Atrioventricular septal defects (AVSD) arise due to aberrant development of the endocardial cushions during fetal development, leading to a central cardiac defect. The key morphological feature of AVSDs is the presence of a common atrioventricular (AV) junction, in contrast to the separate right and left AV junctions found in a normal heart (2). Depending on morphology, AVSDs are recognized as complete or partial (Figure 5). A complete AVSD is identified by a common atrioventricular valve, typically with five leaflets, an ostium primum atrial septal defect, and an inlet-type ventricular septal defect. In contrast, a partial AVSD features separate atrioventricular valves, an ostium primum atrial septal defect frequently associated with a cleft mitral valve, or an inlet-type ventricular septal defect. A transitional AVSD is classified as a subtype of the partial form, featuring a restrictive inlet ventricular septal defect (VSD) that is sealed by the chordal attachment of the right atrioventricular valve. In patients with untreated AVSD, complications such as supraventricular arrhythmias, conduction disorders, pulmonary hypertension, and Eisenmenger syndrome may develop over time.
A 56-year-old woman with a history of uncorrected atrioventricular septal defect, pulmonary hypertension, permanent atrial fibrillation, and hypothyroidism, with repeated hospitalizations for heart failure over the years, presented to the Emergency Department for repeated syncopal episodes, dyspnea, and fatigue at usual exertion. During the two weeks prior to her Emergency Department presentation, she had experienced four episodes of syncope, each lasting a few seconds, followed by palpitations and reduced exercise tolerance. The patient did not have a family history suggestive of sudden cardiac death or recurrent syncopal episodes. Also, the patient denied previous neurological pathology. She was being treated with Acenocoumarol 2 mg daily, Furosemide 40 mg twice daily, Spironolactone 50 mg daily, and Levothyroxine 25 microg daily.
Clinical exam at admission showed a blood pressure of 140/80 mmHg, an irregular heartbeat of 80 beats per minute, and a peripheral oxygen saturation of 88%. She displayed perioral cyanosis, digital clubbing, and jugular venous distension. At cardiac auscultation a holosystolic murmur in the sixth left intercostal space was noticed, as well as a pronounced pulmonic valve closure sound with a split second heart sound.
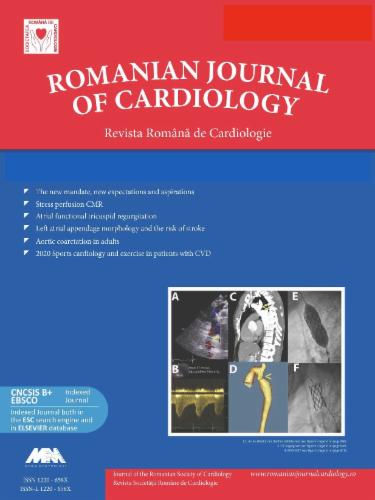
The initial electrocardiogram showed atrial fibrillation, right bundle branch block, QS complex in V2-V6, extreme right QRS axis deviation, and QTc interval of 508 ms (Figure 1).
12-lead ECG showing atrial fibrillation with ventricular rate of 72 beats per minute, right bundle branch block, QS complex in V2-V6, extreme right QRS axis deviation, and QTc interval of 508 ms.
Chest X-ray showed cardiomegaly, with prominent right inferior cardiac border, as well as suggestive signs of pulmonary hypertension.
Focus echocardiography showed absence of the interatrial septum, severe mitral regurgitation, severe tricuspid regurgitation, dilated inferior vena cava, mild pulmonary regurgitation, and moderate pericardial effusion. To rule out acute neurological pathology, a cranial CT scan with contrast was performed in the Emergency Department, which confirmed the absence of lesions in this area. We decided to admit the patient for further explorations.
