Intraoperative radiation therapy (IORT) [1,2,3,4,5,6] is a cancer therapy modality that delivers a precise, high dose of radiation directly to the tumor bed, thereby minimizing the risk of geographical errors. IORT can be implemented using high-energy electrons or photons with varying energies. X-ray radiation systems produce low-energy photons that are quickly attenuated in soft tissues. Due to their low energy, the radiation dose rapidly decreases, resulting in reduced exposure to normal tissues during breast irradiation and minimizing the need for radiation protection for medical personnel. The objective of radiation therapy is to destroy cancer cells while sparing as many healthy cells as possible.
As a consequence of the interaction between ionizing radiation and matter, a dose of this radiation is deposited in a given substance. This dose can be defined as the amount of energy that a particle deposits in living matter (tissue, organ). The unit of absorbed dose in the SI system is the gray (Gy): 1 Gy = 1 J/kg. In radiotherapy, it is often referred to as the dose in water, as most tissues in the body have similar radiological properties to water (with exceptions including lungs, bones, and teeth) [7].
Ionizing radiation can arise from either indirect ionization (charged particles) or direct ionization (photons). Photons, as they traverse through a medium, undergo attenuation – a process driven by scattering, the photoelectric effect, the Compton effect, pair production, and photo-nuclear interactions. In radiotherapy, the deposition of dose is primarily influenced by the photoelectric effect, the Compton effect, and pair production. The chance of each of these events depends on the energy of photons, the density, and the atomic number (Z) of the medium.
The photoelectric effect dominates for low-energy photons (<100 keV), and the probability of photon interaction through the photoelectric effect in a medium with a given density increases with the Z3 of the medium. All the energy of photons is transferred to one of the inner atomic shells. The ejected electrons continue their path in the medium with kinetic energy equal to the initial photon energy minus the binding energy of the electron.
In the case of Compton interaction, photons interact with electrons from valence shells. In this collision, the photon loses some energy, causing its wavelength to lengthen. Simultaneously, the photon changes its direction of motion to conserve momentum. The probability of this interaction in a medium with a given density is approximately independent of the atomic number of the medium and dominates for photons with energies around 1 MeV.
For high-energy photons (>1.022 MeV), the process of electron-positron pair creation occurs. The probability of pair production for a medium with a given density is proportional to Z.
Dose control is achieved using detectors, including commonly used active detectors such as ionization chambers and silicon detectors, measuring real-time dose rates [8]. This implies that ionization chambers and silicon detectors measure the dose rate at a given moment. For assessing the accumulated dose at a specific spatial point, passive detectors are employed and dosimetric films are particularly valuable for this purpose. Commercially available photochromic films, such as Gafchromic®, respond to various types of radiation, including X-rays, gamma rays, electrons, protons, and UV radiation [9]. Due to their high spatial resolution, close tissue equivalence (
Polymerization occurs in Gafchromic films upon irradiation, resulting in the darkening of the exposed film. Result interpretation is relatively straightforward and is conducted using a scanner. The image is converted to optical density and then transformed into dose. Since the maximum absorption for different film types is 635 nm for EBT and 675 nm for MD-55, the red channel is the most suitable for reading the results [11]. The suggested dose range for MD-55 spans from 0.1 Gy to 80 Gy, whereas the ideal dose range for EBT lies between 2 cGy and 800 cGy.
This work encompasses calibration techniques and results in interpretation nuances, shedding light on the efficacy of dosimetric tools. The primary goal of these studies is to enhance the accuracy of radiation dose measurements, a critical prerequisite for ensuring patient safety in radiotherapy. To optimize dose measurements, we employed both radiochromic films and ionization chambers. Since we use the X-ray as a source, we utilized an X-ray tube developed at the National Centre for Nuclear Research, chosen for its modern applications in cancer radiotherapy [12]. The objective of this therapy is to eradicate micro-lesions of cancer cells while simultaneously minimizing the dose delivered to healthy tissue. Achieving synchronous fulfillment of these requirements is challenging. Monitoring radiation dose in cancer radiotherapy is crucial for patient safety. One technique for dose measurement involves the use of radiochromic films, known for their nearly tissue-equivalent composition. As part of the analysis, the focus was on dose distribution concerning the distance between the X-ray radiation source and the detector. This study not only explored dose measurements in air for Gafchromic MD-55-V2 and Gafchromic EBT, but also conducted comparisons with ionization chamber AP values and Monte-Carlo simulations. Water dose measurements for EBT films were compared with readings from ionization chamber PTW-23342, revealing consistent responses between MD-55-V2 and EBT films and ionization chambers. The investigation included exploring the relationship between optical density and dose for Gafchromic foils, affirming the red channel as the optimal readout. A separate study demonstrated the dependence of optical density on the day of reading after exposure for EBT films, highlighting the significance of timely film reading within the initial 2 days. Dosimetric films are, therefore, crucial tools for spatially assessing cumulative dose. Beyond medical applications, the versatility of dosimetric films extends to diverse scientific and industrial domains, solidifying their indispensable role in radiation detection and safety assessments.
