DOACS vs. Interrupted VKA.
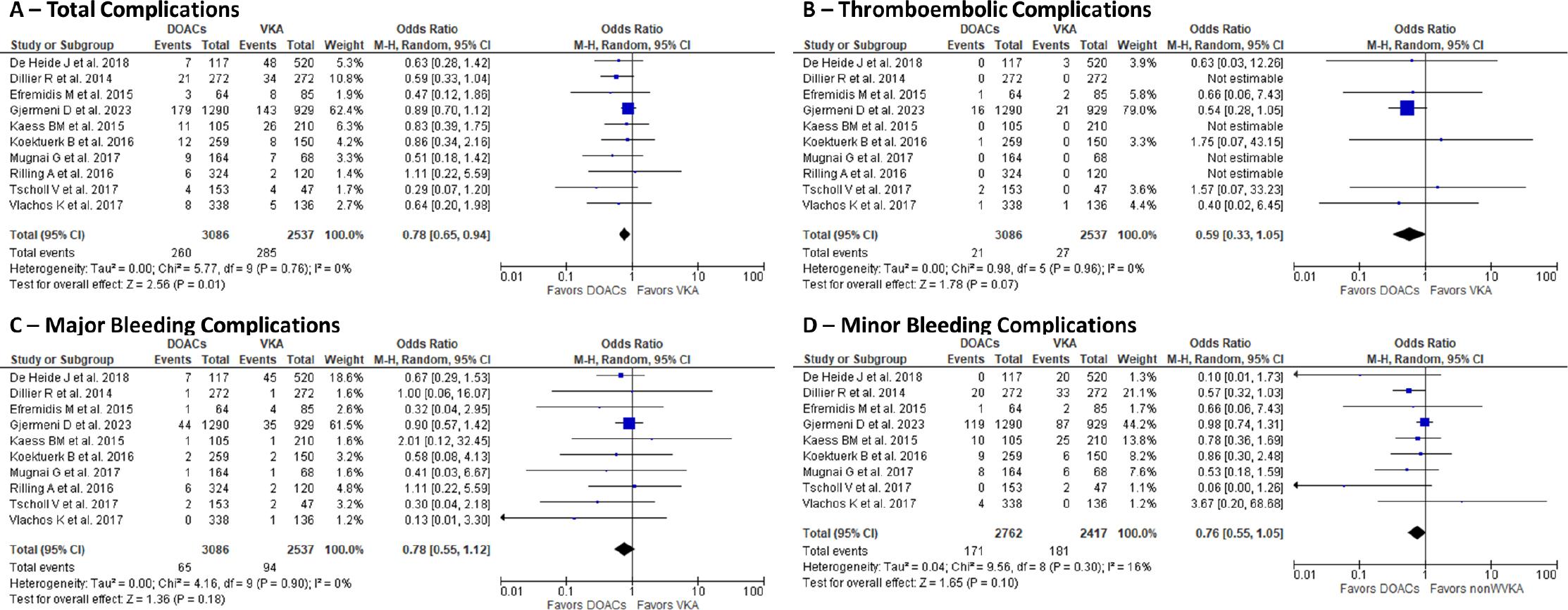
There were 10 studies23,25,26,29,33,40,45,55,61,62 that evaluated the bleeding and thromboembolic complications of non-warfarin (W) VKA (phenprocoumon, acenocoumarol) in comparison with DOACS and included a total of 5623 patients (3086 on DOACS and 2537 on nonWVKA). Total complications were lower in the DOACS group, 260 (8.4%), compared with the non-WVKA group, 285 (11.2%). The risk for thromboembolic, major, and minor bleeding complications was similar for both groups: 0.7% DOACS vs 1.1% nonWVKA, 2.2% DOACS vs 3.7% nonWVKA, and 5.6% DOACS vs 7.1% nonWVKA, respectively. (Figure 10 A, B, C, D)
Complications DOACS vs non-Warfarin VKA.
The safety profile of each of the 3 main DOACS: D, R, and A, was evaluated compared to VKA. The subgroups included 5536 patients on D, which were compared with 8255 patients on VKA, 3849 patients on R, 4852 patients on VKA, and 1913 patients on A, compared with 4148 patients on VKA. There was a significant decrease in number of total complications in dabigatran group, with 414 (7.5%) vs 692 (8.4%) in VKA group (OR 0.81, CI 0.67-0.98, p = 0.03, I2 = 35%) due to a decrease in bleeding complications, 5.3% D vs. 7.0% VKA (OR 0.81, CI 0.67-0.98, p = 0.03, I2 = 32%), and no difference in thromboembolic events, 0.49% D vs. 0.53% VKA (OR 0.81, CI 0.50-1.32, p = 0.62, I2 = 0%). (Figure 11 A) There were 211 complications (6.1%) in the R group and 312 complications (8.0%) in the VKA group, with no significant difference in the total, bleeding, and thromboembolic complication rates between the groups. (Figure 11 B) There were 153 complications (8.9%) in the A group and 296 complications (9.2%) in the VKA group, with no significant difference in the rates of total, bleeding, and thromboembolic complications between the groups (Figure 11C).
