Venous thromboembolism (VTE), in the form of deep vein thrombosis (DVT) or pulmonary embolism (PE), is the third most frequent acute cardiovascular syndrome, after myocardial infarction and stroke [1]. Several risk factors have been associated with VTE, ranging from strong risk factors (OR>10, e.g. lower limb fracture, major trauma, previous VTE, etc.) to moderate risk factors (OR 2-9, e.g. pregnancy, postpartum period, blood transfusion, oral contraceptive therapy, etc.) and weak risk factors (OR<2, e.g. bed rest >3 days, diabetes mellitus, arterial hypertension, etc.) [2]. Therapeutic drug regimens include systemic thrombolysis for high-risk patients (in the absence of contraindications-e.g. history of hemorrhagic stroke, ischemic stroke in the past 6 months, active bleeding, major trauma or surgery in the last 3 weeks, etc.), alongside anticoagulation for all patients, regardless of risk class [1]. Even though, when compared to anticoagulation, systemic thrombolysis leads to faster improvements in the pulmonary circulation, with a reduction in pulmonary artery pressure (PAP) and pulmonary vascular resistance (PVR), it carries the burden of an increased risk of life-threatening hemorrhage, thus limiting its use in high-risk patients. Considering the benefits of thrombolysis, several studies have investigated the benefits of local, catheter-directed thrombolysis in intermediate-risk patients in recent years [3,4,5,6].
We present the case of a 41-year-old woman, who was admitted to the emergency room for dyspnea and extreme fatigue during minimal exertion, symptoms which started immediately after birth and aggravated suddenly 3 days prior to admission. The patient was in the 20th day postpartum and had a history of gestational hypertension (diagnosed in the 34th week of pregnancy). This was the fifth pregnancy of the patient, with no prior history of ante- or postnatal complications, nor any history of abortions or contraceptive drugs use.
Physical examination revealed an elevated heart rate of 115 bpm, with a second-degree (II/VI) tricuspid systolic murmur and an elevated blood pressure of 140/90 mmHg. No signs of DVT were noticed at the time of admission. The patient also presented an increased respiratory rate and an 87% oxygen saturation, which increased to 98% after oxygen administration through a nasal cannula.
The electrocardiogram showed sinus tachycardia of 113 bpm and signs of right ventricular strain (negative T waves in the inferior leads and T wave abnormalities in the anterior leads) as well as the McGinn-White pattern – S1Q3T3 (Figure 1). Laboratory tests performed in the emergency department showed mildly increased highly sensitive I troponin levels (75.9 ng/L; normal range under 29 ng/L), and increased NT-proBNP levels (2248 pg/mL; normal range under 125 pg/mL).
