Managing acute myocardial infarction (AMI) in patients with end-stage renal failure (ESRF) presents significant clinical challenges, particularly concerning the risk of contrast-induced nephropathy (CIN) during percutaneous coronary intervention (PCI) [1],[2]. The selection of an appropriate contrast agent is crucial to minimize renal complications.
The administration of iodinated contrast media in this population carries a heightened risk of CIN, which can lead to further renal impairment and adverse clinical outcomes. Studies have shown that the incidence of CIN is significantly higher in patients with preexisting renal dysfunction, with rates ranging from 13% in general populations to as high as 57% in those with additional risk factors such as congestive heart failure [3].
Iodixanol, an iso-osmolar, non-ionic contrast medium, has been associated with a reduced incidence of CIN compared to low-osmolar contrast media (LOCM) in patients with pre-existing renal impairment. The NEPHRIC study demonstrated a significantly lower rate of CIN in high-risk patients receiving iodixanol versus iohexol, a commonly used LOCM [4].
This case report is distinctive in that it involves a patient with ESRF who declined dialysis yet underwent percutaneous coronary intervention (PCI) using iodixanol without subsequent deterioration in renal function.
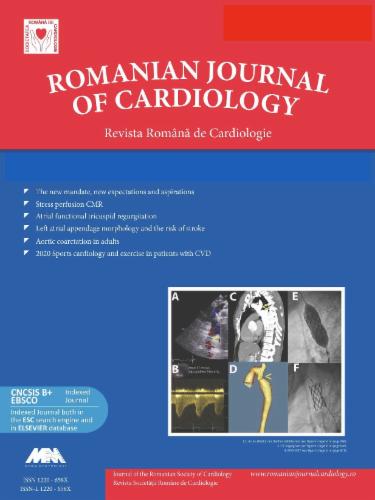
A 79-year-old male with a history of hypertension and chronic kidney disease secondary to chronic glomerulonephritis presented to the emergency department with acute, severe chest pain and diaphoresis. Initial electrocardiography revealed rapid atrial fibrillation, poor R-wave progression in the precordial leads, and a left anterior fascicular block. High-sensitivity Troponin T levels were elevated at 270 pg/mL on admission and subsequently exceeded 10,000 pg/mL. These findings led to a diagnosis of non-ST-elevation myocardial infarction (NSTEMI), and the patient was promptly transferred to the catheterization laboratory (Figure 1).
Patient’s ECG at presentation