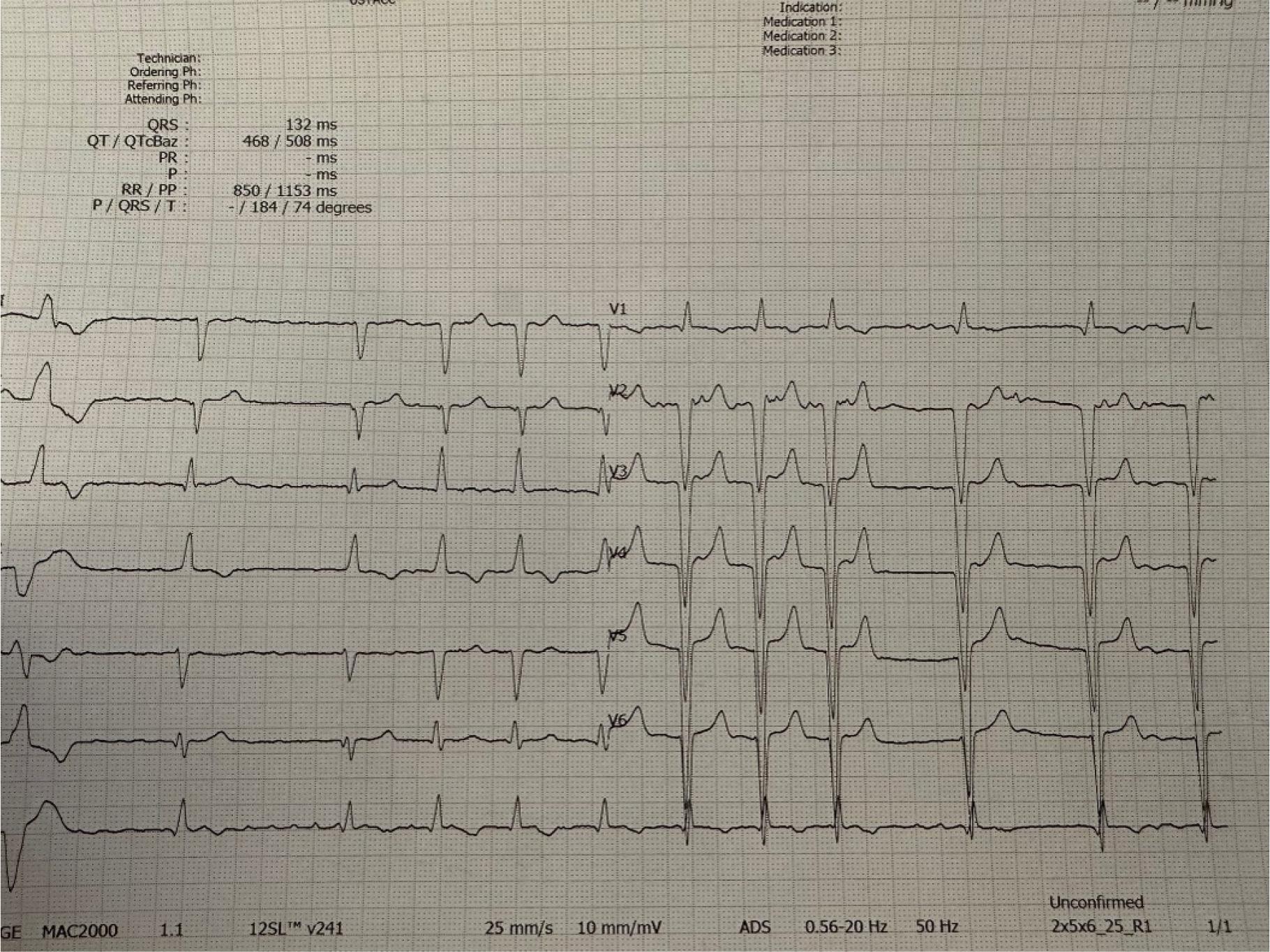
A more detailed echocardiographic evaluation was repeated and revealed a single atrium with a volume of 530 ml, severe mitral regurgitation, severe tricuspid regurgitation, perimembranous VSD with bidirectional flow on Doppler interrogation, left ventricular (LV) end-diastolic volume of 92 mL and end-systolic volume of 33 mL, LV ejection fraction of 60%, right ventricular (RV) basal/longitudinal/medium diameters of 71/89/80 mm, RV longitudinal systolic dysfunction (suggested by the tricuspid annulus plane systolic excursion of 11 mm), estimated pulmonary artery systolic pressure of 92 mmHg, Qp:Qs=3.89, dilated inferior vena cava, mild pulmonary regurgitation, and moderate pericardial effusion (Figure 2–3, video 1-2).