The dose distributions of an X-ray tube with a 3 μm thick silver anode were measured in air and water. The X-ray tube has been designed and developed at the National Centre for Nuclear Research as part of the low-energy accelerator with an X-ray tube for brachytherapy InLine PN50 project. The compact X-ray generator was created using transmission X-ray tube technology and comprised two components: (1) electronics (power-control unit) and (2) the X-ray tube.
The power-control unit is powered by an external 12 V DC power supply with a current of up to 1 A. The accelerating voltage and beam current can be infinitely adjusted. The primary component of the X-ray generator is the electron gun, which was modified and manufactured at NCBJ. It consists of a cathode, control electrodes, accelerating electrodes, a focusing electrode, and an anode.
The control electrode is designed to manage the intensity of the electron flux, achieved by applying a voltage between the control electrode and the cathode. A negative voltage on the control electrode concentrates the electron beam, directing electrons toward a single point. The accelerating electrode, along with the control electrode, interacts with the electrons, pulling them out of the cathode space and giving them higher speed, while also focusing the electron beams. The focusing electrode acts like a lens, concentrating the electron beam.
The first anode is positioned behind the accelerating electrode, and its high voltage accelerates the electrons, allowing them to travel further at a higher speed. Bombarded by the focused electron beam, the silver emission layer on a beryllium disc generates X-rays. The emission layer is sputtered onto the disc, and the electron beam's focus incident on the emission layer is <0.5 mm.
The X-ray generator weighs 0.835 kg and is 430 mm long. The diameter of the power and control unit is 55 mm. The anode element is 190 mm long and 8 mm in diameter, while the emission disc has a diameter of 5 mm. In this measurement, the X-ray tube operates with a voltage of 50 kV and an anode current of 20 μA.
The station of the dosimetry films device, designed and manufactured at NCBJ, is simple to set up and easy to use (Fig. 1). The device comprises:
- –
the X-ray generator holder (adjustable perpendicularly using the knob),
- –
the tank for the water phantom,
- –
the table where the water phantom tank is placed (horizontally movable in one direction),
- –
the radiochromic film holder (on the table),
- –
radiative screens (copper screens on two sides, back and upside, and a lead window in the front).
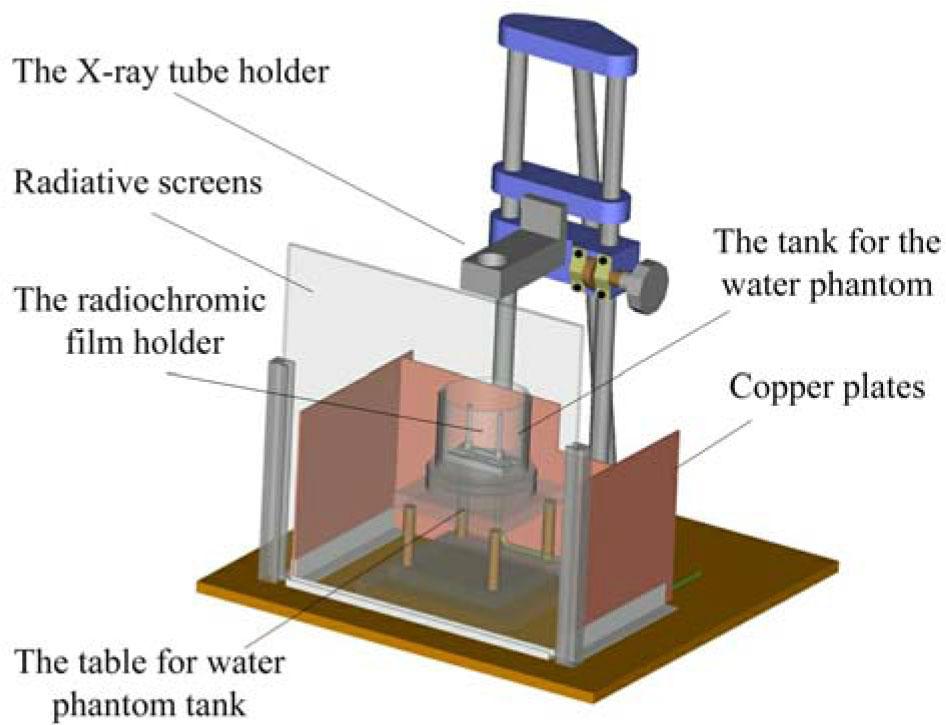
Measurement station for determining dose distribution in air and water.