The patient had been diagnosed with end-stage renal failure (ESRF) six months earlier but had declined dialysis initiation. On admission, his serum creatinine was measured at 319 μmol/L, corresponding to an estimated glomerular filtration rate (eGFR) of approximately 15 mL/min/1.73 m2. Given the severity of his cardiac condition, primary percutaneous coronary intervention (PCI) was deemed necessary. To minimize the risk of contrast-induced nephropathy (CIN), iodixanol (Visipaque™), an iso-osmolar contrast agent, was selected for the procedure.
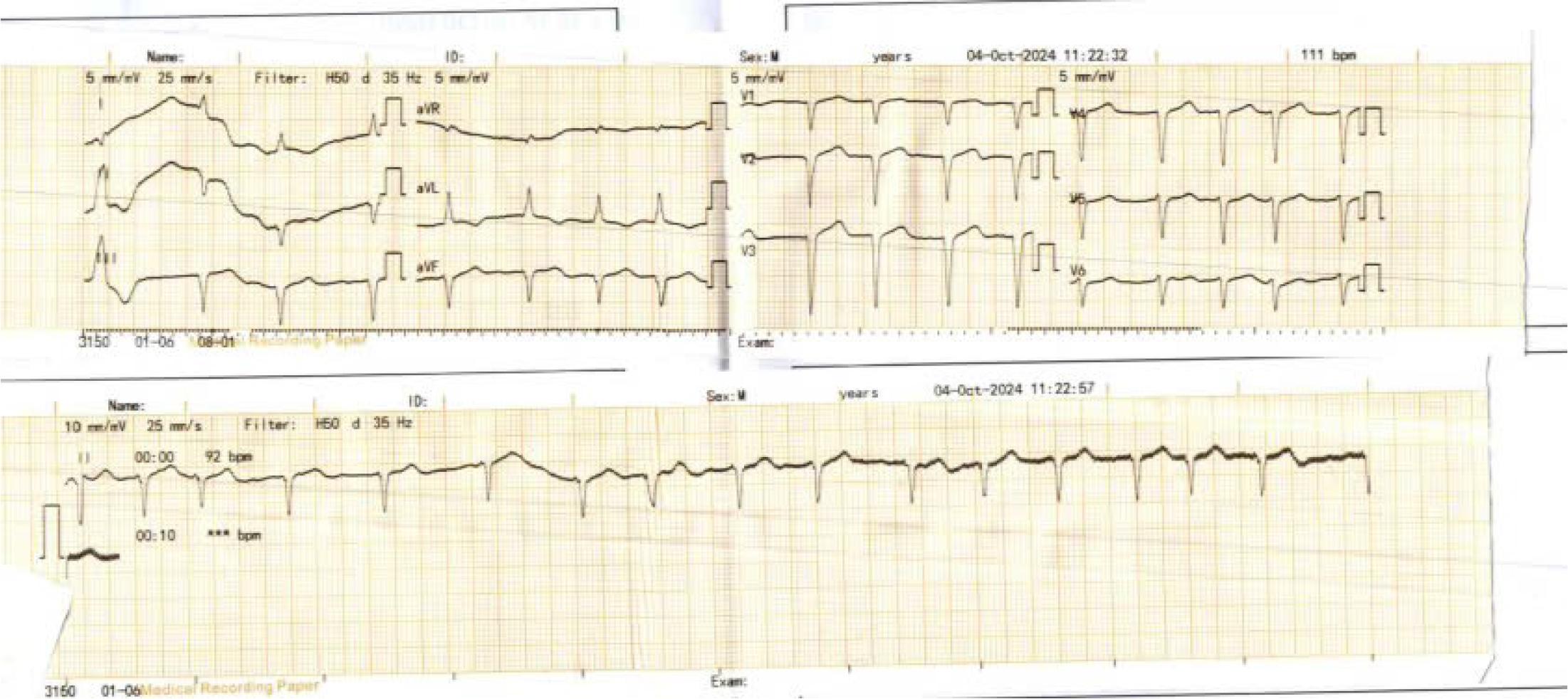
Coronary angiogram revealed stenosis of the left main coronary artery at the ostium and diffuse significant stenosis involving the left anterior descending artery, left circumflex artery, and right coronary artery with total occlusion at distal part supplied by collateral from LAD, indicative of left main and triple vessel disease (Figure 2). The patient was advised to undergo coronary artery bypass grafting (CABG). However, both the patient and his family declined further invasive treatment, citing his underlying comorbidities. Coronary angiogram was performed with the administration of a total of 40 mL of iodixanol (Figure 2).
Coronary angiogram
Following procedure, the patient was transferred to the coronary care unit (CCU) for continuous monitoring. The Mehran Score for this patient was calculated as 10, indicating a 14% risk of developing contrast-induced nephropathy (CIN) and a 0.12% risk of CIN requiring dialysis. As a result, serial assessments of serum creatinine were performed to closely monitor renal function. Within 24 hours post-procedure, serum creatinine levels increased by 92 μmol/L (1.04 mg/dL), suggesting the onset of contrast-induced acute kidney injury (stage 1 AKI). The patient was managed with intravenous fluid therapy, and urine output remained stable at 1500–2000 mL/day. Notably, subsequent creatinine measurements demonstrated a trend toward improvement, and renal function gradually stabilized. Despite these developments, the patient and his family continued to decline dialysis therapy. Renal function stabilized after conservative measures, and no further escalation of care was necessary.
