
Left ventricular pseudoaneurysm (LVP) is a mechanical complication of myocardial infarction that, although rare in clinical practice, is associated with very high mortality. From a pathophysiological perspective, a pseudoaneurysm results from rupture of the left ventricular free wall contained by adherent pericardium or scar tissue.1–3 In practice, the wall of a pseudoaneurysm is formed by hematoma, epicardium, and pericardium, in contrast to a left ventricular aneurysm, which involves the entire myocardial wall with scarred endocardium.4,5
Regarding the timing of this complication, studies show considerable variability in the interval between myocardial infarction and pseudoaneurysm formation, ranging from 3–7 days after the acute coronary event to several years later. However, on average, these patients are diagnosed approximately 60 days after the ischemic event.5
The clinical presentation of these patients can be highly variable and often non-specific, which makes early diagnosis challenging. Patients may present with signs of cardiac decompensation, arrhythmias, or chest pain. Early diagnosis is particularly important because pseudoaneurysms tend to enlarge rapidly, significantly increasing the risk of rupture.4,5 Given the very high mortality associated with pseudoaneurysm rupture, prompt diagnosis is essential. The diagnosis can be confirmed by echocardiography or other imaging modalities such as computed tomography or cardiac magnetic resonance. Once the diagnosis is established, treatment should be determined primarily based on the size of the pseudoaneurysm, the risk of rupture, and whether the patient is symptomatic or asymptomatic.4,5 Surgical repair remains the standard treatment. However, in recent years, percutaneous closure techniques have also been developed. According to available data, these techniques are not yet available in our country.
In this article, we present the case of a giant posterior wall pseudoaneurysm associated with clinical signs of cardiac decompensation in a patient with multiple comorbidities and a precarious social situation, which ultimately led to delayed diagnostic confirmation. The complexity of the case, the very high surgical risk associated with pseudoaneurysm repair, and the lack of percutaneous closure options ultimately resulted in the patient’s death. Through this case report, we also review the relevant literature, highlighting the importance of early diagnosis and the crucial role of appropriate treatment in preventing the most feared outcome of this complication, patient death.
The patient was admitted to the Neurology Department of the Clinical Rehabilitation Hospital in Cluj-Napoca in November 2023 for neurological recovery following an ischemic stroke in August 2023. The patient was known with flaccid tetraparesis, axonal and demyelinating polyradiculoneuritis treated with immunoglobulins (August 2023), type 2 diabetes mellitus, persistent atrial fibrillation, infero-postero-lateral ST-elevation myocardial infarction treated with percutaneous transluminal coronary angioplasty with two drug-eluting stents in the left anterior descending artery and two in the right coronary artery (August 2023), and chronic kidney disease stage IV (KDIGO). After the acute ischemic events in August, the patient had been institutionalized in a palliative care center without cardiological or neurological follow-up during the following 4 months.
On the 16th day of the current hospitalization, the patient developed sudden-onset dyspnea associated with orthopnea, palpitations with a rapid irregular rhythm, marked fatigue, anxiety, and significant deterioration of the general condition. An urgent cardiology consultation was therefore requested.
On clinical examination, the patient was immobilized, markedly tachypneic, and orthopneic. Cardiac auscultation revealed arrhythmic heart sounds, with a heart rate of approximately 100 bpm in atrial fibrillation. Blood pressure was 130/80 mmHg, with no audible cardiovascular murmurs. Oxygen saturation was 79% on room air. Breath sounds were absent in the lower two-thirds of both lung bases. Emergency laboratory tests revealed markedly elevated D-dimer levels (3,240 ng/ml), negative troponin, and significantly elevated NT-proBNP (35,000 pg/ml). Table 1 presents the laboratory results obtained at admission to the Cardiology Department. The electrocardiogram (ECG) revealed atrial fibrillation with a heart rate of approximately 100 bpm, slow R-wave progression in leads V1–V4, and ST-segment depression of approximately 0.5 mm in V5–V6. No S1Q3T3 pattern was observed. (Figure 1). The ECG findings were similar to those on previous recordings.
