A 55-year-old man with a history of hypertension presented with breathlessness and a persistent cough. An electrocardiogram revealed complete heart block with a broad QRS complex, and he was admitted for further investigation. The combination of complete heart block with chest radiography showing bilateral hilar lymphadenopathy raised the initial suspicion of sarcoidosis, as these are classical manifestations of the disease. Routine blood tests were within normal range, while thyroid function tests and Lyme serology were negative. A transthoracic echocardiography (TTE) demonstrated a dilated left ventricle with preserved systolic function, a bicuspid aortic valve with moderate stenosis and regurgitation, and moderate mitral regurgitation. Chest radiography showed bibasal interstitial shadowing and bilateral hilar lymphadenopathy (Panel A). A high-resolution computed tomography (CT) showed bilateral hilar mediastinal lymphadenopathy and micronodules consistent with sarcoid lung disease, with perilymphatic spreading (Panel B). A cardiovascular magnetic resonance (CMR), on a triple inversion recovery (oedema) sequence, demonstrated multiple areas of an increased myocardial signal in the inferolateral, inferior wall at midcavity level, and in the lateral basal segment (Panel C), indicative of active cardiac sarcoidosis, while the late gadolinium study showed multiple subepicardial and mid myocardial areas of enhancement (fibrosis) (Panel D). While the presence of a bicuspid aortic valve was noted, there is no known association between bicuspid aortic valve disease or mild aortic regurgitation in the pattern of myocardial fibrosis observed on the CMR in this case.
Following a discussion in the MDT, cardiac resynchronization therapy with a defibrillator (CRTD) was implanted, given the extent of myocardial scarring and concern about potential deterioration of biventricular function with the right ventricular pacing alone. While current guidelines, including the 2024 AHA statement on cardiac sarcoidosis,[1] indicate that a definitive diagnosis requires myocardial biopsy, the diagnostic yield of an endomyocardial biopsy in cardiac sarcoidosis is notably low, and new histological criteria are still being proposed.[2] In this case, the risk-benefit ratio of biopsy was considered unfavorable, given the compelling multimodality imaging findings. Despite its high cost and limited accessibility, Fluorodeoxyglucose-positron emission tomography (FDG-PET) CT was performed as per UK guidelines, which designate it as an essential investigation for establishing disease activity and monitoring treatment response.[3] After a deliberate two-week delay, it showed extensive active sarcoidosis, including pulmonary, widespread-nodal, splenic, and skeletal sites, as well as extensive cardiac involvement (Panel E). Based on these findings, immunosuppression therapy was initiated, with plans for subsequent imaging to assess treatment response, as is current practice following steroid initiation.
This case illustrates the importance of multimodality imaging for the diagnosis and management of patients with sarcoidosis. [4] TTE can be used for monitoring progression once a diagnosis of cardiac sarcoidosis is established,[4] while the extent of LGE on CMR is important for risk and prognostic stratification.[5] FDG-PET has emerged as an essential tool for assessing disease activity and monitoring response to immunosuppression.[6] Ongoing research involving advanced imaging techniques, such as speckle-tracking echocardiography and hybrid CMR/PET imaging, holds the potential to provide additional insights.[6][7] However, complex imaging is not universally available, and in a constrained-resource setting only selected patients should be evaluated, after exclusion of other, more common pathologies.
