Melanoma is a rare and aggressive type of cancer that can metastasize to any organ of the body, including the heart. Cardiac metastases are reported to have an incidence of 1.6% to 20%. The most common site of cardiac metastasis is the left ventricle (41.9%), followed by the right atrium (35.5%). The most common echocardiogram findings include inflow obstruction (27.6%) and valvular dysfunction [1].
Endocardial and intracavitary metastases are uncommon, accounting for 3% to 5% of cardiac metastases on autopsy [2]. They are often misdiagnosed since they are rarely symptomatic (less than 16% of patients). Post-mortem findings show that up to 64% of patients with melanoma who did not receive immunotherapy or targeted therapy have heart metastases [3].
Patients with cardiac metastases of melanoma are usually symptomatic in case of obstruction, arrhythmia, congestive heart failure or pericardial effusion. The most common symptoms are shortness of breath (36.4%) and tachycardia (24.2%) [4]. Given that these are the most common cardiovascular and pulmonary disease symptoms, cardiac metastases are mostly diagnosed on autopsy. The best chance of early diagnosis lies in using multimodality imaging techniques. Transthoracic or transesophageal three-dimensional echocardiogram is usually performed as the initial test. Cardiac MRI, positron emission tomography and computed tomography are useful in establishing the correct diagnosis. A biopsy is needed for a definitive diagnosis, but is not always possible [5].
When transthoracic echocardiography is performed for emergency indications, as in the presented case, patients usually have unstable hemodynamics, with suspected pulmonary embolism or myocardial infarction. The current finding was interpreted as a metastasis in the heart chamber in a patient who was previously diagnosed and treated for skin melanoma.
A 67-year-old female was admitted to the emergency room with complaints of dyspnea (MRC III, saturation O2 86% without oxygen, 89% on 10L of oxygen via face mask), tachypnea (20 breaths per minute), hypotension (80/60 mm Hg), and tachycardia (102 beats per minute) on 15.09.2024. The patient experienced breathlessness for several hours. She had a history of arterial hypertension for which she received amlodipine 5 mg and Ramipril 2.5 mg. The patient was diagnosed with BRAF-mutated skin melanoma of the chest pT3aN0M0 in November 2022. She had undergone wide surgical excision in December 2022. After excision the patient received targeted therapy in a full volume.
Chest auscultation found diffuse pulmonary crackles; the cardiac auscultation revealed a diastolic murmur. The ECG showed signs of pulmonary hypertension (right axis deviation, P pulmonale) and tachycardia but without other changes. Her laboratory tests revealed mild anemia (hemoglobin 98 g/l [normal range 120-140 g/l], hematocrit 25% [36-42%]), elevated serum creatinine (353 mcmol/l [58-96 mcmol/l]), urea (15 mcmol/l [2.8-7.2 mcmol/l]), and decreased urinary output (approximately 300 ml during the last 24 hours) at the time of admission, considered a prerenal kidney failure.
The chest X-ray showed bilateral opacification of the lung field consistent with pulmonary edema (Figure 1). Echocardiography revealed a mass in the left ventricle. Figure 2 shows a hyperechoic mass of an irregular round shape with clear, uneven contours and a pronounced acoustic shadow. The mass is fixed to the posterior leaflet of the mitral valve and partially to the basal segment of the lateral wall; however, a reliable assessment of its position in transthoracic echocardiogram is difficult. Left atrium (LA) width was 40 mm (normal range [RN] = 27-38 mm). LA volume was 48 ml (NR = less than 52 ml). In the left atrium there was a hypoechogenic mass with an area of 20 × 18 mm. Left ventricle end-systolic volume (ESV) was 22 ml (NR = less than 24 ml), end-dyastolic volume (EDV) was 57 ml (NR = less than 61 ml). Ejection fraction (biplane Simpson) was 50%. Contractile function of the left ventricle in basal, mid and apical segments was normal. Interventricular septum width in inferolateral segment was 12 mm, which confirms the presence of slight hypertrophy. Left ventricular posterior wall was 8 mm. Right atrium (RA) width was 25 mm (NR less than 29 mm). RA square was 17 mm2 (NR was less than 18 mm2).