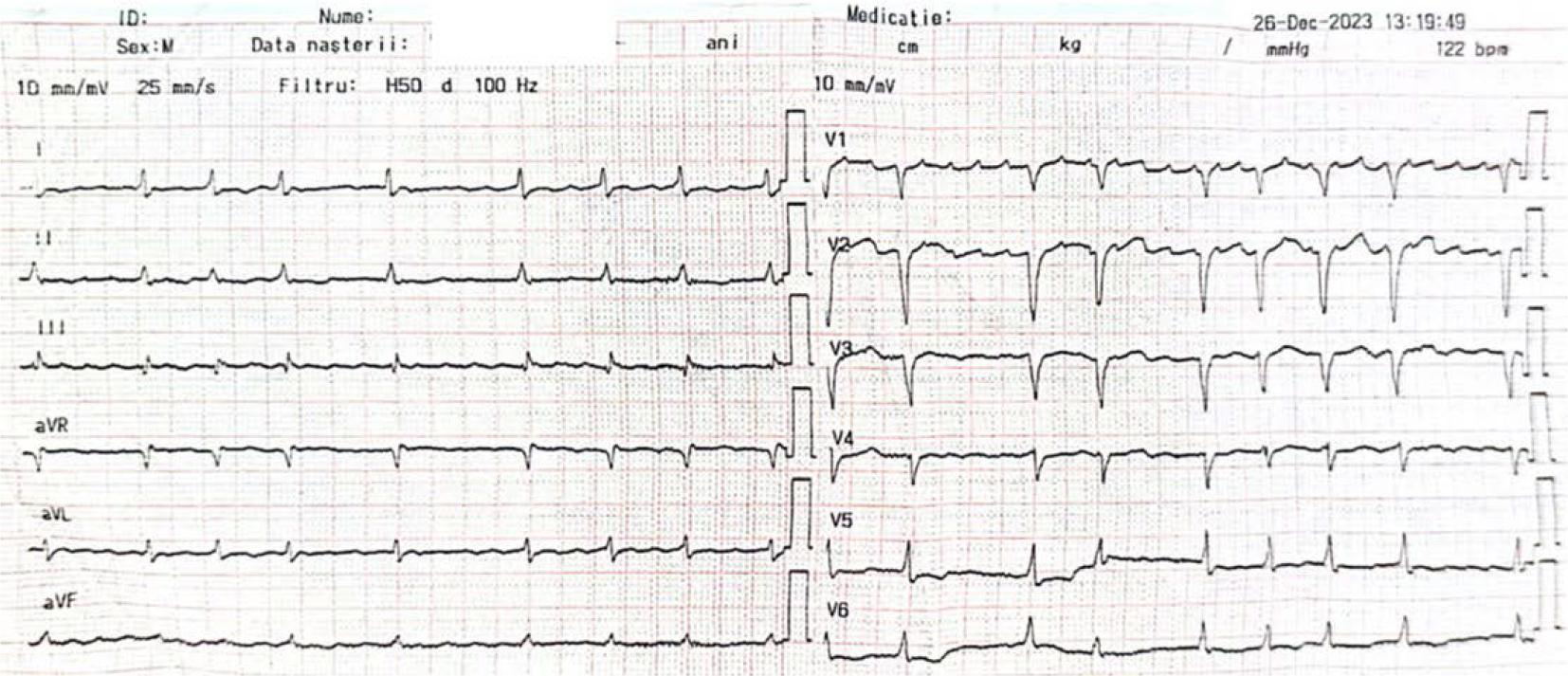
ECG at the moment of the crisis.
Laboratory findings at admission to the Cardiology Department
| Laboratory finding | Value | Reference range |
|---|---|---|
| D-dimers | 3,240 ng/ml | < 500 ng/ml |
| Troponine | 49 | < 50 |
| NT-proBNP | 35,000 pg/ml | < 300 pg/ml |
| Glucose | 115 mg/dl | 70–110 mg/dl |
| Creatinine | 1.70 mg/dl Clearance 28.77 ml/min | 0.5–1.2 mg/dl |
| Urea | 29 mg/dl | 20–50 mg/dl |
| Potassium | 3.43 mmol/L | 3.5–5.1 mmol/L |
| C-reactive protein | 4.8 mg/dl | 0–1 mg/dl |
| Total protein | 5.9 g/dl | 6–8 g/dl |
| Albumin | 2.9 g/dl | 3.5–5.2 g/dl |
| Ferritin | 390 ng/ml | 10–300 ng/ml |
| Serum iron | 47 μg/dl | 50–175 μg/dl |
| Hemoglobin | 10 g/dl | 12–17 g/dl |
| Hematocrit | 31.2 g/dl | 36–52 g/dl |
| Lymphocytes | 19.2% | 20–40% |
| Erythrocyte sedimentation rate | 30 mm/h | 6–12 mm/h |
| International normalized ratio | 1.06 | 0.8–1.2 |
Following the clinical examination and ECG, emergency transthoracic echocardiography was performed. The examination showed a non-dilated left ventricle with mildly impaired systolic function (ejection fraction approximately 45%) and posterior wall akinesia. A pseudoaneurysm measuring 5.36 cm was identified at this level. The right heart chambers were slightly dilated, with moderate tricuspid regurgitation, pulmonary hypertension, and bilateral pleural effusion (8.5 cm on the right and 6 cm on the left) (Figure 2).
