
FIGURE 1.
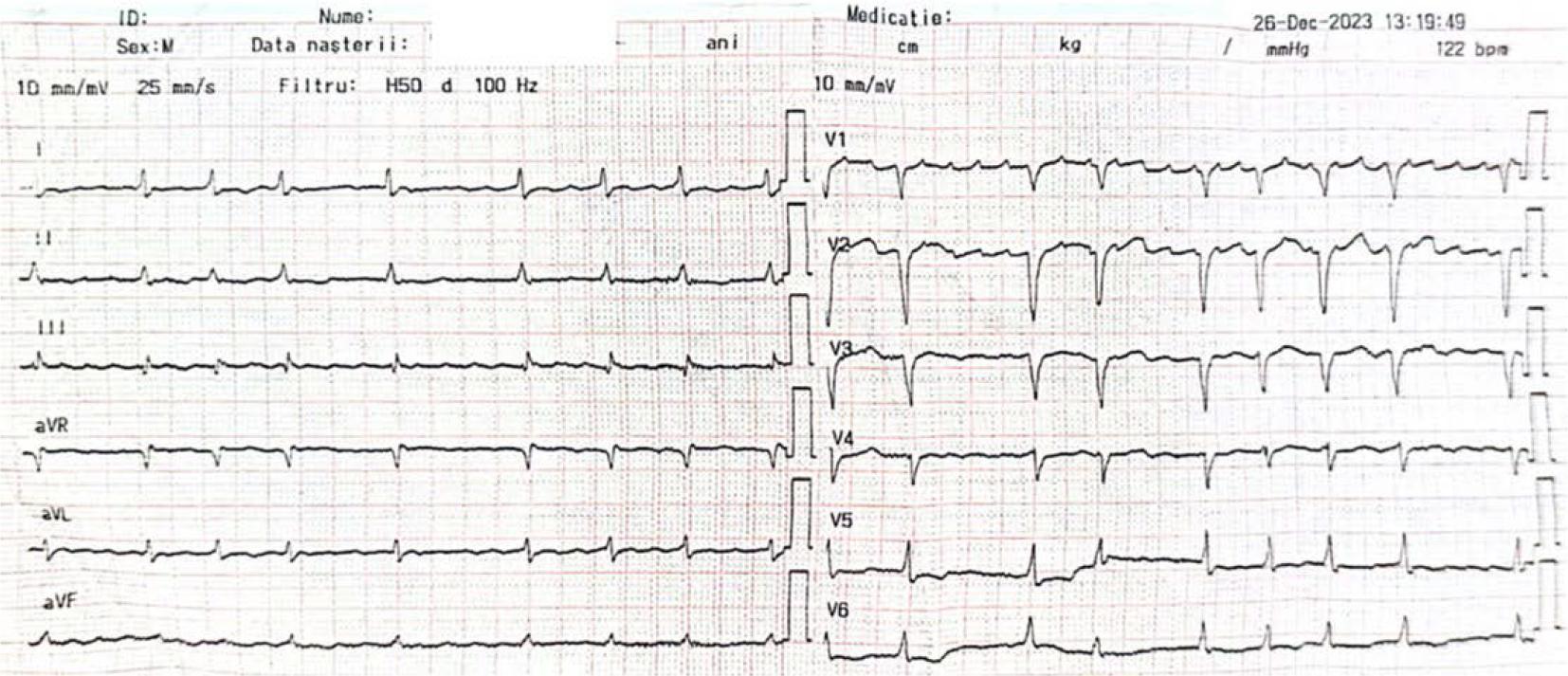
FIGURE 2.
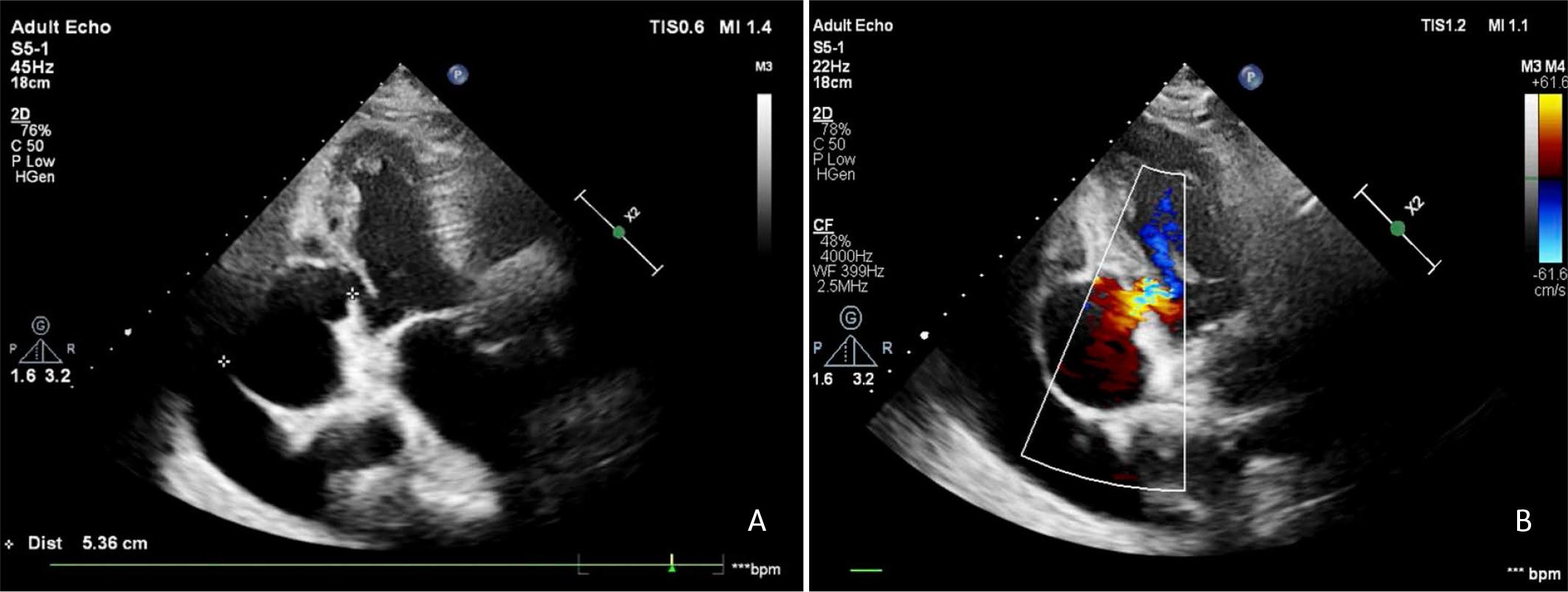
FIGURE 3.
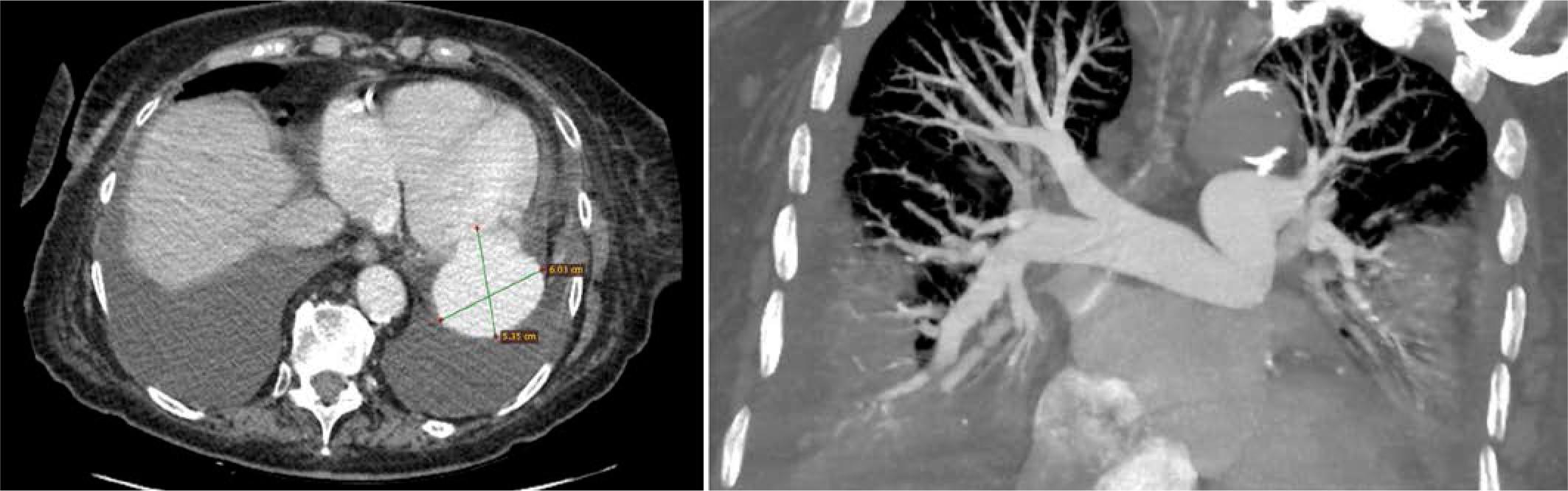
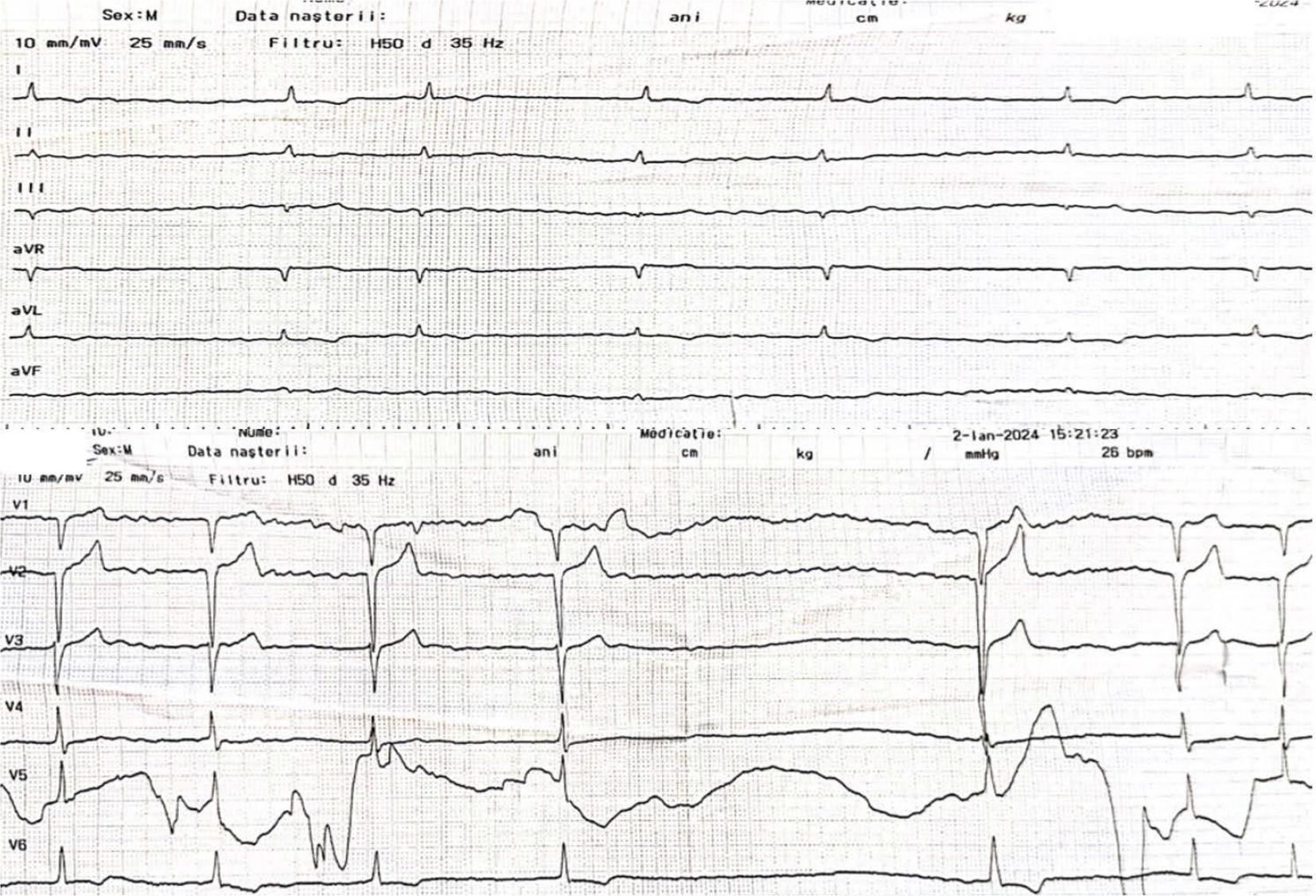
FIGURE 4.
Laboratory findings at admission to the Cardiology Department
| Laboratory finding | Value | Reference range |
|---|---|---|
| D-dimers | 3,240 ng/ml | < 500 ng/ml |
| Troponine | 49 | < 50 |
| NT-proBNP | 35,000 pg/ml | < 300 pg/ml |
| Glucose | 115 mg/dl | 70–110 mg/dl |
| Creatinine | 1.70 mg/dl Clearance 28.77 ml/min | 0.5–1.2 mg/dl |
| Urea | 29 mg/dl | 20–50 mg/dl |