Transthoracic echocardiography modified apical 4-chambers view: large single atrium (A), dilated right ventricle (RV), small pericardial fluid (*), left ventricle (LV), mitral valve (MV), tricuspid valve (TV).
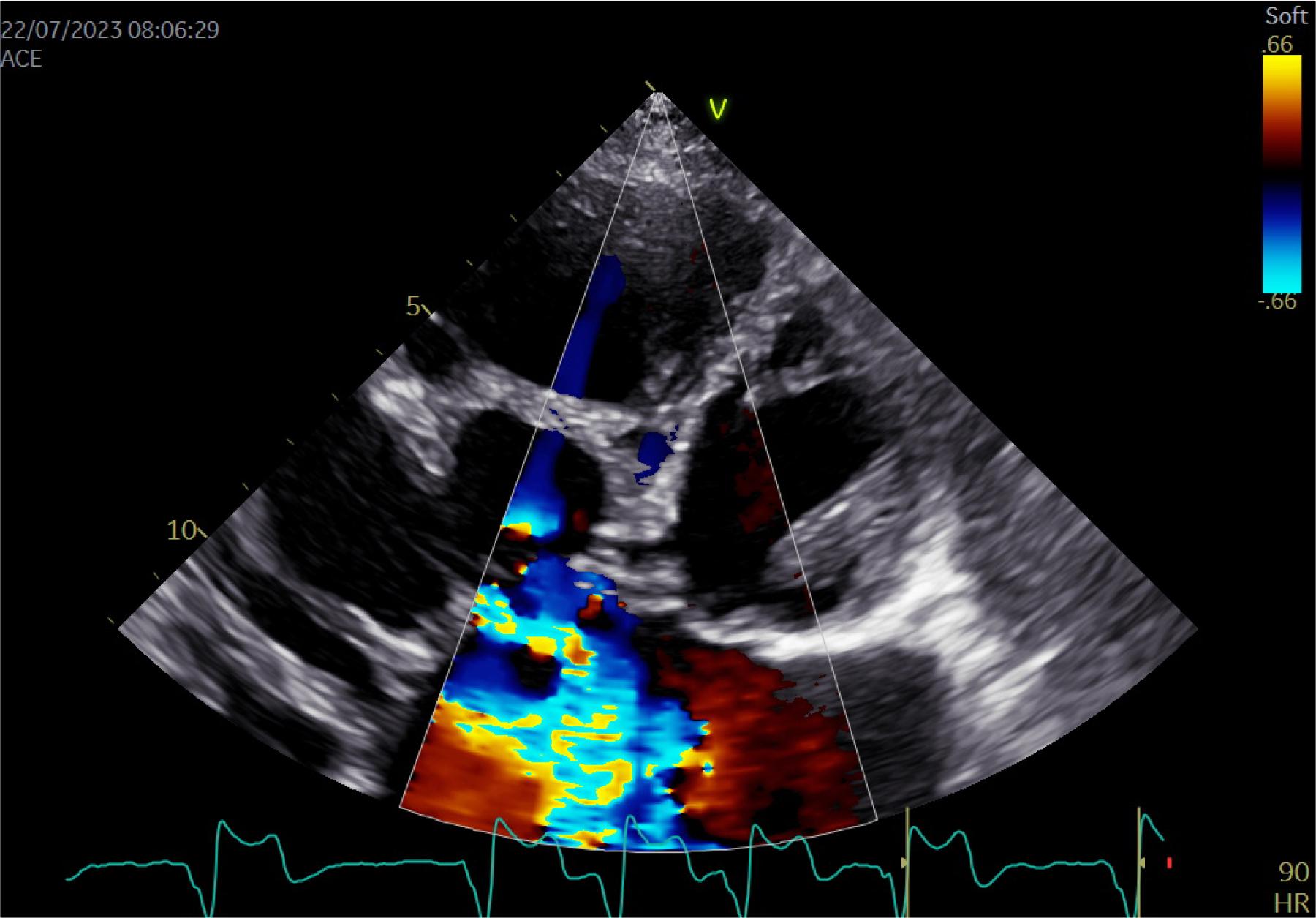
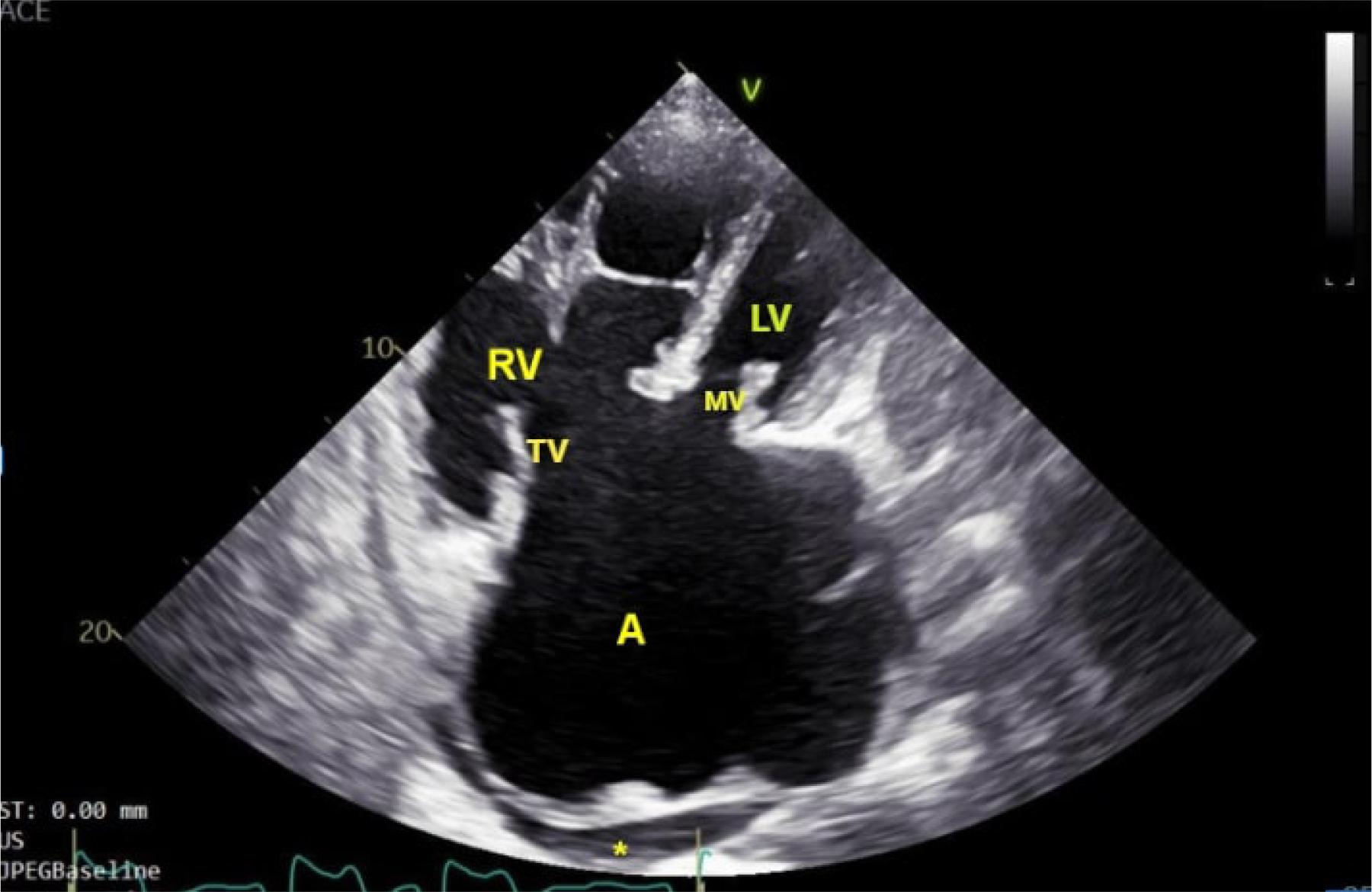
Transthoracic echocardiography modified apical 4-chambers view, color doppler: severe tricuspid regurgitation.