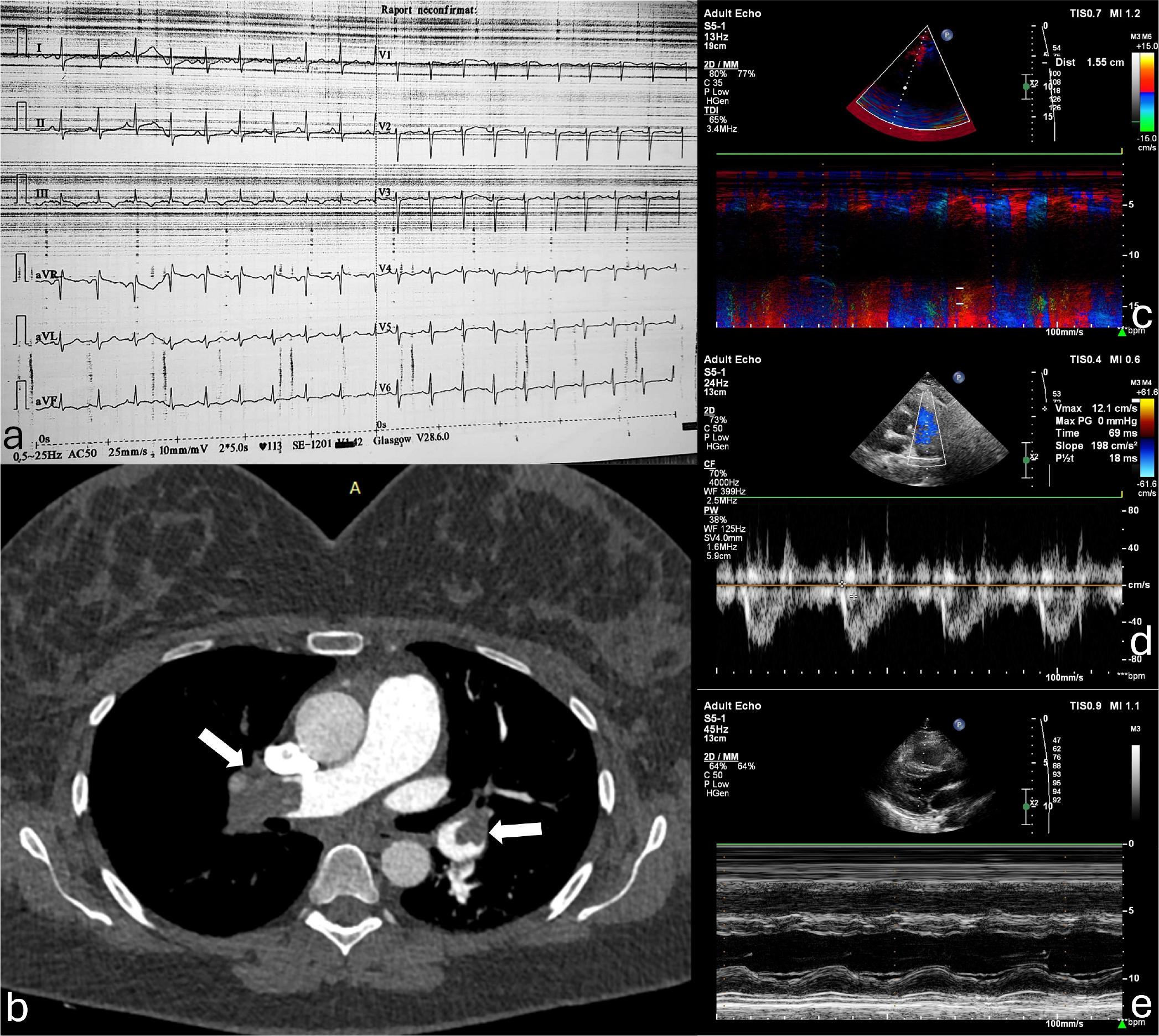
Diagnostic tests before treatment decision. a. Electrocardiogram in the Emergency Department (V-25mm/sec, A-10mm/mV) depicting sinus tachycardia, right ventricular strain, and S1Q3T3 (McGinn-White) pattern. b. Computed tomography pulmonary angiography showing the obstruction of the pulmonary arteries (arrows). c-e. Echocardiographic images registered in the Cardiology Ward, showing a reduced (15.5 mm) tricuspid annular plane systolic excursion (TAPSE) measured by M-mode (c), a severely reduced pulmonary artery acceleration time (69 msec), with a mid-systolic notch (d), and the flattening of the interventricular septum due to the increased right ventricular pressure (e).
Echocardiography revealed a dilated right ventricle with a decreased systolic function (tricuspid annular plane systolic excursion of 15mm), a moderate tricuspid regurgitation, with a transvalvular gradient of 50 mmHg, a dilated inferior vena cava with no inspiratory collapse. An additional sign of increased pressure in the right chambers was the paradoxical septal motion of the interventricular septum and a D-shaped left ventricle (Figure 1).
Based on these findings, noted in the presence of postpartum status (moderate risk factor), and the results of predictive scores for the likelihood of PE (moderate risk group in the Geneva- and Wells scores, and 2 positive criteria of the PERC rule), a computed tomographic pulmonary angiography was performed. The investigation showed acute obstruction of both pulmonary arteries, extending bilaterally to all lobar branches (Figure 1). The patient was admitted to the Cardiology Ward for further investigations and antithrombotic treatment. A gynecology consultation was also performed in the emergency department, which excluded any active hemorrhagic sources as well as any local complications of pregnancy and childbirth as a potential contraindication for systemic thrombolysis.
We calculated a GENEVA score of 5 points and a PESI score of 101 points. Considering the intermediate-high risk of pulmonary embolism, for the first 24 hours the patient received supplemental oxygen and i.v. unfractionated heparin (UFH), with no significant improvement in clinical status or the cardiac function, despite the activated partial thromboplastin time (aPTT) being in the therapeutic range (50-70 sec). To investigate the source of embolism, a lower limb venous Doppler ultrasound investigation was performed, which revealed acute thrombotic material in both right and left iliac and femoral veins.
