Transradial access (TRA) for percutaneous coronary procedures and non-cardiac interventions has demonstrated a reduced risk of vascular complications and major bleeding, including mortality, compared to transfemoral access (TFA), especially in high-risk patients.1 However, TRA has challenges, such as vascular access cross-over and radial artery occlusion (RAO).2 While RAO is often asymptomatic due to the extensive network of anastomoses in the forearm, it limits future use of the affected radial artery.3 The widespread adoption of TRA has made it the preferred vascular access site for a broad spectrum of interventions, irrespective of patient characteristics or procedural complexity.4–11
Despite significant advancements in TRA equipment, including hydrophilic sheaths and catheters, and improved procedural techniques, the crossover rate to TFA remains between 4.6% and 10%.12 The primary factors contributing to TRA failure include the small diameter of the radial artery, vasospasm, tortuosity, and complications from previous catheterizations, such as occlusion or reduced arterial caliber. Notably, the risk of RAO increases by approximately 10% with each repeated access to the same radial artery.13
When TRA is not feasible or preferred, alternative vascular access methods at the arm level, such as distal radial access (DRA), ulnar access, or brachial access, offer viable options. This paper aims to comprehensively explore and detail these alternative arm vascular access techniques as potential substitutes for conventional TRA.
In 2011, Avtandil Babunashvili introduced DRA to reopen forearm radial arteries that had occluded due to previous catheterization procedures.14 This innovative approach has steadily gained acceptance within the medical community. Interestingly, the first use of DRA as an alternative site for perioperative blood pressure monitoring was documented by anesthesiologists in the late 1970s, with reports by Amato et al.15 in 1977 and Pyles et al.16 in 1982 highlighting its application in pediatric and adult cardiac patients when conventional vascular sites were inaccessible.
Following its introduction, numerous observational studies and registries have assessed the clinical outcomes associated with DRA.4–11 More recently, randomized trials have recently compared this technique to conventional TRA.17–18 The initial investigations were primarily motivated by the need for a safe and effective alternative for vascular access, particularly in situations where TRA or transfemoral access presented challenges. Early data on DRA have been promising, showcasing its feasibility and high success rate with minimal safety concerns.19–20
The adoption of DRA has also been bolstered by social media, where its benefits have been widely promoted.21 Since 2017, when Ferdinand Kiemeneij published his initial experience with left DRA in the anatomical snuffbox, this technique has significantly increased in popularity.22 Today, DRA is not just an alternative to TRA but is increasingly used as a primary access site for various interventional cardiology and radiology procedures.23–25 It has proven effective across various percutaneous vascular procedures, with published registries and trials reporting no major safety issues.
Several registries have documented the clinical application of DRA in routine practice. Al-Azizi et al. observed a 98.3% success rate in performing DRA for diagnostic and coronary angioplasty across five operators, with no complications reported.4 Hemostasis was achieved using a conventional radial band, and no bleeding incidents were noted.
Kim et al. reported an 88.0% feasibility rate for coronary angiography and angioplasty using DRA, compared to the traditional radial approach 6. The challenges encountered in the failed cases included difficult punctures of the distal radial artery and challenging wiring. In their study, DRA was utilized for 2 patients (1.5%) undergoing emergency coronary angiography for ST-elevation myocardial infarction and for 56 patients (42.4%) with non-ST-elevation acute coronary syndrome, including unstable angina.
