
Figure 1
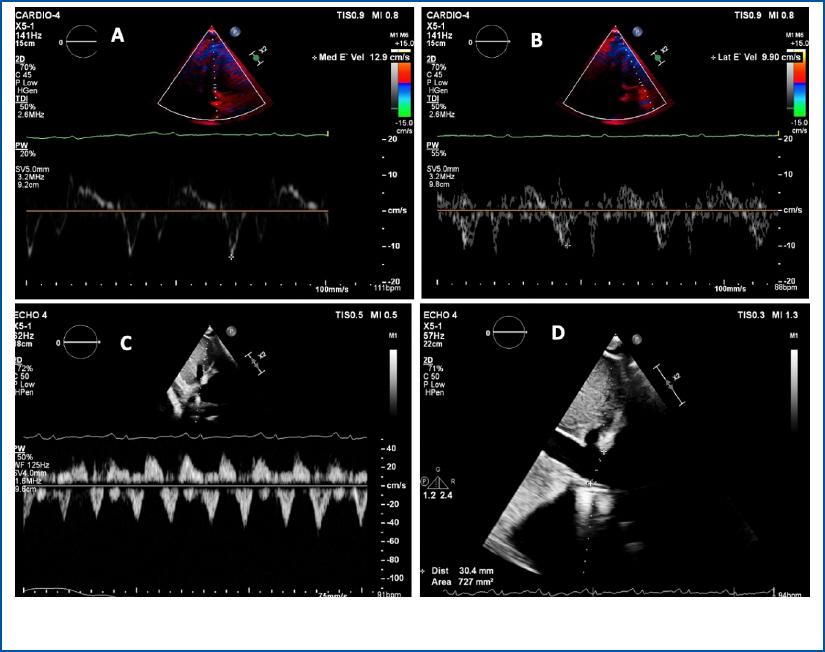
Figure 2
Figure 3
Figure 4
Previous investigations and medical history_ GI – gastrointestinal; TTE – transthoracic echocardiography; LVEF – left ventricular ejection fraction; ESR – erythrocyte sedimentation rate; hs-CRP – high-sensitivity C-reactive protein; UNL – upper normal limit; ANA – antinuclear antibodies; dsDNA – double strand DNA antibody; CCP – cyclic citrullinated peptide antibodies; cANCA – diffuse staining antineutrophil cytoplasmic antibodies; pANCA – perinuclear staining antineutrophil antibodies; ADA- adenosine deaminase; LDH – lactate dehydrogenase; ACR – albumin creatinine ratio
| March 2020 | Ascites | Paracentesis with fluid analysis: transudate |
| October 2020 | Right pleural effusion Ascites | ESR: 83 mm/h; hs-CRP: 52 ng/ml |
| April 2021 | Bilateral pleural effusion Ascites | ESR: 88 mm/h: hs-CRP: 45 ng/ml |
| May 2021 | Bilateral pleural effusion | QuantiFERON test: negative |
| March 2022 | Lower limb edema | 24 h proteinuria: 355 mg |
| November 2022 | NYHA class III | Referral to our clinic |
TTE diastolic function assessment_ Notice that the E/E’ is abnormally low (annulus paradoxus) and that septal TDI velocities have higher values than the ones sampled from the lateral wall (“annulus reversus”)
| E | A | E/A | Septal E’ | Lateral E’ | E/E’ (avg) | Septal S’ | Lateral S’ |
|---|---|---|---|---|---|---|---|
| 70 | 55 | 1.3 | 12.9 | 9.9 | 6.14 | 8 | 6 |