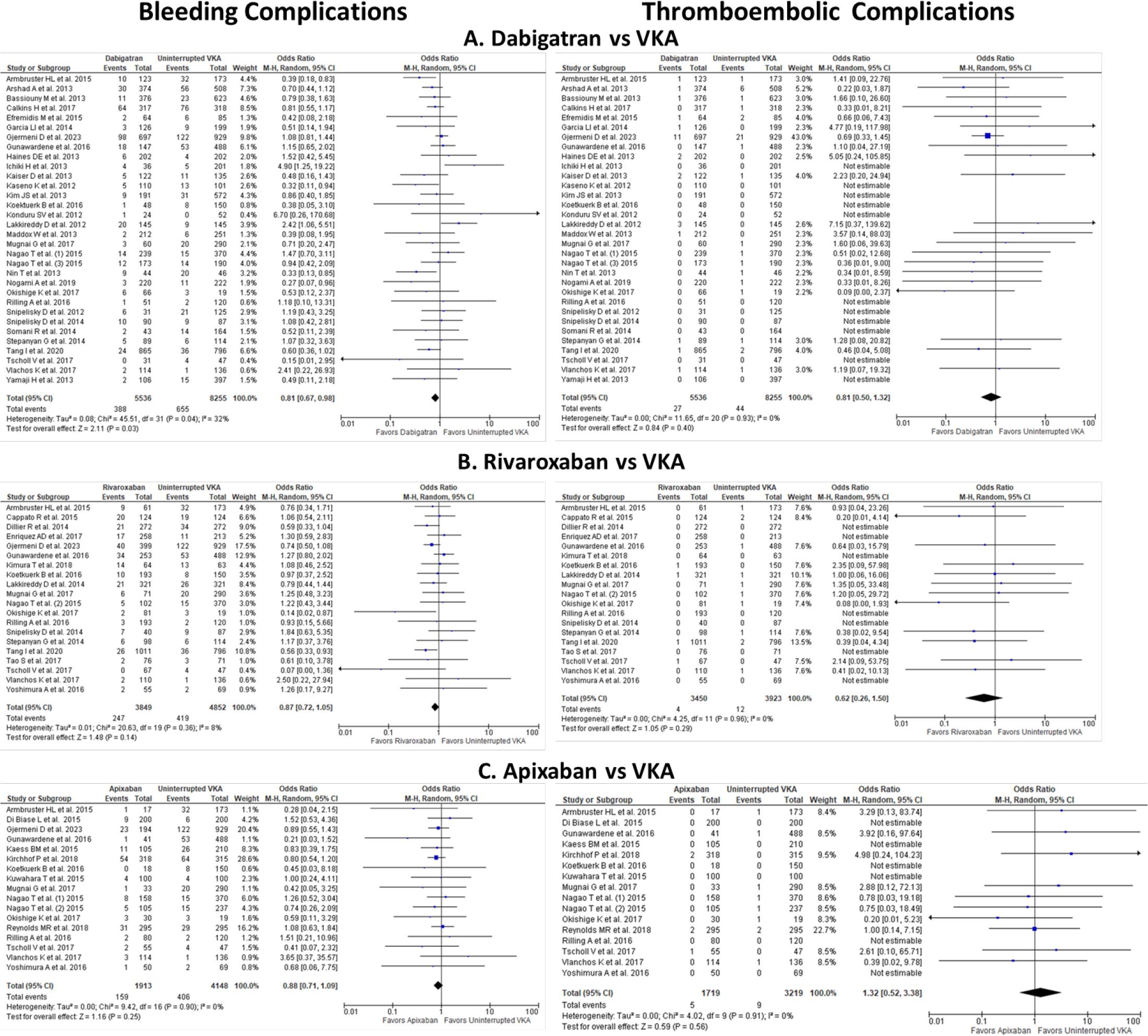
Bleeding and Thromboembolic Complications of Dabigatran, Rivaroxaban, Apixaban Compared to VKA.