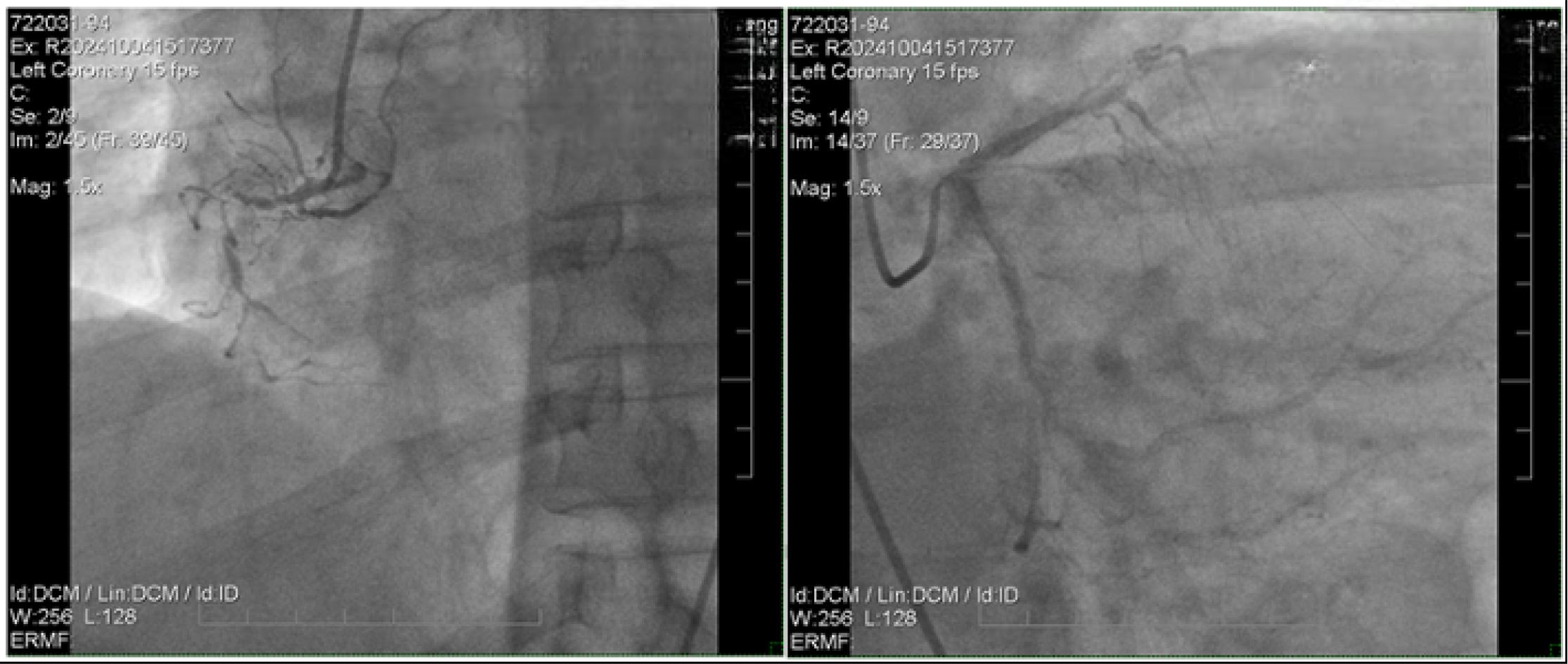
Twelve days later, the patient reported persistent angina symptoms and underwent further intervention for the coronary lesion. During the procedure, a guiding JR catheter, followed by an AL1 catheter, was used to advance a Fielder XT guidewire across the distal left anterior descending (LAD) lesion. Lesion preparation was performed using a Sapphire II Pro balloon (1.0 × 15 mm) to dilate the LAD II stenosis. However, despite balloon angioplasty, significant residual stenosis (approximately 80%) persisted, necessitating the deployment of a Combo Plus drug-eluting stent (DES) measuring 2.5 × 33 mm.
Attempts to intervene on the right coronary artery (RCA) using Runthrough, Fielder XT, and Gaia 1 guidewires with microcatheter support were unsuccessful, as the wires failed to cross the proximal stenosis. Consequently, the decision was made to address the proximal LAD lesion, where an additional Combo Plus DES (2.75 × 33 mm) was deployed. Post-stent placement, follow-up imaging confirmed TIMI 3 flow, indicative of successful revascularization (Figure 3).

LAD intervention
A total of 80 mL of iodixanol was used during the intervention procedure, and the Maximal Allowable Contrast Dose (MACD) calculated base body weight and creatinine of the patient was about 70 ml. Following the procedure, the patient was transferred to CCU for close monitoring. The Mehran Score, calculated as 10, was consistent with the assessment from the previous procedure, indicating a moderate risk of CIN. Forty-eight hours after the second PCI, the patient remained hemodynamically stable, with renal function and urine output showing no significant changes (Table 1). The patient was subsequently discharged on day five with optimized medical therapy, including dual antiplatelet therapy, a vitamin K antagonist, statins, and antihypertensive agents.