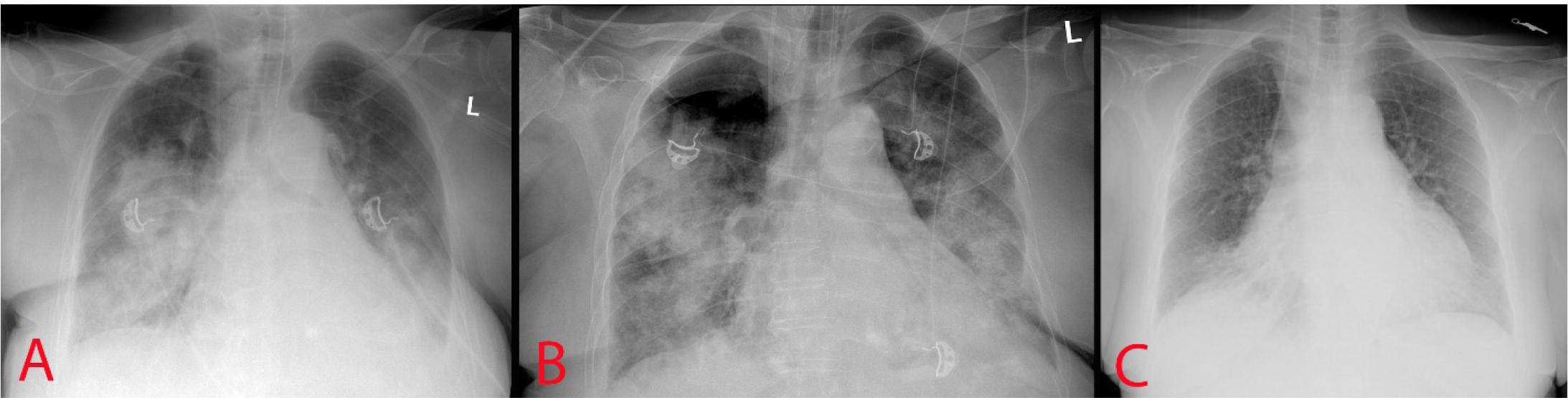
Chest X-Ray. A – at admission; B – 2nd day of admission; C – at the time of discharge.
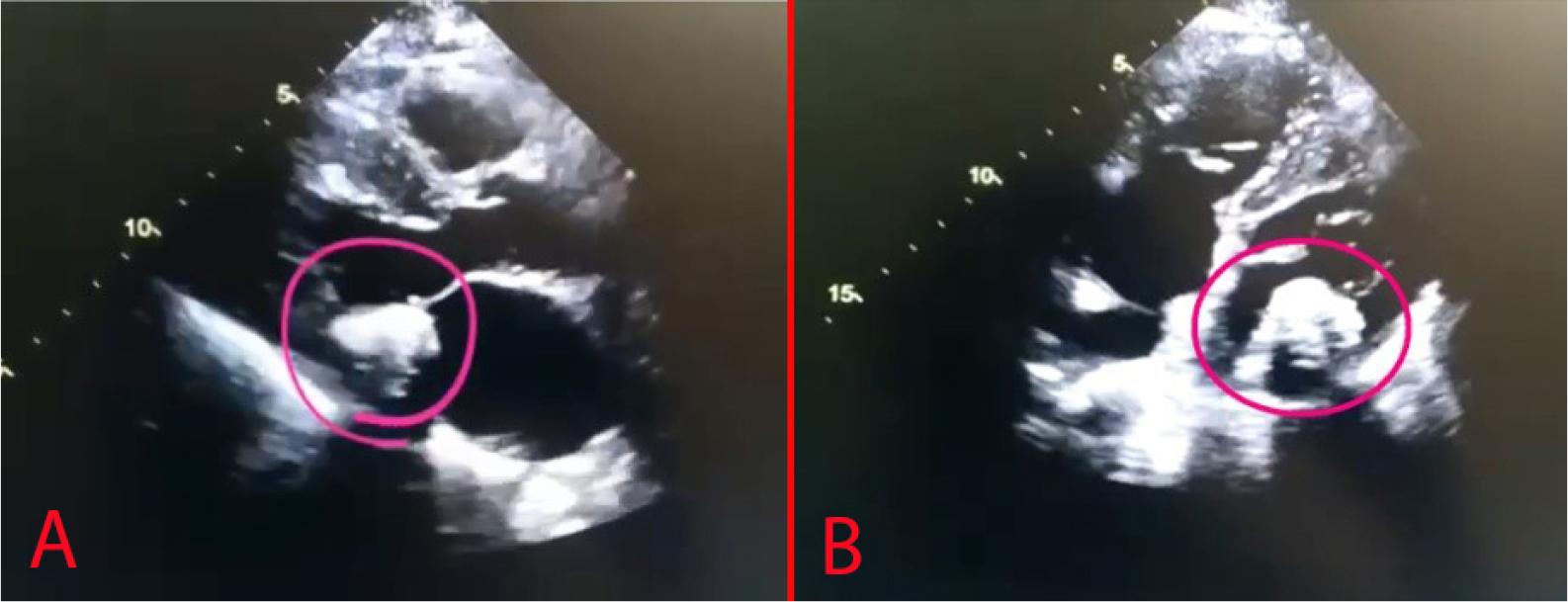
Transthoracic echocardiography (the circle marks the position of the cardiac mass).