Achim et al. shared their extensive experience with DRA in conventional coronary and peripheral interventions involving over 1,200 patients. They reported a high success rate of 97%, achieved through ultrasound guidance in all cases.20
DRA has been effectively employed in many clinical settings and for nearly all types of coronary interventions. In the American Progress-CTO registry, Nikolakopoulos et al. compared 120 chronic total occlusion (CTO) percutaneous coronary interventions (PCI) performed via DRA with 2,625 CTO-PCI procedures conducted through TRA. Their findings indicated a steady increase in the use of DRA for CTO-PCI, which was associated with favorable outcomes.26
Despite the smaller size of the distal radial artery than the proximal radial artery, DRA has proven feasible for even large 7 Fr guiding catheters. This was demonstrated through the new RailTracking Technique. In a prospective observational registry, a long dilator Railway system (Cordis) was used to taper the entire system, reducing the entry profile of the guiding catheter. This improved the transition zone, trackability, and crossing capabilities in normal and challenging anatomies. This technique was tested in 20 consecutive complex coronary interventions, including CTO-PCI, left main coronary artery PCI, rotational atherectomy, coronary lithotripsy, and multivessel PCI, all without switching to another vascular access.27
Additionally, Gasparini et al. proposed using an introducer sheath with a reduced outer diameter, based on thin-walled specific technology such as the Glidesheath Slender (Terumo), for CTO interventions where large-bore guiding catheters are frequently necessary.28
Di Cesare et al. explored the application of distal radial access (DRA) for balloon aortic valvuloplasty in a cohort of 10 patients. This technique was utilized in cases where the distal radial artery could accommodate an 8 Fr sheath. The results were promising, with no complications reported, and a 30-day follow-up using color Doppler ultrasound revealed that the distal radial artery remained patent in 89% of the patients.29 Shortly after, the first pilot study of 32 patients receiving balloon aortic valvuloplasty via DRA only was reported, with no immediate vascular or procedure-related major events and an impressive 90% radial artery patency at 1-month follow-up 30. This method could be particularly beneficial for patients with femoral artery calcifications, those at high risk for vascular complications, or those who need the preservation of the femoral arteries during valvuloplasty bridging to TAVI.29–30
The RADCAR-DISTAL study, conducted by Nardai et al., investigated the use of DRA for carotid artery stenting in a diverse patient population, employing a sheathless coronary guiding system. The study found that all patients who underwent DRA achieved procedural success using ultrasound-guided cannulation. There was only one major access site complication reported, an arteriovenous fistula that required surgical intervention.24
The use of DRA is expanding into neuro-interventional procedures as well. It has proven effective for diagnostic cerebral angiography and for interventions addressing hemorrhagic pathology and ischemic stroke. Hoffman et al. conducted a meta-analysis encompassing seven studies with 459 procedures. Of these, 348 (75.8%) were diagnostic cerebral angiograms, and 111 (24.2%) were interventions. The meta-analysis confirmed the feasibility and safety of DRA for these neuro-interventional applications.25
The radial artery travels down the lateral side of the forearm, adjacent to the radius, and reaches the wrist. At the wrist, the superficial palmar branch of the radial artery emerges, traversing through the thenar muscles and connecting with the terminal part of the ulnar artery. Moving distally, the radial artery curves posterolaterally towards the dorsal side of the wrist. To complete the deep palmar arch, it forms an anastomosis with the deep branch of the ulnar artery.
There are two key locations for palpating the pulse of the distal radial artery and for potential vascular access. The first is the anatomical snuffbox, a triangular depression on the radial, dorsal aspect of the hand. The second is beyond the extensor pollicis longus, which forms the medial boundary of the snuffbox. The anatomical snuffbox is a three-dimensional, triangular space with distinct borders, a floor, and a roof. The floor comprises bones, including the distal radius, scaphoid, trapezium, and the base of the first metacarpal bone. The roof consists of skin. The medial and lateral borders are defined by the tendons of the extensor pollicis longus and extensor pollicis brevis, respectively. The styloid process of the radius marks the proximal border. Several structures are found within this confined triangular area, including the distal radial artery, superficial branches of the radial nerve, and the cephalic vein (Figure 1).
????
DRA has the potential to significantly reduce the risk of radial artery occlusion (RAO). This advantage can be observed in nearly all patients, regardless of the radial hemostasis technique employed, without requiring stringent protocols or extensive monitoring for transradial access (TRA) procedures.
Recent studies reported that RAO incidence within 24 hours of transradial catheterization is up to 9%. This risk is associated with several factors, including sheath size, procedural techniques, anticoagulation levels, and hemostasis methods.31–32
Flow interruption during hemostasis is a major contributor to RAO development. However, by performing the puncture distal to the superficial palmar arch, continuous anterograde blood flow in the forearm radial artery is maintained during hemostatic compression, reducing the likelihood of proximal RAO. If occlusion occurs at the DRA puncture site, the superficial palmar branch originating proximally continues to supply blood to the hand, thus protecting the patency of the proximal radial artery.33
One of DRA’s key advantages is preserving the forearm radial artery by preventing the mechanical damage typically caused by a puncture, which helps avoid occlusion. Optical coherence tomography imaging studies have demonstrated a low rate of acute vascular injury in the proximal radial artery during DRA procedures using 6 Fr guiding catheters.34 These studies observed intimal tears in only 2.2% of cases and detected non-obstructive intraluminal thrombus in 8.7% of patients. Maintaining the integrity of the forearm radial artery is critical for enabling future catheterizations, creating arteriovenous shunts, or harvesting the artery for coronary bypass grafting.
DRA presents numerous benefits compared to the traditional forearm approach. Firstly, it enhances patient comfort during the procedure, eliminating the need for forced forearm supination making radial access feasible for patients with limited arm mobility. Post-procedure, patients enjoy the freedom to move and use their wrists, as there is no venous compression from bandages, reducing the risk of venous stasis in the hands and fingers.