During hospitalization, the patient experienced repeated syncopal episodes, and upon recovery reported visual impairment, palpitations with a rapid heart rate, and reduced exercise capacity. She was not aware of the presence of any symptoms during the syncopal episodes. In the case of our patient with uncorrected atrioventricular septal defect, in which anatomical changes of the atrioventricular septal junction with a particular postero-inferior position of the atrioventricular node translate to an abnormal sequential ventricular activation and prolonged atrioventricular conduction time, atrioventricular blocks are not rare and are the first possible cause for syncope. Secondly, repeated syncopal episodes in such a patient could also be caused by a failure of the right ventricle to adapt to the increased afterload due to pulmonary hypertension caused by the uncorrected defect. Finally, the electrocardiogram at admission showed long QT interval which could be associated with ventricular arrhythmias such as Torsades des Points. In this context, a 24-hour Holter ECG monitoring was performed that revealed AF, as well as periods of asystole up to 6-7 seconds. Furthermore, given the increased prevalence of embolisms in this category of patients, an ophthalmological consultation was performed, which ruled out the presence of embolisms in the retinal vessels.
Identification of repeated asystole episodes in the absence of probable reversible causes clarified the diagnosis and established the indication for permanent pacemaker implantation.
Initially, multiple attempts were made through left cephalic approach to position a lead with active fixation at the level of the right ventricular apex, but because of the modified cardiac anatomy, atrioventricular valve regurgitations, and high intracardiac pressures, this approach could not be used. During the procedure, the patient experienced multiple episodes of ventricular fibrillation, which stopped spontaneously, caused by myocardial irritation due to the immediately dislodging lead. In the context of the unavailability of a leadless lead, a surgical placement attempt of an epicardial lead was discussed in the heart team. However, the surgical risk was considered prohibitive due to severe pulmonary hypertension. The transvenous approach was attempted in a second procedure, and we managed to place a pacing lead with passive fixation at the right ventricle apex which proved stable, the positioning of the passive lead particularly facilitated by the trabeculated myocardium (Figure 4). Acute parameters for stimulation and sensing were RV = 0.5V/0.6ms/5.6mV, RV impedance = 900 ohms. The pacemaker was programmed in VVI mode, with a base rate of 50 beats per minute and hysteresis set to 40 beats per minute.
