
Figure 1
Figure 2
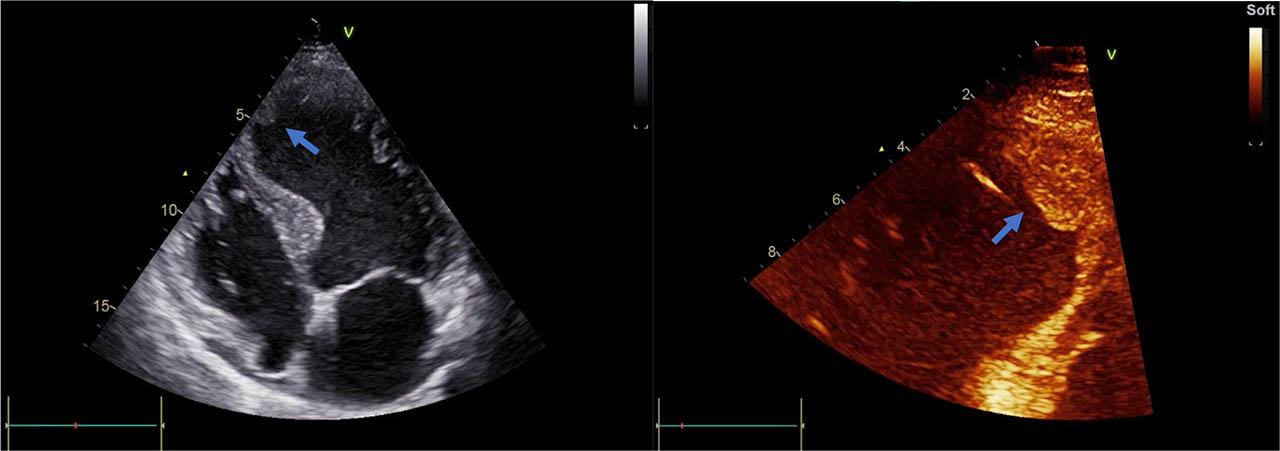
Figure 3

Guidelines for management of left ventricular thrombosis
| LVT | Recommendation | |
|---|---|---|
| STEMI Guidelines | ||
| ACC/AHA-201313 | ||
| Patient with STEMI and | DAPT+VKA with INR target 2–2.5 | |
| ||
| ESC 2012 | ||
| LVT | VKA for a minimum of 3 months | |
| ESC 201715 | ||
| LVT | Anticoagulation should be administered for up to 6 months guided by repeated imaging | |
| Stroke Guidelines | ||
| AHA/ASA 201416 | ||
Patient with ischemic stroke or TIA:
|
| |
| AHA/ASA 202117 | ||
| Patient with stroke or TIA: | ||
|
| |
| CHEST guidelines | ||
| ACCP 201218 | ||
| Patient with anterior MI + LVT/high risk for LVT | ||
|
| Then discontinue warfarin and continue DAPT for up to 12 months as per ACS recommendation |
| Patient with LV systolic dysfunction + LVT without CAD | VKA for 3 months with INR target 2–3 | |