The likelihood of bleeding and vascular complications at the access site is minimal with distal radial access (DRA). The distal radial artery’s superficial course in the dorsal subcutaneous space makes it easy to compress and handle bleeding if it occurs. Positioned above the fascial compartments of the hand and the muscles surrounding the first intermetacarpal space, this anatomical feature also helps limit functional consequences and avoids the risk of compartment syndrome.
The guide catheter is more stable during DRA, particularly with the sheathless technique. This stability is achieved through the ergonomic positioning of the hand and the natural “fixing” of the guide catheter at the vascular access site. The mechanical force and friction between the guide catheter and the anatomical structures provide a secure fit, offering greater stability than conventional sheaths or Glidesheath Slender, which tend to be very slippery. This setup ensures the guide catheter remains firmly in place throughout the procedure, enhancing overall precision and control.
DRA significantly improves operator comfort by providing an optimal ergonomic position for the left hand and wrist. The patient’s left arm is comfortably positioned with the upper arm resting on a cushion on the left side, the forearm across the abdomen, and the hand pronated on the right groin. This arrangement allows the operator to work without bending over, which is especially beneficial for shorter operators and those working with obese patients. Additionally, the procedure is performed at the patient’s knee level, similar to the transfemoral approach, ensuring the operator maintains a safe distance from the X-ray source and minimizing radiation exposure and scatter.
DRA significantly reduces the time required for hemostasis, achieved through more straightforward and reliable compression. This benefit stems from the anatomical characteristics of the snuffbox area, where the radial artery runs superficially over a supportive bone floor. The specific anatomical features of this region facilitate effective compression, thereby minimizing the risk of complications 35.
Additionally, the absence of large venous vessels in the vicinity means there is a reduced risk of venous stasis during the compression process. This makes the procedure inherently safer for patients. The quicker and more reliable hemostasis achievable with DRA makes it particularly well-suited for outpatient PCI. Patients can benefit from the procedure’s efficiency, which allows for shorter recovery times and quicker discharges from the medical facility, thus improving overall patient throughput and satisfaction.
For patients needing multiple endovascular interventions, the ability to consistently use the radial artery (RA) for cannulation is highly beneficial. However, radial artery occlusion (RAO) has traditionally been considered a contraindication for subsequent procedures.
Opening the RAO through distal radial access (DRA) by crossing the occlusion with polymeric coronary guidewires and performing subsequent low-pressure angioplasty with small-profile coronary balloons can be advantageous in cases where numerous interventions are required, and traditional femoral access is not feasible.36–37 A pilot study provides some reassuring data in that the same coronary CTO techniques can be applied to reopen a radial CTO via retrograde DRA access, with no need for balloon angioplasty.38 The safety of directly using a sheathless catheter over the 0.0018” CTO guidewire was also demonstrated, thus reducing radiation, procedure time, and contrast injections, which may have occurred due to repeated balloon dilatations.38
Maintaining the patency of the RA from the outset with techniques like DRA can prevent the need for such complex interventions and is crucial for enabling future procedures. This proactive approach ensures the RA remains a viable access route for multiple interventions, potentially improving long-term patient outcomes.
The technique for achieving distal radial access (DRA) has been extensively detailed by Kiemeneij et al.22 To keep the dorsal area accessible, the thumb and first finger are separated by asking the patient to touch the base of their little finger with their thumb. This facilitates easier puncture. The patient’s arm is placed in a pronated or neutral position, and they are provided with a roll of 4 × 4 gauze or a small towel to hold. The arm is naturally placed across the patient’s abdomen for left radial access, with the hand positioned over the right groin.
Alternatively, the STARBoard, designed by Mark Webster (Adept Medical Ltd, Auckland, New Zealand), can be used. This radial arm board features four pivoting joints and a rotating handle, making it versatile for standard and distal radial approaches. In the distal radial approach, the handle is positioned vertically, aligning the patient’s snuffbox upward and extending the wrist medially. This setup ensures the snuffbox region faces upward, unlike the typical palmar orientation in standard radial access.
Access is obtained once the wrist is prepped, given that the vessel lies superficially. The distal radial artery is punctured in the anatomical snuffbox using a 20 G micro-puncture cannula over the needle. After a successful puncture, a flexible, soft, J-shaped 0.021- inch plastic-type mini guidewire attached to the sheath is introduced.
Following this, a 4, 5, or 6 Fr sheath is inserted over the guidewire after administering a subcutaneous injection of 1–3 mL of 2% lidocaine. Intra-arterial isosorbide dinitrate (2 cc) and heparin (5000 units) are injected through the introducer sheath to prevent radial artery occlusion. Vasodilator cocktails can be administered as per local protocols.