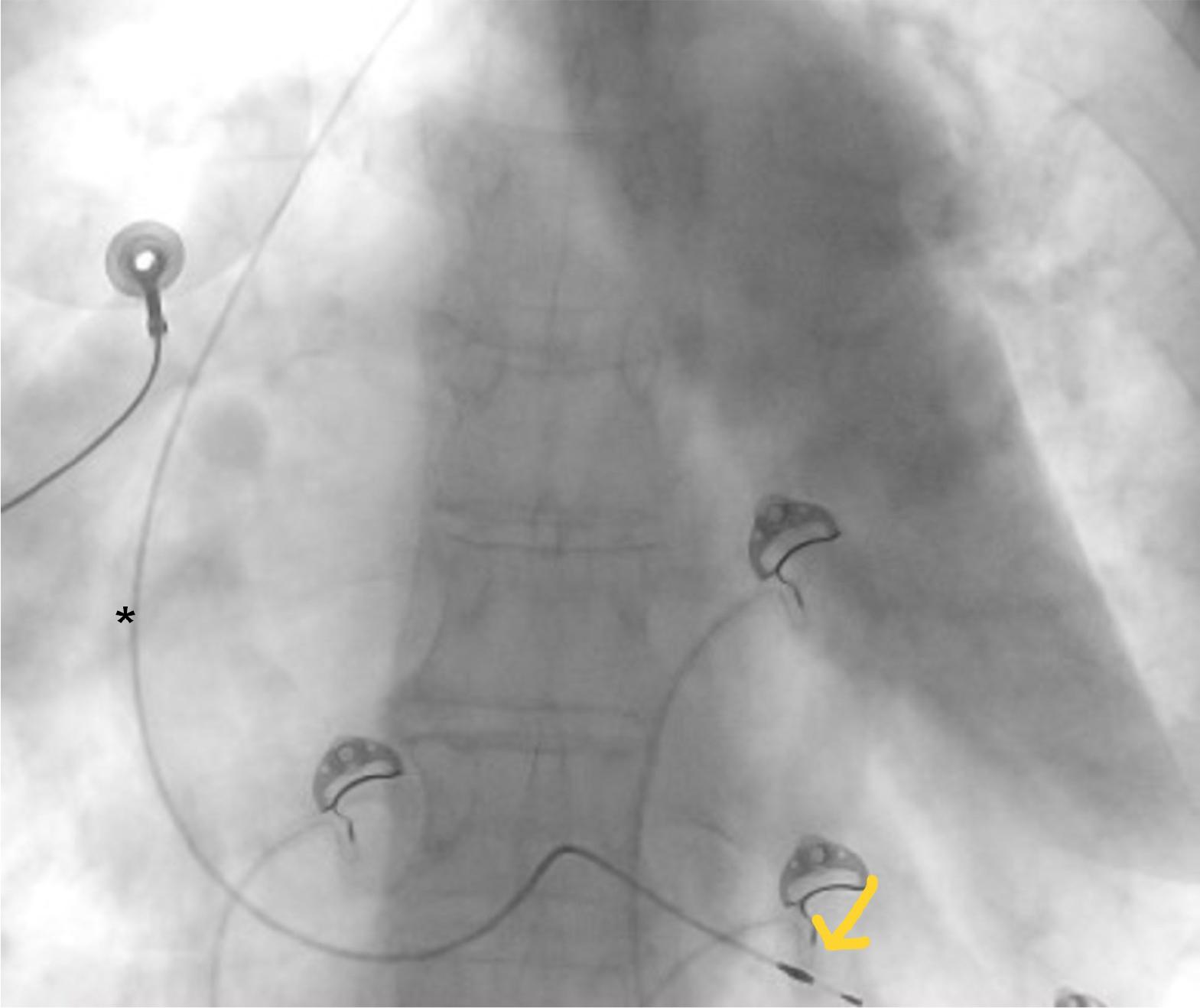
Postero-anterior chest X-ray showing the positioning of the pacemaker lead (*).
Pharmacological treatment for congestive heart failure was optimized, and oral anticoagulation continued.
The patient has not experienced any further hospitalizations due to syncopal episodes in the year following the implantation. Her baseline functional status has improved.
Atrioventricular septal defects represent 5% of all congenital heart defects, with no significant difference between male and female gender, and are frequently associated with chromosomal abnormalities such as Trisomy 21 (1). Furthermore, maternal conditions such as diabetes (2) and obesity have been proven to be associated with AVSD (3).
Depending on morphology, AVSDs are recognized as complete or partial (Figure 5). A complete AVSD is identified by a common atrioventricular valve, typically with five leaflets, an ostium primum atrial septal defect, and an inlet-type ventricular septal defect. In contrast, a partial AVSD features separate atrioventricular valves, an ostium primum atrial septal defect frequently associated with a cleft mitral valve, or a an inlet-type ventricular septal defect (4). All AVSDs exhibit shared features during routine cardiac imaging, including: lack of the AV septum; tricuspid valve loses its typical apical displacement, aligning at the same level as mitral valve; the papillary muscles appear closer due to the counterclockwise rotation of the inferomedial papillary muscle’s position; the distance from the LV apex to the aortic valve is elongated due to unwedging; and there is anterior displacement of the LV outflow tract.