Lab test monitoring after PCI
| At the ER | 48 hours | 72 hour | 7 days | 12 days | 14 days | 2 weeks | |
|---|---|---|---|---|---|---|---|
| Ure (mmol/L) | 14.09 | 17.37 | 21.45 | ||||
| Creatinin (umol/L) | 319.8 | 319 | 411 | 427 | 420 | 315 | 309 |
| eGFR (ml/min/1.73m2) | 15 | 15 | 11.13 | 10 | 10 | 12 | 15 |
| Na+ (mmol/L) | 130 | 133 | 129 | 131 | |||
| K+ (mmol/L) | 4.46 | 4.03 | 4.21 | 3.88 | |||
| Troponin I (pg/ml) | 270.5 | 30012 | 4956 | ||||
| Urine (mL) | 1500 | 1300 | 1600 | 1300 | 1500 | 1400 | 1500 |
Managing AMI in patients with ESRF who decline dialysis presents a significant clinical challenge, particularly concerning the heightened risk of CIN [5]. The administration of iodinated contrast media during PCI is associated with the potential for acute kidney injury, a risk that is especially pronounced in patients with severely compromised renal function [6]. The use of iodixanol in patients with renal impairment has been widely investigated, with mixed results in the literature. Several studies, including the NEPHRIC trial, have shown that iso-osmolar contrast agents are associated with a lower incidence of CIN compared to LOCM in high-risk populations [4]. However, other reports, including meta-analyses, suggest comparable safety profiles between iodixanol and specific LOCMs [7],[8].
The patient in this case, presenting with ESRF and refusing dialysis, represents a unique subset of the population that is rarely addressed in existing studies. Given the severity of his cardiac condition and the lack of alternative revascularization options, primary PCI was performed using iodixanol, an iso-osmolar contrast agent, to minimize the risk of CIN. The pathophysiology of CIN involves several interconnected mechanisms. Renal vasoconstriction occurs when contrast agents disrupt the balance between vasodilators, such as nitric oxide, and vasoconstrictors, such as endothelin, leading to reduced renal blood flow and subsequent ischemic injury. Additionally, direct tubular toxicity may result from the cytotoxic effects of contrast media on renal tubular epithelial cells, causing cellular damage and necrosis [9]. High-osmolar contrast agents further exacerbate these effects by imposing an osmotic load that can induce osmotic nephrosis, characterized by vacuolization and swelling of renal tubular cells, impairing their function [10]. Iso-osmolar contrast agents, such as iodixanol, are designed to match the osmolality of blood plasma, effectively minimizing risks by reducing the osmotic load, preserving renal hemodynamic stability, and lowering cytotoxic potential, thus providing a safer profile for renal outcomes [11].
This patient, with a history of CKD due to chronic glomerulonephritis that progressed to ESRF, was at heightened risk for CIN. The Mehran score was calculated as 10 for both PCI procedures, reflecting a moderate risk. Following the first PCI, the patient developed stage 1 AKI, evidenced by an elevation in serum creatinine, though urine output remained stable, consistent with the non-oliguric presentation of CIN. The patient was managed according to the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines for AKI, which included intravenous fluid therapy and regular monitoring of serum creatinine and urine output [12]. Renal function stabilized with these conservative measures, and no escalation of care was necessary.
For the second PCI, although the Mehran score remained unchanged, the cumulative risk for CIN increased due to the short interval between procedures. Despite counseling on the benefits of dialysis in mitigating risks, the patient and family maintained their decision to decline therapy. Post-procedure, the patient was closely monitored, and fortunately, no CIN developed this time. This case underscores the challenges of managing sequential PCI in high-risk ESRF patients and the importance of individualized care and vigilant monitoring.
Managing coronary artery disease in patients with CKD requires a delicate balance between achieving optimal cardiovascular outcomes and mitigating renal risks. Preventive strategies such as adequate hydration protocols before and after the procedure, combined with vigilant post-procedural monitoring of renal function, are critical in the prevention and early detection of AKI [13]. The choice of contrast agent should also be carefully considered to reduce the incidence of CIN in high-risk populations [14].
This case report has several limitations that warrant consideration. First, it is a single-case observation, which limits the generalizability of the findings to broader patient populations. While the successful use of iodixanol in this patient is promising, larger studies are needed to confirm its safety and efficacy in ESRF patients who decline dialysis. Second, the lack of advanced imaging modalities, such as renal perfusion studies or biomarkers of subclinical renal injury, restricts the ability to fully assess the physiological impact of the contrast agent on renal function. Serial measurements of serum creatinine, while standard, may not capture subtle changes in renal health that could have prognostic significance.
In conclusion, this case contributes novel data to the existing literature by demonstrating the feasibility and safety of performing PCI using iodixanol in an ESRF patient who declined dialysis. The findings highlight the importance of individualized management strategies, especially in populations with unique clinical profiles, and underscore the need for further research to establish evidence based guidelines for similar high-risk scenarios.