Measurements were conducted using ionization chambers and Gafchromic foils. Figure 2 shows the geometries of these measurements (a) water dose measurement using ionization chamber AP 2.0, (b) water dose measurement using Gafchromic foils, and (c) air dose measurement using ionization chamber PTW-23342.
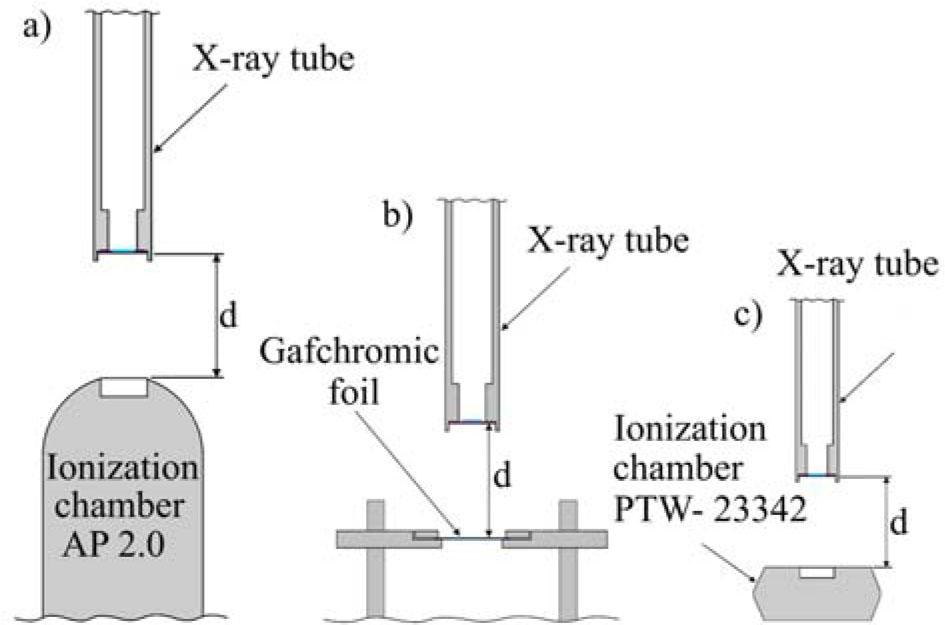
Geometrical setups for dose measurements: (a) ionization chamber AP 2.0, (b) Gafchromic film, and (c) ionization chamber PTW-23342.
The size of samples of radiochromic films, cut from the manufacturing sheet, was 30 mm × 30 mm. The manufacturer of these films is International Speciality Products, Wayne, NJ (ISP). To test the dosimetry techniques, two types of Gafchromic films, MD-55-V2 (Fig. 3a) and EBT (Fig. 3b) were irradiated with X-rays generated using an X-ray tube. As a result of irradiation, the films become darker, and the darkness of radiochromic films (Fig. 4) is proportional to the absorbed dose. The result of irradiation of such a foil is permanently placed on it (the foil changes color), making it a single-use foil. For each measurement point, a single Gafchromic film was used. Although the total film size was 30 mm × 30 mm, the analyzed region for dose determination was limited to an area of 19 mm2. In this region, 440 data points were recorded to generate a dose profile, with the standard deviation of the optical density measurements being 0.009, ensuring precise and consistent dose assessment.