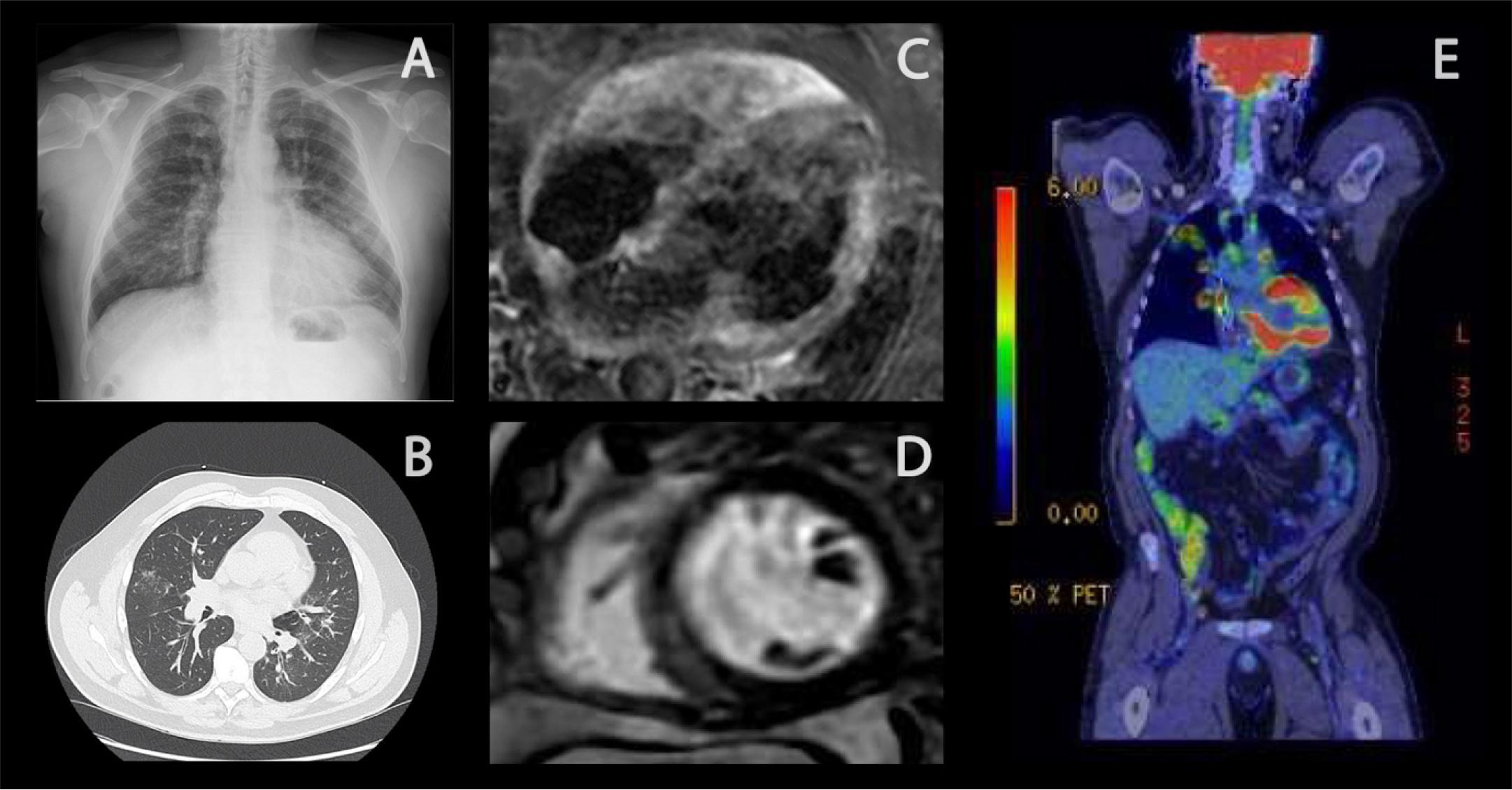
(A) CXR showing bilateral hilar lymphadenopathy. (B) HRCT with micronodules with a perilymphatic distribution, resulting of discrete, confluent, or cluster distribution. (C) Triple IR (oedema) imaging demonstrating multiple areas of increased myocardial signal. (D) Gadolinium study demonstrating multiple subepicardial and mid-myocardial areas of LGE (E) FDG-PET CT with apical pulmonary infiltrates and hilar lymph node involvement and extensive lymphadenopathy from the cervical area to the retroperitoneum. Markedly increased uptake in myocardium and nodular moderate uptake in the splenic parenchyma indicative of extensive active sarcoidosis with cardiac involvement. CXR, Chest radiography; HRCT, High-resolution computed tomography; LGE, Late gadolinium enhancement; FDG-PET CT, Fluorodeoxyglucose-positron emission tomography.