In this setting, we considered catheter-directed thrombolysis, aiming to increase the chances of pulmonary artery clot dissolution, with lower bleeding risk compared to systemic thrombolysis. Written consent for the procedure was obtained after carefully weighing potential benefits and risks and thoroughly discussing all therapeutic options with the patient.
Right heart catheterization was performed after echo-guided puncture of the left femoral vein, in which two 5F sheaths were placed. This side was chosen because the left ilio-femoral veins were only partially occluded by thrombi, in contrast to the right side, where complete thrombotic occlusion was described. Right ventricular systolic pressure and pulmonary artery systolic pressure were both elevated (Figure 2). Pulmonary angiography showed multiple thrombotic masses at the level of the left superior and inferior lobar arteries, as well as in the distal right main pulmonary artery. The right superior and middle lobar pulmonary arteries were completely occluded, the right inferior lobar artery had severe proximal thrombotic stenosis, and partially recovered blood flow (Figure 2). As both main pulmonary branches were affected, two 5F Pigtail catheters were placed into the right and left main pulmonary arteries. A 25mg/50mL dilution of recombinant tissue plasminogen activator (Alteplase) was injected directly into the pulmonary arteries via catheters, with an infusion rate of 6mL/h. The infusion was continued until a total dose of 24mg of Alteplase (12mg/lung) was delivered. This low dose was considered in order to reduce the risks of complications, and was similar to that used in other recent studies [3,7]. Alongside the interventional treatment, the patient also received UFH 25000 IU/50ml at a rate of 2.8mL/h (apTT 68 sec at the start of thrombolytic treatment). During the thrombolysis the patient was monitored in the coronary care unit. Laboratory parameters, such as platelet count, fibrinogen concentration and activated partial thromboplastin time were closely monitored. Fibrinogen concentration dropped from 580.7mg/dL to a minimum value of 118.2 mg/dL at the end of thrombolysis. No thrombocytopenia was observed during or after the treatment. After 4 hours, at the end of the thrombolysis, the repeated right heart catheterization evidenced right ventricular and pulmonary artery pressures at the upper limit of normal (Figure 2). Pulmonary angiography revealed almost complete recanalization of right inferior- and all the left lobar pulmonary artery branches; the right superior- and middle lobar pulmonary arteries were partially recanalized (Figure 2). The femoral sheaths were removed after 12 hours, hemostasis was easily obtained by manual compression. No peri-procedural complications occurred.