A through-and-through puncture is not recommended, especially when accessing the artery in the snuffbox, as the needle may contact the periosteum of the scaphoid or trapezium bones, which can cause pain (Figure 1). The remainder of the procedure should follow the same steps as a standard radial procedure, ensuring patient comfort and minimizing complications.
Ultrasound guidance is favored over tactile location because it can significantly increase distal radial artery (DRA) puncture and cannulation success rate. The recommendation for ultrasound guidance is related to several key advantages: it ensures a safe puncture with a single anterior wall crossing, minimizes the risk of tendon and radial nerve damage, and allows for precise recognition of all surrounding structures.39
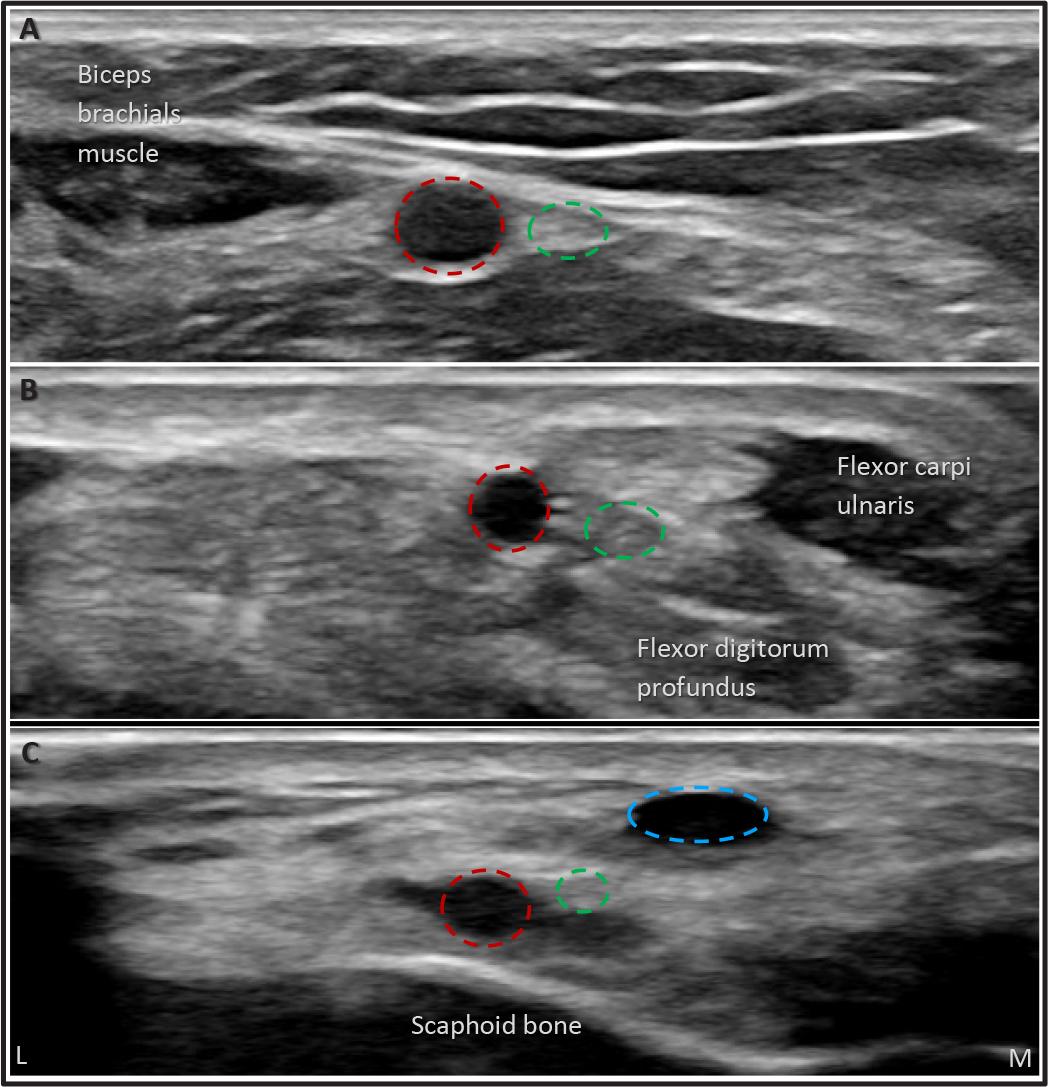
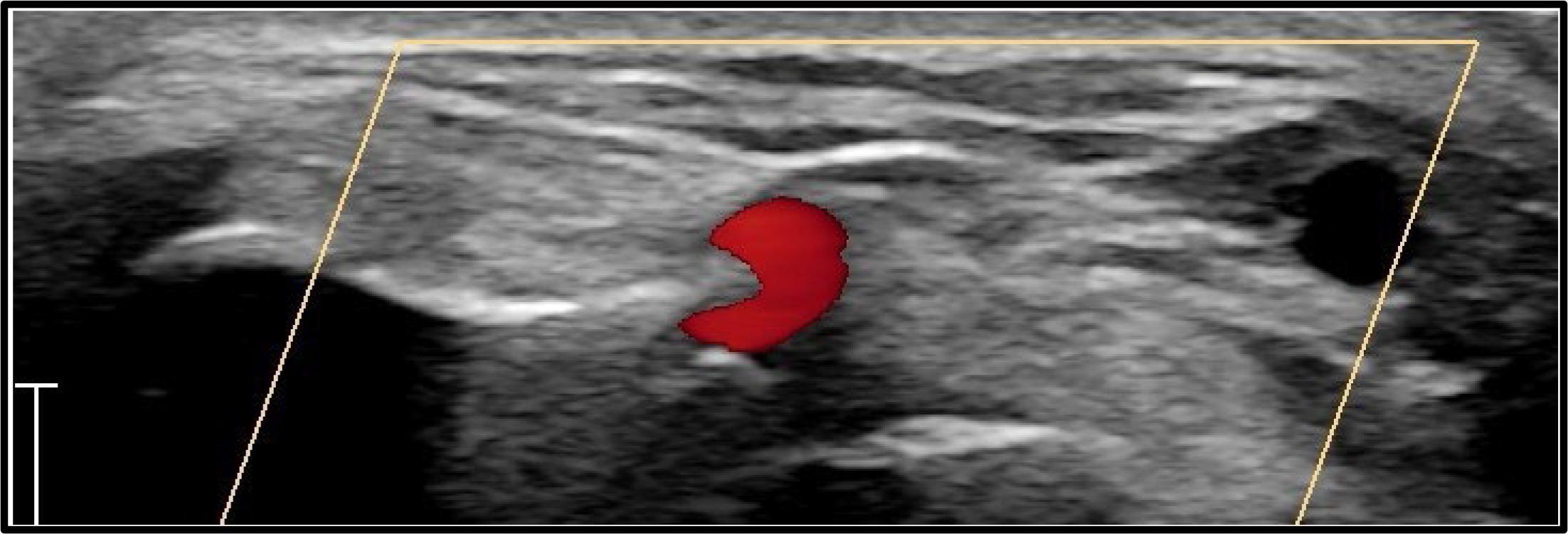
Ultrasound makes it easy to identify the scaphoid floor, extensor pollicis longus, and extensor pollicis brevis, accurately locating the distal radial artery and the optimal puncture site in a non-angulated segment, thus avoiding multiple punctures (Figure 2). Additionally, ultrasound allows the operator to measure the arterial diameter, ensuring appropriate sizing for the planned or potentially needed intervention.
Angulated segment of the distal radial artery which should be avoided during puncture. Blue dotted circle, cephalic vein.
A detailed ultrasound (US) analysis of the surrounding structures is recommended to select the optimal puncture site for distal radial access (DRA). The ideal site should be chosen based on several factors. First, the distance between the skin and the artery should be minimized to ensure the most superficial trajectory possible, facilitating easy access. Additionally, the DRA should be positioned close to a bone structure to secure effective compression and facilitate