| Potassium | 3.43 mmol/L | 3.5–5.1 mmol/L |
| C-reactive protein | 4.8 mg/dl | 0–1 mg/dl |
| Total protein | 5.9 g/dl | 6–8 g/dl |
| Albumin | 2.9 g/dl | 3.5–5.2 g/dl |
| Ferritin | 390 ng/ml | 10–300 ng/ml |
| Serum iron | 47 μg/dl | 50–175 μg/dl |
| Hemoglobin | 10 g/dl | 12–17 g/dl |
| Hematocrit | 31.2 g/dl | 36–52 g/dl |
| Lymphocytes | 19.2% | 20–40% |
| Erythrocyte sedimentation rate | 30 mm/h | 6–12 mm/h |
| International normalized ratio | 1.06 | 0.8–1.2 |
Paraclinical investigations on day 23 of hospitalization
| Laboratory finding | Value | Reference range |
|---|---|---|
| White blood cells | 16.67 × 109/L | 4–40 |
| Neutrophils | 82.9% | 50–75 |
| Lymphocytes | 10% | 20–40 |
| Hemoglobin | 11.8 g/dl | 12–17 |
| Ferritin | 530 ng/ml | 10–300 |
| C-reactive protein | 5.2 mg/dl | 0–1 |
| Creatinine | 1.81 mg/dl, eGFR 26.49 ml/min/1.73 m2 | 0.5–1.2 |
| Albumin | 3.3 g/dl | 3.5–5.2 |
| Glucose | 240 mg/dl | 70–110 |
| Total bilirubin | 0.57 mg/dl | <1 |
| Direct bilirubin | 0.02 mg/dl | <0.4 |
| Amylase | 26 U/L | 0–100 |
| Abdominal ultrasound | Dilated gallbladder with markedly thickened, echogenic walls and multiple gallstones. | |