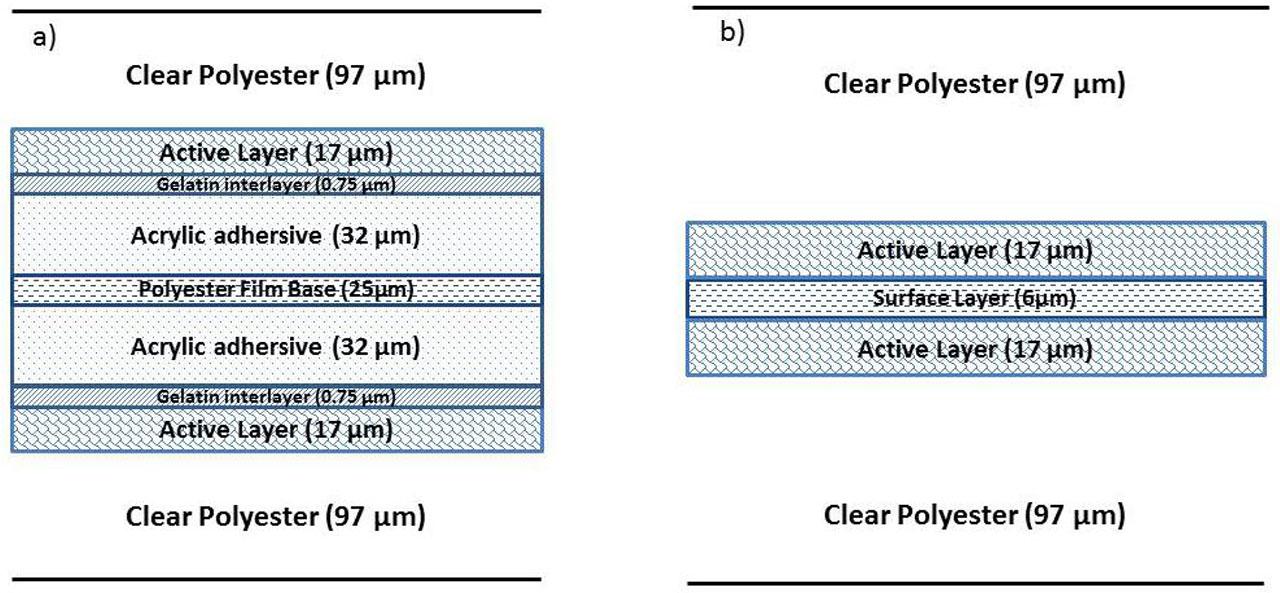
Configuration of (a) MD-V2-55 and (b) EBT dosimetry films (adapted from ISP Brochures).
EBT film after irradiation, showing the effects of absorbed dose.
The advantages of using radiochromic films include:
- –
tissue equivalence (Zeff ~ Zeff tissue),
- –
high spatial resolution,
- –
energy independence,
- –
dose rate independence,
- –
insensitivity to visible light,
- –
waterproof,
- –
no additional (chemical, physical) processing is required.
Measurement uncertainties in dose determination using radiochromic film involve several stages of the process. The total uncertainty of the dose measurement consists of the following components: uncertainty related to film exposure, i.e., X-ray beam uniformity, uexp = 1%, uncertainty related to optical readout, i.e., uncertainty from scanner calibration, usc = 0.5% and uncertainty related to the conversion of optical density to dose, i.e., uncertainty in fitting the calibration curve to experimental data, ucal = 1%. The combined standard uncertainty is the square root of the sum of the squared uncertainty components:
While the expanded uncertainty U, which covers a 95% confidence level, has been obtained by multiplying the combined standard uncertainty by the expansion factor k = 2:
The combined standard uncertainty uc is 1.5% and the expanded uncertainty U at a 95% confidence level is 3.0%.
Dose measurements in water, depending on the detector distance, were conducted using the AP 2.0 ionization chamber and Gafchromic foils. The results of the measurements using the ionization chamber are presented in Fig. 5.
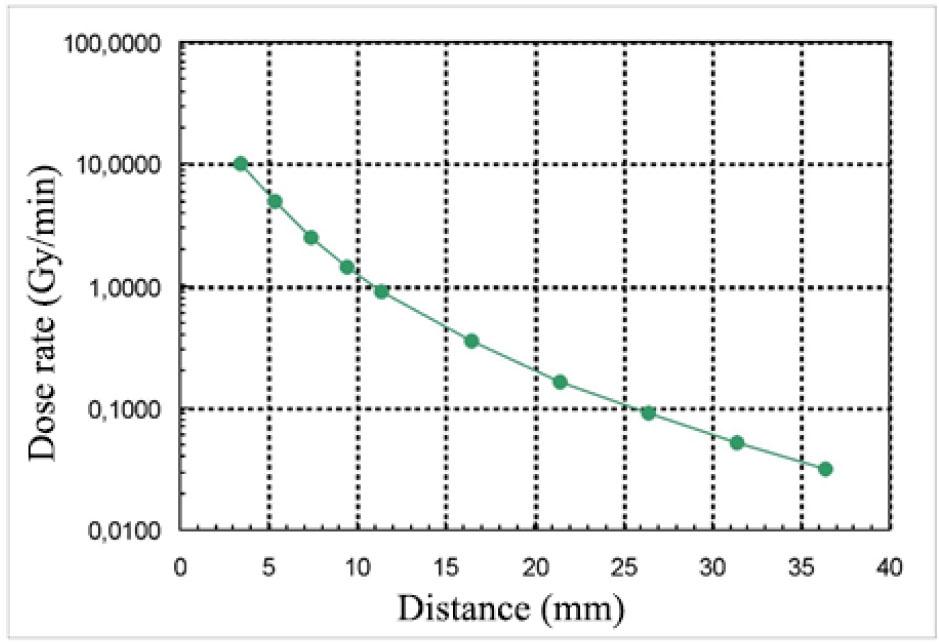
Dose rate measurement results using an ionization chamber as a function of the distance between the X-ray source and the detector.