anastomosis. It is crucial to screen the surrounding structures to avoid puncturing the cephalic vein, superficial branches of the radial nerve, and, most importantly, the extensor tendons. Lastly, evaluating the tortuosity of the artery and visualizing its curvilinear trajectory in the long axis can help select the most suitable puncture site (Figure 2).
If resistance is encountered during the procedure, utilizing a 0.014 coronary workhorse guidewire can be very effective. This maneuver is considered safe if the wire movements are continuously monitored under fluoroscopy.
After the procedure, hemostasis can be achieved efficiently using either a gauze wrapped with a tight elastic bandage or a specialized hemostasis device. Presently, only one specifically designed compression device for the anatomic snuffbox is available in both right and left versions. The distal radial access (DRA) is advantageous because it is situated beyond the superficial anastomotic branches, allowing for continuous blood flow in the forearm radial artery without requiring intricate hemostasis management. However, the radial artery segment beyond the extensor pollicis longus tendon is more superficial and surrounded by small muscles, leading to potentially less predictable compression results. Therefore, targeting a true snuffbox puncture for more consistent hemostasis outcomes is advisable, leveraging the flat and supportive plane provided by the carpal bones in the snuffbox region.
Despite its numerous advantages, DRA has certain limitations. One of the primary challenges is the more difficult puncture process, which requires overcoming a learning curve. Compared to TRA, DRA involves a longer cannulation time, requires more puncture attempts, and has a higher rate of access site crossover. These issues currently represent the significant drawbacks of this newer arterial access method.