This meta-analysis demonstrates that interrupted DOACS regimens are superior to uninterrupted VKA regimens in reducing bleeding complications, with no increase in thromboembolic events. This is the largest, with 31,589 patients, most comprehensive, and the only meta-analysis of thromboembolic and bleeding complications comparing all the available DOACS (D, R, A, and E) with VKA as peri-ablation anticoagulation strategies. To our knowledge, it included all published full-text series through October 2023, which enrolled patients with consistent anticoagulation regimens pre- and post-ablation.
The major findings of our study included: 1) Overall, the DOACS peri-AF ablation anticoagulation strategy is superior to VKA with a significant decrease in bleeding complications and similar thromboembolic complications. 2) Uninterrupted regimes with DOACS and VKA yielded similar total, bleeding, and thromboembolic events. 3) Interrupted DOACS regimen was superior to uninterrupted VKA with lower bleeding complications, and no increase in thromboembolic complications. 4) DOACS strategy was superior to non-WVKA regimens for total complications. 5) DOACS regimen had lower bleeding complications compared to interrupted VKA. 6) D peri-AF ablation resulted in lower complications than VKA, driven by a decrease in post-procedural bleeding. The R and A had complications similar to those of VKA.
This is the first meta-analysis to show that an interrupted DOACS regimen is superior to an uninterrupted VKA (Central Figure).
Important for the interpretation and the reliability of the results, our analysis did not find any strong evidence in favor of publication bias in the dataset of trials included.
The initial concerns of increased total complications with D, raised by Lakkireddy et al15 and Ichiki et al16 studies, are not supported in the current meta-analysis. Those prior results were driven by an unusually high incidence of cardiac tamponade and pericardial effusions in the D group [15 in 145 patients (10%),15 and 4 in 36 patients (11.1%)16, respectively]. It is notable that patients in these series underwent extensive AF ablation, which may not be representative of the experiences of other centers. Interestingly enough, the strategy of interrupted DOACS yielded better results than uninterrupted regimens, likely due to the lower incidence of bleeding found in patients taking D compared with those on A and R. The vast majority of patients taking D had at least one dose of medication held before the procedure (> 80%), in contrast, the medication was uninterrupted in > 75% of patients taking the A and R.
Several other meta-analyses were published that compared DOACS with VKA, mainly W. The current meta-analysis included all the studies in these prior analyses if they conformed to the inclusion criteria of our study. No prior meta-analysis has compared specifically the continuous and interrupted DOACS and VKA regimens, which are still widely used in clinical practice. During the effort to acquire all relevant published data, we also found that some previous meta-analyses failed to include all the studies reported during their specified search periods or had restrictive searching criteria. Several of the prior meta-analyses included studies with inconsistent anticoagulation strategies pre vs. post ablation, with change from VKA to DOACS, or fully interrupted periprocedural anticoagulation, thus introducing selection bias in their results.
One of the first meta-analyses of D vs W published by Steinberg70 reported similar composite total complications, but with the D group having a higher incidence of thromboembolic events, the only meta-analysis to reach this conclusion, most likely due to a small number of studies included. Rui Providencia71 included studies using periprocedural D and W, which demonstrated no difference in thromboembolic events or major bleeding and a lower incidence of minor bleeding with D use. Several other early meta-analyses of D vs. W72–74 showed no difference in the thromboembolic or bleeding complications.
Subsequent meta-analyses by Aryal75 and Phan76,77 that included R and D comparing with W strategies, showed comparable safety with all 3 strategies, but these analyses included either studies with significant changes amongst pre- and post-procedural anticoagulation strategies, or a post hoc analysis of the Rocket AF study that lumped together patients post-electrical or pharmacologic cardioversion with AF ablation patients78. Thus the results of these meta-analyses have to be interpreted with caution as might be skewed given such inhomogeneous groups.
More recent meta-analyses by Ukaigwe79, Lu80 and Bladino81, comparing either interrupted or uninterrupted A to W demonstrated similar bleeding and thromboembolic events between the two groups.
Overall, the results of these meta-analyses are mixed, based on the series included, the majority of which show no benefit of uninterrupted or interrupted DOACS over VKA, and one reported an increased thromboembolic event with DOACS. Thus, a more comprehensive meta-analysis, including more patients and consistent anticoagulation protocols, helps provide a better understanding of the benefits and risks of different anticoagulation protocols. In our meta-analysis, we have shown a significant benefit from DOACS over VKA.