Because of the large range of dose variability, two types of Gafchromic foils were used namely MD-55-V2 and EBT. Before dose measurement, the Gafchromic foils were calibrated at the Medical Physics Department of the Maria Skłodowska-Curie National Research Institute of Oncology in Warsaw (Fig. 6). The calibration was performed using a mammography X-ray tube operated with a voltage of 35 kV and an anode current of 20 mA. The distance between the Mo-X-Ray tube and Gafchromic films was set at 35 cm. The radiation from the lamp is collimated into a beam, which, at a distance of 100 cm from the lamp, has a diameter of 18 cm (flux accuracy ≤1%).
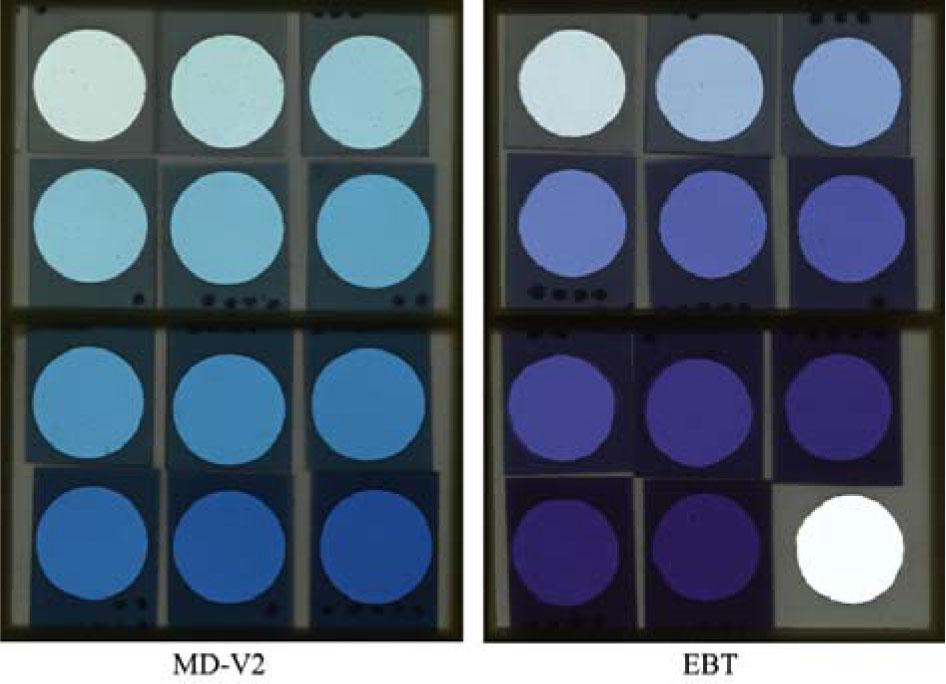
Calibration Gachromic foils, MD-55-V2 (left), EBT (right).
The films were scanned in red-blue-green (RGB) format using the Agfa Arcus 1200 scanner. To account for post-exposure density changes, the scanning procedure was initiated 24 h after film irradiation. The X-ray image obtained from the scanning procedure is analyzed using the SkanFilm application. This program sets the optical density for each pixel, and then the dose value is calculated.
The readout system is equipped with two patterns, the optical density pattern for densitometric calibration and the dose pattern for dosimetric calibration. The red and green readout channels were set for MD-55-V2 and EBT, respectively. The choice of the readout color channel was determined using previous measurements. Figure 7 shows the color sensitometric response of MD-V2-55 and EBT films. It can be observed that to maximize the response, the red color readout channel should be used.