A randomized trial highlighted these challenges, showing that DRA access and procedural times were longer than conventional TRA (120 seconds vs. 75 seconds for access time and 14 minutes vs. 11 minutes for procedural time). The crossover rate to an alternative access site was significantly higher in the distal TRA group (21.8%) than the conventional TRA group (5.5%), primarily due to difficulties inserting the sheath wire. These higher crossover rates can be attributed to the distinct anatomical features of the radial artery. The distal part of the radial artery is 0.3 to 0.6 mm smaller in diameter, making arterial puncture and sheath wire insertion more challenging. These anatomical differences contribute to the increased difficulty in successful cannulation with DRA.
To overcome some of these limitations, ultrasound-guided puncture could be a viable solution. Another important consideration is the need for specialized equipment due to the anatomical challenges associated with DRA. When standard methods fail, improving the coaxial alignment between the catheter tip and the vessel route and minimizing the gap between the catheter tip and the wire can be beneficial.
The Railtracking (RTT) method is designed to address these issues. Its stiffness helps straighten tortuous anatomies, enhancing coaxiality while maintaining good maneuverability.40 The primary advantage of RTT is the tapered transition zone between the guidewire and the catheter tip, which reduces friction between the devices and the vessel wall, eliminating the razor effect. RTT can be used in two ways: with or without the introducer sheath, having the potential to decrease the need for vascular access crossover.
Since its adoption, forearm arterial access has managed to easily improve patient safety and comfort while significantly decreasing vascular complications and the economic burden that came along with the femoral route.41 TRA heralded this radical shift through its intuitive advantages, such as easily palpable and superficial course at the wrist level and the support of adequate boney structures for proper hemostasis. However, the incidence of unsuitable radial arteries for catheterization reaches up to 11%, mainly due to factors like a spasm or anatomical variants such as loops, tortuosity, small caliber, and high bifurcation.42–43 Consequently, maintaining the desire to preserve the advantage of forearm access, the ulnar artery (UA) became the next best alternative, decreasing the crossover rates to transfemoral. Transulnar vascular access (TUA) was first reported in 2001 by Terashima et al.,44 and proved feasible. Since then, accumulating evidence revealed the safer course of switching to TUA in cases of TRA failure, as opposed to contralateral radial or femoral crossover.45–46 Thus, TUA became increasingly attractive as a bailout forearm vascular access.47–49
Both radial and ulnar arteries arise from the division of the brachial artery below the elbow. The UA is the larger of the two branches and presents with a straighter course on its way to the hand. The line that connects the medial epicondyle of the humerus to the lateral aspect of the pisiform bone largely reflects the trajectory of the artery, which advances along the medial half of the forearm, deep to the median nerve, and in close vicinity to the ulnar nerve. In the mid-third of the forearm, the artery is covered by flexor muscles. At the same time, in the distal third, it progresses lateral to the tendon of the flexor carpi ulnaris muscle, still in close medial proximity to the ulnar nerve, which can be easily traumatized during vascular access attempts (Figure 1). After crossing the pisiform bone, the UA divides into two branches with the radial artery, forming the superficial and deep palmar arch. With the wrist in a hyperextended position, the UA can be palpated proximal to the pisiform bone, on the anteromedial aspect of the proximal wrist fold, remarking the deep-seated position, particularly when compared to the radial artery.
The same general principles used to cannulate the radial artery are employed for the UA. However, irrespective of the experience level with other arterial access sites (including radial artery), UA cannulation assumes a specific learning curve.50 The particularities arise from several anatomical considerations: i) the deep course of the artery beneath the flexor tendons, which makes it less likely to be accurately palpated, ii) its proximity to the ulnar nerve, which makes the puncture more prone to nerve irritation/injury, iii) absence of posterior bony structures which otherwise might have contributed to better hemostasis.