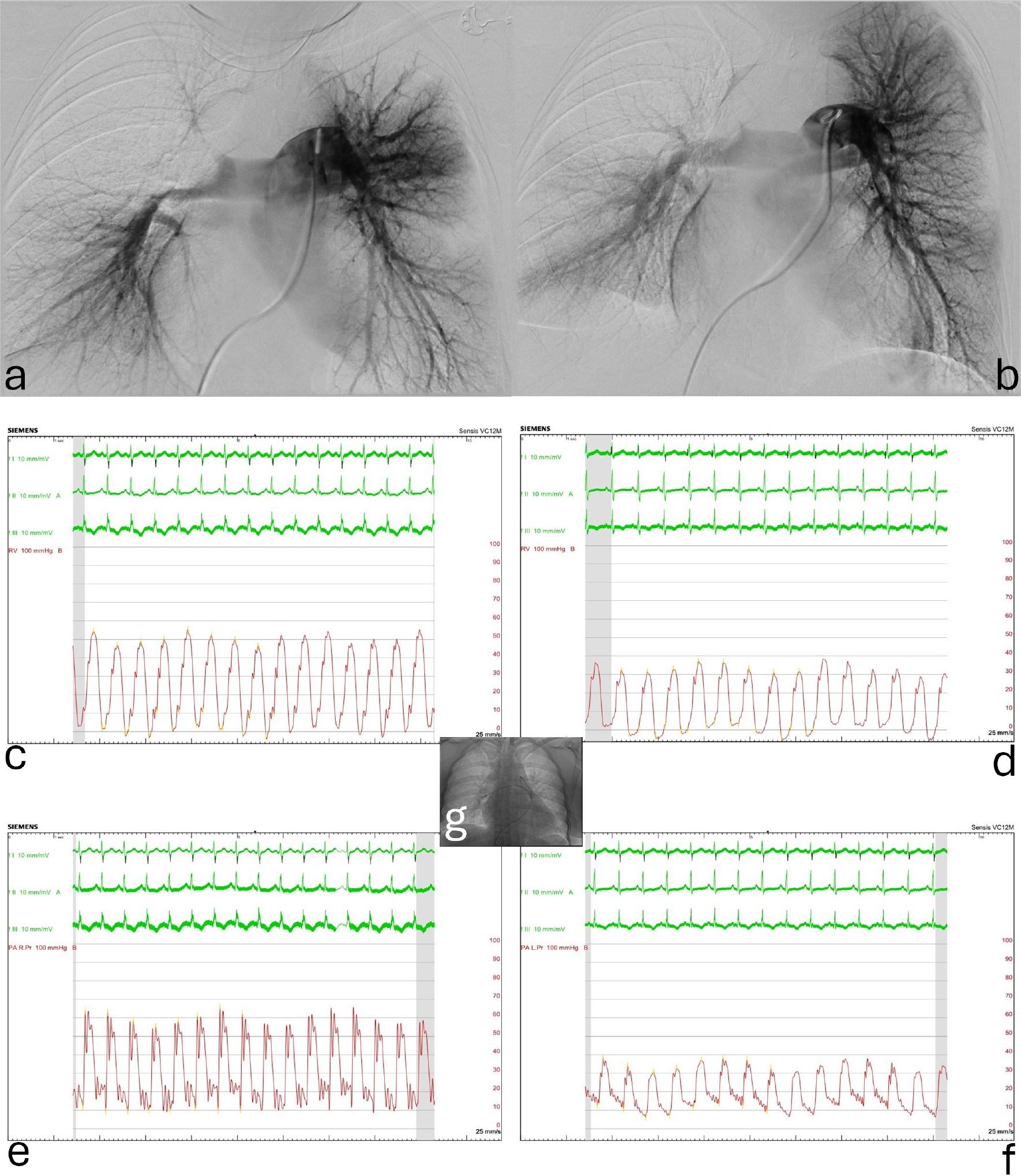
Digital subtraction pulmonary artery angiography and invasive right heart pressure recordings before and after catheter-directed thrombolysis. a. Multiple thrombi obstructing completely/partially the left and right pulmonary artery branches before thrombolysis. b. Improved angiographic appearance at the level of almost any of the lobar arteries at the end of thrombolysis; however, clots still can be identified at multiple sites. c-d. Right ventricular pressure tracings at the beginning and at the end of thrombolysis: the systolic pressure dropped from 55 to 35 mmHg. e-f. Similarly, the mean pulmonary artery pressure decreased from 31 to 19 mmHg. The embedded image (g) shows the two pigtail catheters positioned in the right and left pulmonary arteries at the beginning of the treatment.
During the following days, the clinical status of the patient has dramatically improved, with complete remission of the dyspnea and fatigue. Echocardiographic parameters for pulmonary hypertension have improved, and the overall progression of the case has been favorable. The repeated vascular echography of the lower limbs evidenced complete recanalization of ilio-femoral veins on both sides with no residual thrombotic material 48 hours after the thrombolysis. The patient was discharged on acenocoumarol (taking into consideration the patient’s option to continue breastfeeding), with a therapeutic INR range between 2 and 3, and antihypertensive treatment with enalapril and diltiazem.
During follow-up, the status of the patients gradually improved, with no signs of pulmonary hypertension at the 6-month visit. At this point, acenocoumarol treatment was discontinued and another Doppler investigation of the venous system was performed, with no signs of thrombus in the lower limbs. Under treatment, the patient’s blood pressure remained in normal range, with a heart rate of around 90 bpm, thus continuation of both Enalapril and Diltiazem was advised. The patient follows a recommendation of yearly cardiologic examinations, her and her infant’s clinical and paraclinical status is currently in the normal range, and they have a good quality of life.