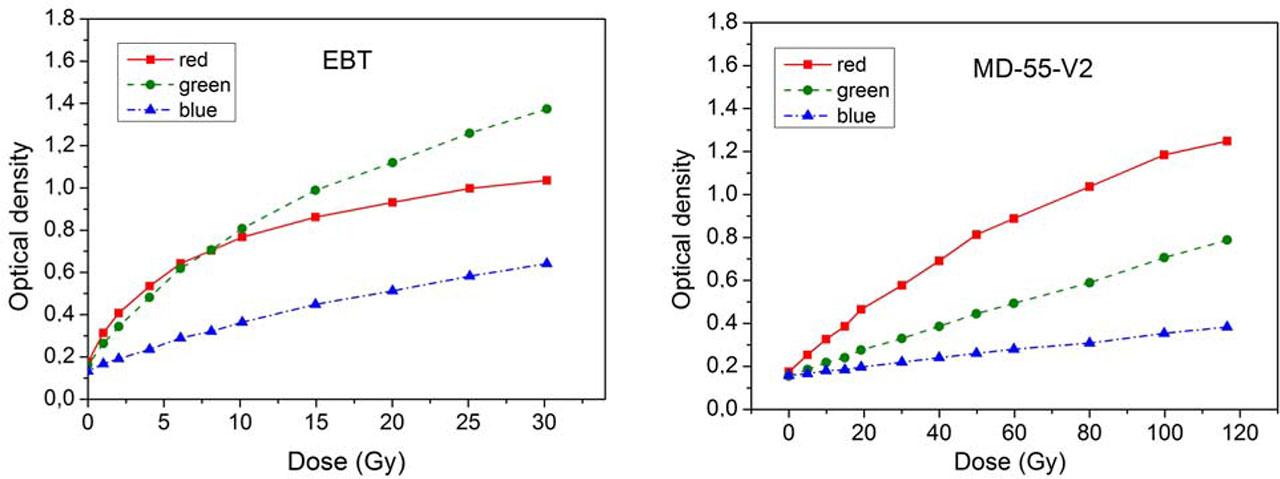
Response of MD-V2-55 and EBT radiochromic dosimetry films to radiation exposure.
Additionally, the EBT film was pre-exposed to assess the change in optical density over different days after reading the film (Fig. 8) for different dose rate values. As observed, the first day is crucial in the film reading, with a subsequent increase in optical density.
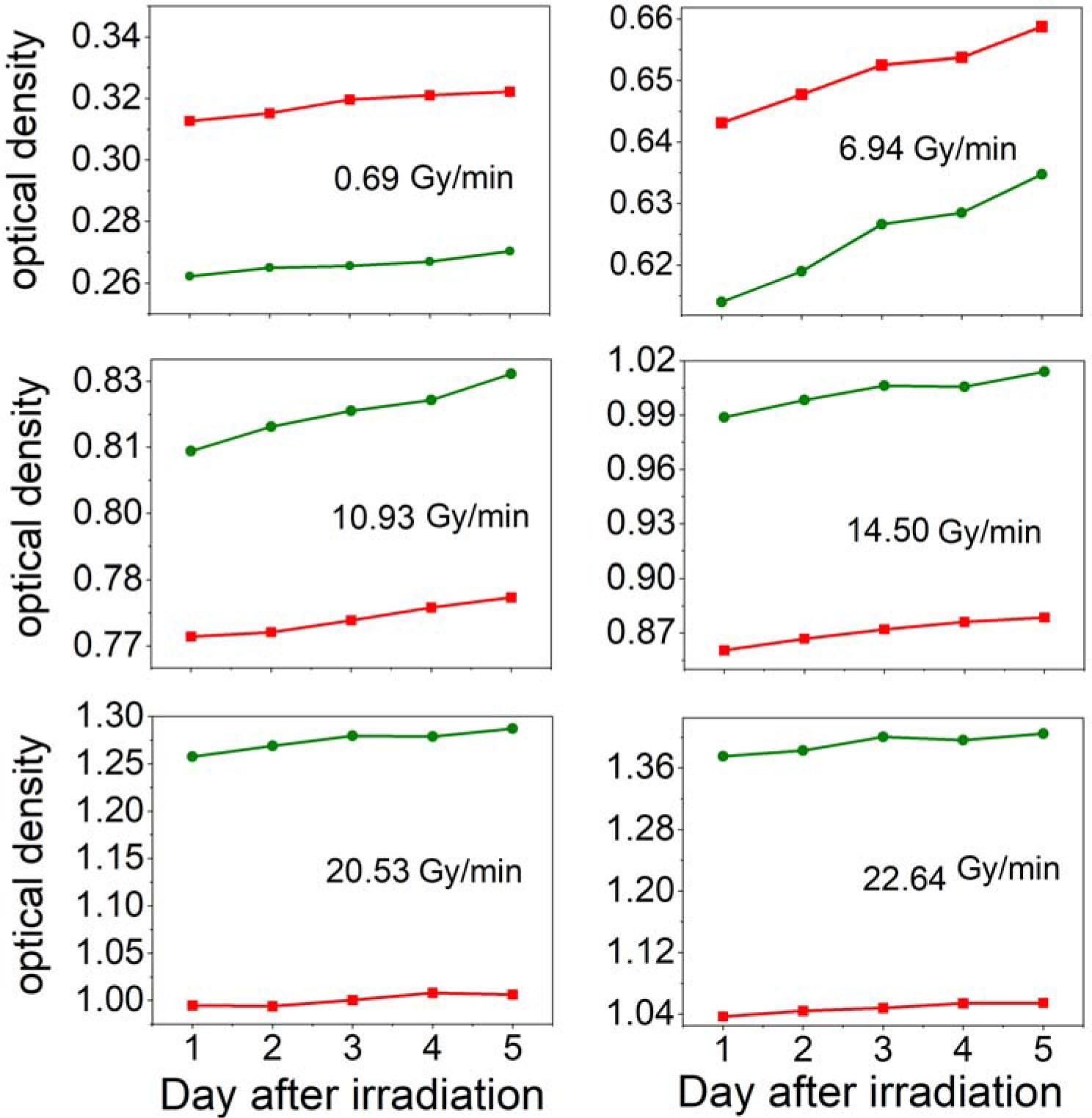
Dependence of optical density on the reading day following exposure, indicated by red and green colors.