The peri-procedural strategy at the beginnings of AF ablation was interrupted W with heparin bridging, however several studies, including a randomized trial, Di Biase6, and 2 meta-analyses, by Santangeli7 in 2012 and more recent one by Bawazeer82 in 2021 suggested that uninterrupted VKA is safe and superior to bridged VKA strategy with less thromboembolic events without significant increase in bleeding complications. However, other studies, including one of the studies from the current meta-analysis, Arshad et al.19, found a higher percentage of major complications with uninterrupted W arm (4.3%), driven by major bleeding, when compared with both bridged W (2.6%) or D (0.8%) arms. There are some proponents of interrupted peri-procedural anticoagulation, without bridging, or only post-procedural anticoagulation, especially in low stroke risk patients. Winkle et al.83 evaluated interrupted peri-procedural anticoagulation in 2334 patients and found a low rate of total periprocedural complications (1.5%) with a 0.3% TIA/stroke rate using this strategy.
The use of the interrupted VKA strategy has faded lately. However, there are still sites using interrupted anticoagulation to avoid cancellation of the procedure due to supra- or subtherapeutic INR and some operators’ perception of safer management of intraprocedural major bleeding complications without the anticoagulation effect of VKA.
The studies included in this meta-analysis reflect real-world practice, with a large variance regarding the timing of holding the VKA strategy studies, which had different timing and bridging modalities. Our meta-analysis, which included more than 4000 patients with interrupted VKA, showed a significant increase in major bleeding events compared with DOACS.
Current guidelines1 We recommend a continuous anticoagulation strategy peri-procedural for atrial fibrillation ablation with a class I indication. In our meta-analysis, we found no difference in complication rates between uninterrupted DOACS and uninterrupted VKA.
In the current practice, most patients are on DOACS, and it is unclear if continuous or minimally interrupted without a bridging strategy is better. There is a concern that uninterrupted anticoagulation may lead to a higher risk of access site bleeding or cardiac tamponade. The minimally interrupted DOACS approach, with no bridging may theoretically reduce these risks without significantly compromising thromboembolic protection. Proponents of the minimally interrupted strategy argue that a brief discontinuation of DOACS may reduce bleeding complications during catheter manipulation without significantly increasing the risk of thromboembolism. Although hard to rigorously prove in a trial, skipping 1 or 2 doses might decrease the severity of a complication such as cardiac tamponade, were it to happen, and possibly make managing such complications easier to handle.
A trial by Nakamura84 randomized 846 patients to either uninterrupted or interrupted (the day of the procedure and restarted the next morning) DOACS and showed no differences in bleeding or thromboembolic events. In addition, a 2021 meta-analysis by van Vugt69 including 2168 patients evaluating strategies of minimally interrupted versus uninterrupted DOACS administration found no difference in bleeding nor in embolic complications.
In our meta-analysis, there was a large variability in periprocedural DOACS strategies, with 5027 patients on uninterrupted DOACS and 6739 patients using a minimally interrupted DOACS strategy. There was no difference in the thromboembolic or bleeding incidence when compared with uninterrupted DOACS and uninterrupted VKA regimen; however, the minimally interrupted DOACS had a significantly lower incidence of major bleeding events compared with uninterrupted VKA, with no increase in thromboembolic complications.
Despite the lack of guideline recommendations on the minimally interrupted use of DOACS, this strategy is increasingly adopted in clinical practice. Our data suggests that minimally interrupted DOACS use may be a reasonable strategy for reducing bleeding risk without increasing thromboembolic complications. Further large-scale studies are needed to precisely define the optimal periprocedural anticoagulation strategy, especially in high-risk patient populations.
This study’s limitations are those inherent to any meta-analysis. The data analyzed emanates mainly from observational studies, with only a minority of the trials being randomized, controlled, or prospective. One third of the trials were reported in abstract format, and despite best attempts to gather information, including direct contact with the author, some data remained incomplete. The lack of evidence for publication bias provides reassurance regarding the robustness of our broad inclusion strategy. There is a significant variability among individual studies, translating into heterogeneity in the reported data for total and bleeding complications (I2 ~ 30). The meta-analysis could not control the variation of practices among different institutions or other factors that might alter the risk for complications, including operator experience, ablation strategies and duration, TEE and ICE usage, and patient risk factors. Nonetheless, the very large sample protects against some of these potential biases.
This meta-analysis demonstrates in over 31,500 patients that DOACS are a great alternative to VKA in patients undergoing ablation for AF with lower bleeding rates. There is no significant increase in thromboembolic events and a decrease in total complications. Minimally interrupted DOACS proves to be a viable strategy, with lower bleeding complications than uninterrupted VKA and similar risk for thromboembolism. Future studies should determine the optimal time to stop and restart of the DOACS relative to the ablation.