This paper would like to emphasize the importance of periodically reevaluating the therapeutic algorithms for acute cardiovascular events, as technology progresses. Transcatheter delivery of drugs can dramatically change the way physicians’ approach certain diseases, increasing the overall benefits from the treatment through reduced systemic side effects. Women in the postpartum period are an overlooked category of patients in clinical trials, due to the frail psychological and physical status associated with the postpartum period, as well as unwillingness to risk deteriorating the normal development of the newborn through changes in the mother’s capability of care. This could result in physicians’ hesitation to provide novel and up-to-date medical therapies to this group of patients, even though a considerable number of cardiovascular events are associated with postpartum status. Similar to the heart team approach for decision making in clinical circumstances such as complex coronary artery disease or transcatheter aortic valve replacement, the concept of pulmonary embolism response team (PERT) was introduced [8,9]. The members of the team have different fields of expertise from emergency medicine, radiology, clinical- and interventional cardiology to cardio-thoracic and vascular surgery or even other specialties, as needed. The PERT can substantially aid the management of massive and intermediate-high risk pulmonary embolism, especially when clinical data and guideline recommendations are insufficient [9]. At this time, our pulmonary embolism team consisted of an emergency medicine specialist, a radiologist, an obstetrician, a clinical cardiologist, and an interventional cardiologist. The final decision about the management of the case was taken together with the patient herself.
Regarding local thrombolytic therapy in pulmonary embolism, several percutaneous techniques have been described. The most frequently studied are the Ultrasound Assisted Catheter-Directed Thrombolysis (UCDT) [10] and the Pigtail (Standard) Catheter-Directed Thrombolysis (SCDT) [11]. Controlled trials have shown the efficacy of these techniques in intermediate risk PE patients, with no increase in the overall bleeding risk [12]. Moreover, compared to systemic administration, catheter-directed thrombolysis was associated with a reduced risk of death, intracerebral- and other major bleeding in a recent meta-analysis [13]. In comparation with anticoagulation alone, catheter-directed thrombolysis was associated with reduced mortality and similar intracerebral- and major bleeding risk in the same work [13]. As these techniques become more widely available and routinely used by interventional cardiologists, identifying the best option for the patient has become the focus of research. Several studies compared UCDT and SCDT, with no statistically significant improvement in outcomes when using one technique over the other. In the SUNSET sPE trial, Avgerinos ED et al. showed that ultrasound fragmentation of thrombus brought no additional improvement in pulmonary thrombus reduction or pulmonary hypertension, as assessed by echocardiography, by comparison with standard catheter-directed thrombolysis [4].
Considering thrombus quantity and the impact of an intermediate-high risk PE on the clinical status and heart function of the patient, as well as the lack of improvement under conventional treatment, we presented to the patient the option of SCDT. Because these patients are usually excluded from clinical trials, in most cases there is a disproportionate lack of access to new therapies for young women. Thus, it is of utmost importance to reassess the potential benefits of the therapy and to present the patient with all the available options, so that she can make an informed decision [14].
In our particular case, the patient agreed to the procedure and a standard catheter-directed thrombolysis was performed, due to the availability of the equipment and strong evidence for the efficacy and non-inferiority of the procedure when compared to UCDT [5,15]. We would like to emphasize the importance of vascular imaging before the intervention. Echography can aid the selection of vascular access site and offers easy guidance for vascular puncture, thus minimizing the access-site related bleeding risk of catheter-directed thrombolysis. The results of the procedure were optimal, without any complication and quick improvement of the clinical situation.
As clinical status improved and discharge was scheduled in a few days, the dilemma of oral anticoagulation emerged, as there were several particularities of this case. First, the patient made a strong statement to continue lactation for the normal development of the newborn. Due to the lack of solid evidence, DOACs were not considered in the management of this patient. Low molecular weight heparin was considered, but it was finally rejected due to the administration method and high costs. As mentioned in an article from the e-journal of the ESC Council for Cardiology Practice, acenocoumarol and warfarin remain the safest and most efficient anticoagulant therapy in lactating women. Thus, the decision was made to initiate acenocoumarol with a therapeutic range for INR between 2 and 3, with good results over the upcoming months and normal development of the newborn [16].
Considering the literature and the positive outcome of our case, we consider of utmost importance to raise awareness of the potential benefits of novel medical and interventional therapies on women in the postpartum period, as they have the potential to become life-saving strategies when performed by an experienced physician in the right circumstances.
Even though encountering a postpartum woman presenting in the emergency department with a major cardiovascular event could be a frightening sight, physicians should not forget that this fragile category of patients is one of the most exposed to such events. Catheter directed thrombolysis could be an effective treatment of postpartum pulmonary thromboembolism, with a reasonable hemorrhagic risk. While medical breakthroughs occur by conducting clinical trials, this category of patients is most of the time excluded from enrollment, limiting the potential benefits of new therapies in the first few years of their approval. Thus, careful clinical assessment and more attention to details are required when dealing with this specific type of patient, while the delicate balance between potential risks and benefits should be evaluated during a shared decision-making process.