Gafchromic foils irradiated with an X-ray lamp were scanned using an Arcus 1200 scanner to determine the dose depending on the distance. Due to the properties of the foil, the MD-V2-55 type foil was used for shorter distances and the EBT type foil for larger distances. The results of dose rate measurements in water are shown in Fig. 9.
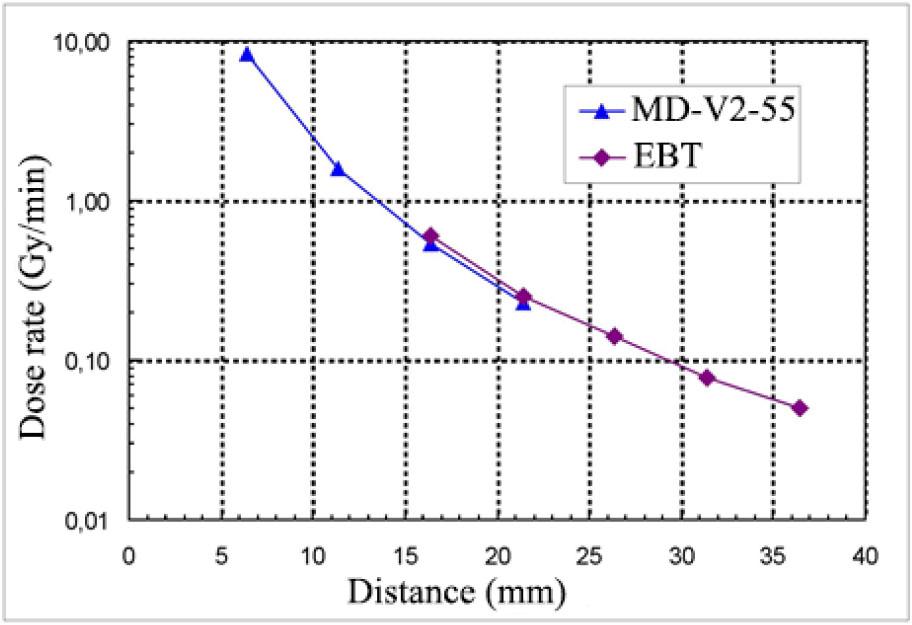
Dose rate measurement in water using Gafchromic foils as a function of the distance between the X-ray source and the foils.
Figure 10 presents the comparison of the measurement results and the results of Monte-Carlo calculations. The calculations were performed for a cylindrical-conical anode. The underestimated dose values measured with the AP 2.0 ionization chamber, compared to Gafchromic foil measurements and calculations, are likely due to the decalibration of the ionization chamber, potentially caused by a reduction in active volume resulting from decreased sensitivity due to the aging of materials.
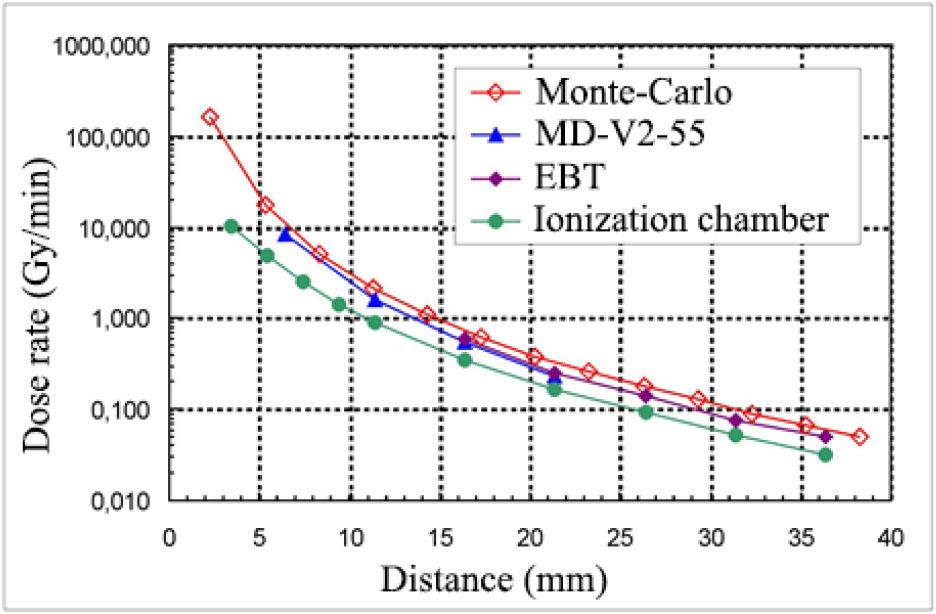
Comparison of the measurement results with Monte-Carlo calculations.