In general, contractile function of the myocardium is up to normal: ejection fraction measured by the Simpson method was 50%. The slight hypertrophy of the left ventricular myocardium and a slight equal enlargement of the atria are also noteworthy. Her previous echocardiography was performed in September 2023 but did not reveal a tumor.
The patient did not respond to non-invasive oxygen support and continued to desaturate up to 82% O2 on oxygen insufflation and continuous positive airway pressure. Therefore, the patient was intubated and transferred to the ICU. She required intensive therapy, which lasted for 7 days, including analgesia, sedation, invasive mechanical ventilation in lung protective mode, restrictive fluid management, diuretics and hemofiltration followed by a 3-day treatment in the internal medicine department. She was discharged in a stable condition with a recommendation for immune therapy as she refused further evaluation of the cardiac mass.
It is evident that any tumor with metastatic potential can spread to the heart and can involve any of its structures or the pericardium and great vessels. The most common primary tumors to metastasize to the heart are lung cancer, breast cancer, and hematologic malignancies such as non-Hodgkin lymphoma. However, this is mostly due to the prevalence of these cancers in the population. There are several tumors that have a predilection to metastasize to the heart such as melanoma, malignant pleural mesothelioma, and mediastinal malignancies such as thymoma [6].
The management of patients with cardiac metastases remains discussable. Historically, the optimal option was a surgical resection; however, this is possible only in stable patients with a solitary metastasis. Combined therapy for the IIIA stage after melanoma progression includes anti-PD1/anti-CTLA4 immunotherapy with Nivolumab and Ipilimumab. Immunotherapy with either blockade of PD-1 or CTLA-4 therapy is based on activation of cytotoxic T cells to induce an antitumor immune response. CTLA-4 is believed to regulate the proliferation of T-cells early in the tumor response and decrease regulatory T cells. PD-1 suppresses the later-stage T cell response in the peripheral tissues [7]. If there is a progression after anti-PD1/anti-CTLA4 monoclonal antibodies in the second-line setting, then BRAF/MEK tyrosine kinase inhibitors (TKI) may be prescribed again if there has been a remarkable response after more than 6 months of first-line therapy with TKI.
Patients with cardiac metastasis have overall 30-day, 3-month and 6-month survival rates at 85%, 59%, and 51%, respectively. The average survival time is 27.33 months with continued treatment and 6.6 months in patients who do not receive treatment. However, in patients with a cardiac response to treatment the median survival time is 55.60 months [8].
Balinski and coworkers reviewed electronic medical records of outpatients with metastatic melanoma during 2009-2022, identifying patients with a clinical or histopathologic diagnosis of cardiac metastasis. Their analysis demonstrates that up to 61% of patients with cardiac metastases have at least one symptom at the time of diagnosis. The most common are fatigue (35%) and dyspnea (30%). This is usually a single mass (65-83%) in the right ventricle (23-65%), left ventricle (30-35%), or right atrium (30-35%). Approximately 48-65% of patients experience at least one cardiovascular complication within one year after the diagnosis with the most common being arrhythmia (30-35%), heart failure (22%), right ventricular obstruction (40%) and pericardial effusion (17-20%). Mortality at one year post◻ diagnosis of cardiac metastasis was 35%, and 2-year mortality was 57%. Treatment strategies for cardiac metastasis included immunotherapy (25-65%), targeted therapy (35%), radiation (25%), and surgery (15-55%) [9]. A major concern of cardiac metastases is arrhythmia, which may be fatal and requires careful evaluation [10].
Surgical management of cardiac melanoma metastases is usually performed to palliate symptoms of heart failure and outflow tract obstruction. The role of surgical management for cardiac metastases is quite limited and, if pursued, particularly for symptomatic or oligometastatic disease, should be discussed by a multi-disciplinary team. Treatment of metastatic melanoma has evolved due to the implementation of immunotherapy and targeted therapy [7]. Heart metastases usually remain silent since there are no physical signs or laboratory tests that specifically detect cardiac tumors. Therefore, pathology remains the gold standard for diagnosing such lesions, which can be obtained surgically or postmortem. Unfortunately, the risk of major surgery often does not allow proper histological evaluation and the patient is treated empirically.
Cardiac metastases are uncommon. The treatment strategy is usually based on the cancer histology. In case of melanoma targeted therapy and immunotherapy are indicated, while surgical resection is reserved for selected cases, usually to palliate symptoms of heart failure and outflow tract obstruction.