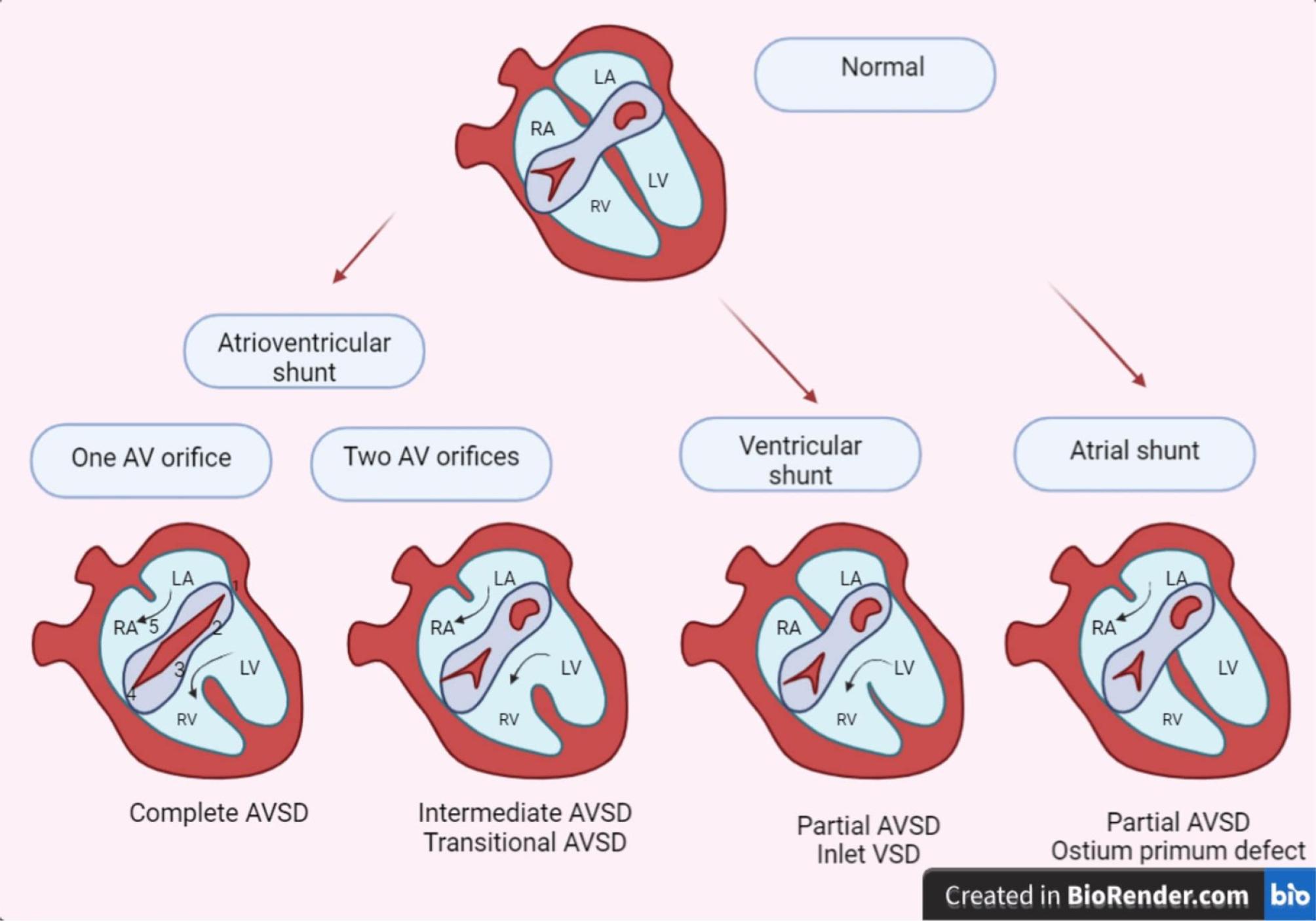
Classification of atrioventricular septal defects. AVSD atrioventricular septal defect; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; AV, atrioventricular.