In a hyperextended wrist position, the puncture site is identified on the proximal wrist fold, proximal to the pisiform bone (Figure 2). Care should be taken to the risk of ulnar nerve injury. Using the precise location of the maximal pulse prominence or ultrasound guidance, the puncture is performed using the Seldinger technique using a 21-gauge needle, through which a 0.021-inch soft wire is passed. The sheath of the desired size (up to 7F) is then inserted over the wire. Certain degrees of possible vasospasm can be prevented using routine vasodilators such as intraarterial nitroglycerin or verapamil, while heparin administration reduces the occurrence of arterial thrombosis (2500-5000 IU). As a final step, after the termination of the procedure, the sheath is removed, and local hemostasis is obtained using either TR-band (Terumo, Tokyo, Japan) or other improvised basic compression devices. Given the deep-seated position of the UA, if a TR-band device is used for hemostasis, a higher inflation pressure is needed compared to radial artery hemostasis.47
As mentioned above, transradial access becomes unsuitable in a various number of cases due to spasm or certain anatomical circumstances.42–43 Additionally, occlusion of the radial artery can occur in up to 10% of cases 51 hindering the possibility of reutilization for cardiac interventions or as an arterial conduit for coronary artery bypass. UA has a larger caliber, a smaller anatomic propensity for loops, and fewer adrenergic receptors, making spasm less probable.52 Given the crossover rates from TRA to transfemoral ranging between 4.6% and 10%, considering the UA as the alternative crossover site confines the vascular access to the forearm in up to 99.5% of the cases.48
Since the first description of the ulnar artery access feasibility,44 a growing number of studies from 2005 until around 2015 attempted to evaluate the procedural success and the complication rate of TUA 47,49,53–67. Due to the large heterogenicity between these studies, there is no uniform data from which adequate extrapolations can be made. For example, even in studies involving larger number of patients (number of patients above 400)49,54,59,60 the success rate for TUA varies widely between 67.7% and 98.5%. In contrast, the crossover rate (i.e., failure of TUA access) varies from 32.3% to 1.5% 49,54,59,60. Some authors attribute these large variations to improper patient selection and inexperienced TUA operators.68
Similarly, mixed conclusions appear even when considering randomized controlled trials (RCTs) published over the years about TUA compared to TRA. The AURA of the ARTEMIS study, the first large RCT involving 462 patients, concluded that TUA should not be regarded as an alternative to TRA, given the higher crossover rates of 26.34% compared to TRA (p = 0.004).60
These findings were considered rebutted by other RCTs which concluded that TUA represents a safe alternative to TRA, including for primary PCI.62–63 A large meta-analysis published in 2016 evaluated data from 5 large RCTs involving a total number of 2744 patients.69 Herein, the comparison between TUA and TRA revealed similar rates of MACE (RR 0.87; 95% CI 0.56–1.36) and no difference between complications related to the access site [RR 0.92 (0.67–1.27); p= 0.62]. No differences were reported in total procedure time or fluoroscopy time. However, significantly higher crossover rates and number of puncture attempts were noted in the TUA.69
An updated meta-analysis was performed after the publication of the largest RCT, which included 2532 patients 50. Despite the larger number of patients evaluated, the results of this meta-analysis revealed similar rates of MACE and access-site-related complications compared to the previous one 50, 69 However, in this updated analysis, there was no significant difference for access-site failure between TUA and TRA (although numerically more in the TUA group).50
Despite the reasonable evidence showing that TUA is feasible and safe, it remains underutilized, given the larger adoption of TRA and, more recently, DRA. Given the higher expected rates of failure and possible complications compared to TRA, there is little reason to utilize TUA as the default access site. However, ulnar access can represent a decent alternative when radial access is unattainable, particularly when compared to femoral crossover.
Regarding the utility of ipsilateral TUA (i.e., patients with known chronic RA occlusion and patients with failed TRA access in which subsequent RA occlusion becomes a possibility), there is limited data to support the safety of this approach. Indeed, there is some evidence suggesting the lack of notable adverse events for TUA in cases of known RA occlusion.49 However, given the lack of multiple studies on this subject, significant heterogenicity must be anticipated, comparable to the overall literature on TUA. Therefore, it is the authors’ opinion that ispilateral TUA should be avoided when safe options are available, and it might become of value only in particular situations when all other options have been exhausted.
Transbrachial access (TBA) has evolved from the initial method of cutdown followed by arteriotomy to percutaneous catheterization by Quint and colleagues using a modified Seldinger technique starting in 1976.70 This was then followed by published reports describing the appropriate brachial access technique and its feasibility.70 Similar to wrist access, it became attractive given its benefit of maintaining the advantages of arm access when TRA or TUA were not feasible while offering particular strengths such as larger caliber, predictable anatomy, or the length accessibility benefit when revascularization is intended for aorto-iliac or femoral disease.71 Compared to TFA, TBA states its superiority is in terms of early ambulation, patient comfort, and the availability of a viable access site for treatment when severe ilio-femoral disease is present.72 However, given its anatomy, TBA catheterization is theoretically more susceptible to vascular and neurological complications. This was further suggested by early studies, which revealed complication rates ranging from 7-11%73–74 up to 36%,75 consisting mainly of bleeding events, pseudoaneurysms, and neurological complications. In light of the continuous progress that allowed the predominant adoption of wrist arterial access, TBA maintains a smaller role in rather isolated procedural scenarios, bearing in mind the non-negligible force of tradition of each center.