The dose rate distribution in air was also measured. The dose detectors used were the PTW-23342 ionization chamber and Gafchromic EBT foil. Figure 11 presents the measurement results.
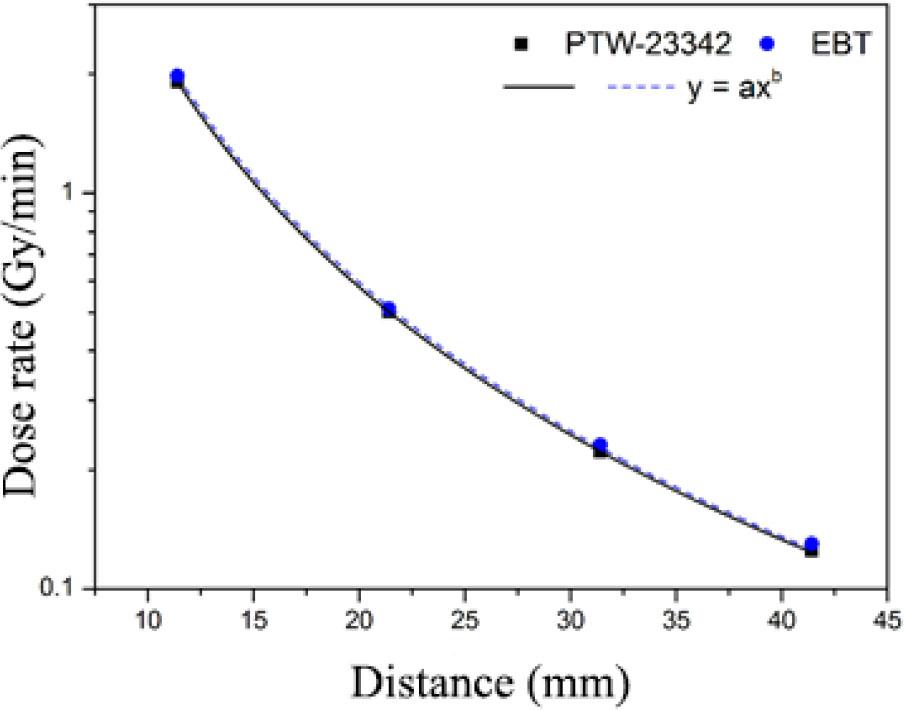
The results of measuring the dose in the air as a function of distance between the X-ray source and detector.
The focus of the discussed works revolves around the application of radiochromic films in dosimetry, spanning scenarios such as dose measurements in photon fields with high gradients and studies in IORT. These publications offer insights into calibration methods, result interpretation, and the utilization of different detectors, prominently featuring ionization chambers.
A key consideration in these works is the assessment of post-exposure changes in the optical density of the films and the subsequent correction of these changes during results analysis. Comparative evaluations between distinct film types, like MD-55-V2 and EBT, aim to gauge their efficacy under varying conditions.
A collective objective across these studies is the enhancement of the accuracy in radiation dose measurements, a critical element for ensuring patient safety in radiotherapy.
In one study, the investigation focused on dose rate distribution concerning the distance between the X-ray radiation source and the detector. Dose rate measurements in the air were conducted for Gafchromic MD-55-V2 and Gafchromic EBT and are compared with ionization chamber AP values and Monte-Carlo simulations. Water dose measurements were performed for EBT films, compared with measurements from ionization chamber PTW-23342. Results indicated that both MD-55-V2 and EBT films yielded responses consistent with ionization chamber values.
Additionally, optical density-dose relationships were explored for Gafchromic foils at the Maria Skłodowska-Curie National Research Institute of Oncology in Warsaw, affirming the red channel as the optimal readout. For EBT films, a study demonstrated the dependence of optical density on the day of reading after exposure, highlighting the significance of reading the film within the first days. Dosimetric films were underscored as valuable tools for spatially assessing cumulative dose in various applications, with a substantial impact on medical physics, treatment plan optimization, and patient safety in radiotherapy. The versatility of dosimetric films extends to diverse scientific and industrial applications, marking them as pivotal components in radiation detection and safety assessments across different fields.