Considering the existence of intricate anatomy and numerous risk factors, various mechanisms have been established to elucidate the link between congenital septal defects and arrhythmias (5), one of them being the presence of left-to-right shunt, which can result in myocardial stretching due to chronic volume overload and electrophysiological remodeling. Although certain defects are distinct from the specialized conduction structures, others can disrupt the congenital conduction system (5,6) in patients with AVSD; for example, the atrioventricular (AV) node and His bundle may be positioned more posteriorly and inferiorly than in a structurally normal heart. This abnormal positioning leads to irregular sequential ventricular activation and a prolonged atrioventricular conduction time resulting in varying degrees of AV block (7).
AV block in the congenital population may occur spontaneously over time, with higher-grade AV conduction abnormalities commonly observed in patients with ostium primum ASDs, primarily due to the anatomical proximity of the structures.
Furthermore, AV conduction abnormalities may also be found in association with AVSDs due to mutations in a group of myocardial transcription factors, such as NKX2.5, GATA4, and TBX5, which are active during early embryologic development (3).
Given the high prevalence of arrhythmias and conduction disorders, a considerable proportion of adults with congenital heart disease require cardiac rhythm management devices. The implantation of endocardial or epicardial pacemaker leads poses unique challenges in this patient population. Epicardial pacing systems offer clear benefits for patients with complex congenital heart disease. Despite being significantly more invasive, typically necessitating a thoracotomy, epicardial pacing does not depend on venous access, implantation could be made during concurrent surgery, the associated risk of thromboembolic events is much lower, and it presents fewer issues related to lead extraction. However, these factors must be balanced carefully with a greater susceptibility of deterioration over time, with a tendency to have higher capture thresholds and greater risk of lead failure (8). One of the main reasons for lead failure is trauma or tension placed on epicardial leads due to thoraco-abdominal movement, as well as the numerous cardiac surgeries often undergone by patients with congenital heart disease (CHD), resulting in an inflamed or scarred epicardium. Steroid-eluting leads enhance the effectiveness of epicardial leads, and the potentially life-threatening consequences of lead failure are somewhat mitigated by advanced technologies like transtelephonic monitoring and auto-capture algorithms, offering a level of safety during the early stages of failure (4). In contrast, permanent transvenous pacing leads are widely recognized for their association with thrombus formation where unintentional lead placement in the systemic circulation can result in embolic strokes, as emphasized in a retrospective study by Khairy et al (9).
For patients where an endovascular approach is deemed most suitable, a thorough evaluation of shunts (or potential shunts) using echocardiography or angiography should be performed prior to lead implantation (Class 1C recommendation) to assess thromboembolic risk (5). When endocardial or epicardial implants are contraindicated or deemed suboptimal, new techniques like the Micra leadless transcatheter pacing System by Medtronic, a miniaturized, single-chamber pacing device, should be considered (10).
The present case emphasizes that a multidisciplinary discussion prior to implantation is nearly always necessary, involving input from congenital cardiac surgeons, interventionalists, imaging specialists, and electrophysiologists to ensure a well-rounded approach that takes long-term considerations into account, with special focus given to residual shunt, malfunction of the atrioventricular valve, enlargement and dysfunction of the left and right ventricles, elevation in pulmonary artery pressure, left ventricular outflow tract obstruction, and arrhythmias. Our case illustrates how through multidisciplinary team planning, complications were effectively managed, minimizing morbidity and achieving favorable outcomes despite the initial challenges encountered during implantation. The diversity within the patient population necessitates that nearly every implantation decision be customized to the individual patient (11), with thorough understanding of preoperative evaluations, procedural techniques, and potential complications (12).