BA represents the anatomical extension of the axillary artery, standing as the main artery of the upper extremity. Its trajectory starts at the inferior border of the teres major muscle, advancing along the ventral side of the arm towards the cubital fossa, giving rise immediately below the elbow to its two terminal branches. BA is contained within the brachial fascial compartment alongside the brachial vein and the median nerve, indicating the anatomical basis for the higher propensity to develop TBA compartment syndrome (Figure 1). The artery is best palpated above the bifurcation against the medial epicondyle of the humerus.
The puncture site is located medially, just above the elbow crease, above the medial epicondyle of the humerus, at the maximum pulsation region. Performing the puncture below this point arrives with the risk of hematoma, given the lack of proper structure against which compression can be performed. Ultrasound guidance can facilitate the puncture by identifying the proper puncture site above the medial epicondyle at the most superficial location of the artery (Figure 1). The single puncture technique is used with a 21-gauge needle, through which a 0.021-inch soft wire is passed. The sheath of the desired size (up to 7F) is then inserted over the wire. Heparin anticoagulation (2500-5000 IU) is mandatory, given the risk of periprocedural thrombosis. Since vasospasm is not an issue, spasmolytic agents are not required. BA hemostasis remains challenging, given the lack of a proper bony structure. The sheath removal is followed by manual digital compression (duration dependent on the anticoagulation status), continued by compression devices such as an elastic bandage, which should still allow distal perfusion. The total duration of hemostasis should be restricted to less than 4-6 hours. At present, there are no vascular closing devices suited for TBA. However, there are positive reports on the off-label safety of several femoral closure devices employed on the BA.76–78 Given the lack of reasonable data confirming the safety of closure devices on BA, the authors cannot recommend their usage in these settings, irrespective of the sheath sizes.
As mentioned above, early reports on TBA raised doubts about its safety.73–75 Nevertheless, the current literature on this topic is rather controversial,79 highlighting the role of a learning curve and the available versatility when defining certain endpoints. One of the largest studies available included 4955 patients and analyzed three different approaches for percutaneous coronary interventions: TBA in 1102 patients (22.2%), TRA in 2797 patients (56.4%), and TFA in 1054 patients (21.2%).80 There was a higher total procedural success for the TBA and TRA groups compared to TFA (98% vs. 98.4% vs. 95.6%, P = 0.0001). Additionally, the highest rates of access site major hematoma were recorded in the TFA (1.2%) compared to 0.3% for TBA and 0.1% for TRA (p< 0.05). TFA also revealed numerically the highest rates of MACE compared to TBA and TRA (2.6%, 1.9%, 1.2%, p = 0.008). Major access site hematoma was observed predominantly in the TFA group (p=0.0001). The authors concluded that considering both safety and efficacy, TBA is a good alternative to wrist access compared to TFA.80
Similar conclusions were drawn from a different study, including patients with failed TRA, assigning them to TBA or TFA as bailout.81 There were no significant differences between the two approaches regarding bleeding rates or other access site-related complications.79 A recent publication with a similar inclusion protocol revealed TBA’s safety, efficiency, and overall non-inferiority compared to TFA in bailout situations after TRA failure.82 In studies where TBA was used for percutaneous revascularization of lower-limb artery disease, the overall complication rate was 16.7%, mainly minor events (local hematoma – 14%) with a rate of major events of 2.7% (arterial thrombosis) 83. Similarly, considering the low rates of major complications, these results determined the authors to conclude the utility of TBA as a safe alternative in peripheral revascularization.84 As it would seem intuitive to conclude, sheath size is a good predictor of local vascular events related to TBA. A study, which included patients with peripheral procedures, revealed an overall complication rate of 10.6% for TBA, with values ranging from 5.4% in cases where a 5F sheath was used, up to 12.4% for 6F and 12.5% for 7F (p=0.49).82 Other predictive factors for complications related to TBA seem to be determined by age and female gender.85 Ultrasound guidance is a decisive factor in the TBA success rate while significantly decreasing complications.76
The overall utility of TBA is limited not only by higher rates of potential complications but also by the convenience of alternative access sites. In cases where wrist access and the TFA approach are unattainable, TBA can offer a reasonable substitute. TBA remains of greater utility for peripheral revascularization, particularly for aortoiliac and proximally located femoral lesions.
In conclusion, alternative access sites such as distal radial, transulnar, and transbrachial are increasingly important for PCI, offering solutions when radial or femoral access is not viable. DRA reduces the incidence of radial artery occlusion and improves patient comfort. At the same time, both TUA and TBA serve only as bailout options, with TBA accommodating larger sheath sizes but carrying higher complication risks. Mastering these techniques is essential for managing complex cases and improving patient outcomes.