
Figure 1
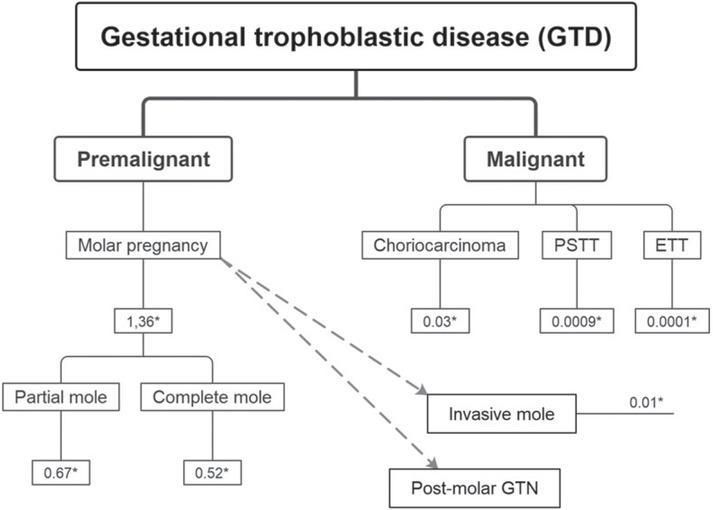
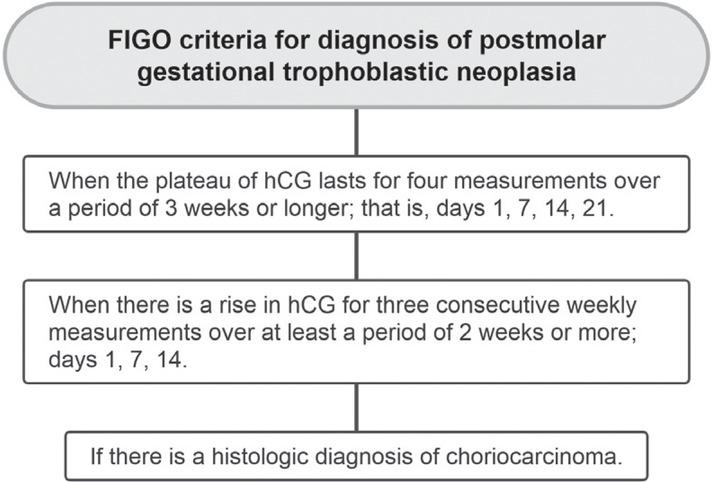
Figure 2
Ongoing clinical trials involving treatment of gestational trophoblastic disease
| Trial Drug Design | Reg. Nr. | Recruitment status | |
|---|---|---|---|
| Immunotherapy | Camrelizumab combined with apatinib for recurrent resistant GTN | NCT04047017 | Completed |
| Pebrolizumab for resistant GTN | NCT04303884 | Not yet recruiting | |
| Camrelizumab combined with apatinib in patients with high-risk GTN | NCT05139095 | Not yet recruiting | |
| Avelumab combined with methotrexate for low-risk GTN | NCT04396223 | Recruiting | |
| Avelumab in chemo-resistant GTN | NCT03135769 | Completed | |
| Camrelizumab combined with bevacizumab in high-risk GTN after combined chemotherapy | NCT04812002 | Recruiting | |
| TRC105 and/or bevacizumab in refractory GTN | NCT02664961 | Terminated | |
| Chemotherapy | Paclitaxel plus cisplatin vs EMA-CO in high-risk GTN | NCT02639650 | Unknown |
| Rescue regimen with MTX vs high-dose MTX protocol in persistent GTN | NCT03280979 | Unknown | |
| Pemetrexed disodium as salvage therapy for failed low-risk GTN | NCT00096187 | Terminated | |
| Dactinomycin in patients with persistent or recurrent low-risk GTN | NCT00003688 | Completed | |
| Single dose MTX vs MTX and Actinomycin-D single dose vs MTX multiple courses | NCT01823315 | Unknow | |
| Biweekly actinomycin-D treatment vs multi-day methotrexate in low-risk GTN | NCT04562558 | Recruiting | |
| Methotrexate vs dactinomycin in low-risk GTN | NCT00003702 | Completed | |
| Methotrexate for prevention of postmolar GTN | NCT01984099 | Completed | |
| Dactinomycin vs methotrexate in low-risk GTN | NCT01535053 | Completed | |
| Chemotherapy vs follow up in hydatidiform mole with lung nodule | NCT03785574 | Recruiting | |
| Pemetrexed in recurrent or persistent low-risk GTN | NCT00190918 | Completed | |
| Methotrexate vs methotrexate plus actinomycin in low-risk GTN patients with score 5-6 | NCT03885388 | Recruiting | |
| Surgical treatment | Hysteroscopic repeat curettage vs methotrexate in low-risk GTN | NCT03703271 | Recruiting |
| Total abdominal hysterectomy and methotrexate vs methotrexate plus folinic acid | NCT02606539 | Unknown | |
| Second uterine evacuation vs chemotherapy in low-risk GTN | NCT04756713 | Recruiting | |
| Second curettage in low-risk, non-metastatic GTN | NCT00521118 | Completed | |
| Single evacuation vs double evacuation of mole | NCT01630954 | Unknown |
FIGO staging and classification for gestational trophoblastic neoplasia24
| FIGO stage | Description |
|---|---|
| I | Gestational trophoblastic tumours strictly confined to the uterine corpus |
| II | Gestational trophoblastic tumours extending to the adnexa or to the vagina but limited to the genital structures |
| III | Gestational trophoblastic tumour extending to the lungs and may or may not involve the genital tract. |
| IV | Gestational trophoblastic tumours extending to all other metastatic sites |
Ultrasound characteristics of partial hydatidiform mole (PHM) versus complete hydatidiform mole (CHM)13,16,18
| Feature | CHM | PHM |
|---|---|---|
| US characteristics | Enlarged uterus filled with a heterogeneous predominantly echogenic mass with several hypoechoic foci (snowstorm appearance), multiple small anechoic cystic spaces varying in size from 1 to 30 mm (cluster of grapes). Theca lutein cysts presenting as multiple large, bilateral, functional ovarian cysts can be present. | Subtler US changes. Hydropic changes of some villi are often not visible before 10 weeks of gestation. Enlarged placenta relative to the size of the uterine cavity with internal cystic changes producing a “Swiss cheese pattern” is often seen. Theca lutein cysts are infrequent. |
| Foetal parts | Absent, except in the rare event of a CHM with a coexisting diploid twin. | Present as amorphous echoes. If a foetus is formed, it carries a typical spectrum of severe abnormalities. Growth retardation is common. |
| Colour-Doppler power of the uterus | Variable | Variable |
World Health Organization scoring system based on prognostic factors modified as FIGO score24
| FIGO score | 0 | 1 | 2 | 4 |
|---|---|---|---|---|
| Age | <40 | >40 | - | - |
| Antecedent pregnancy | Mole | Abortion | Term | |
| Interval from index pregnancy, months | <4 | 4–6 | 7–12 | >12 |
| Pretreatment hCG IU/L | <103 | >103–104 | >104–105 | >105 |
| Largest tumour size including uterus, cm | - | 3–4 | ≥5 | - |
| Site of metastases including uterus | Lung | Spleen, kidney | Gastrointestinal tract | Brain, liver |
| Number of metastases identified | - | 1–4 | 5–8 | >8 |
| Previous failed chemotherapy | - | - | Single drug | Two or more drugs |