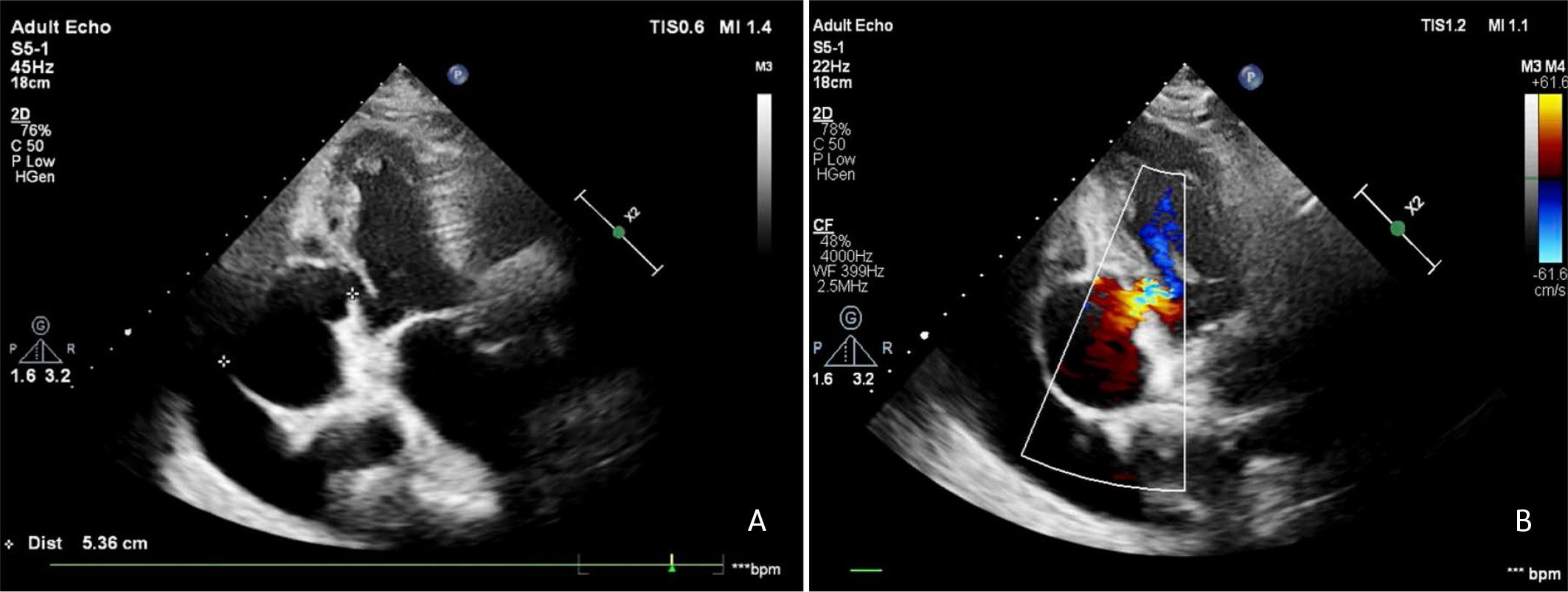
A. Apical three-chamber view showing a left ventricular posterior wall pseudoaneurysm measuring 5.36 cm, with associated left pleural effusion. B. Color Doppler examination demonstrating communication between the left ventricular cavity and the pseudoaneurysm.
Notably, this was the first cardiac ultrasound performed after the myocardial infarction in August, approximately 4 months after the acute event. An earlier echocardiographic evaluation, ideally within the first month after myocardial infarction, would likely have detected a smaller pseudoaneurysm before the development of heart failure, with important clinical implications and potentially lower mortality.
Because pulmonary thromboembolism could not be excluded given the sudden onset of dyspnea, low oxygen saturation, markedly elevated D-dimer levels, dilated right heart chambers, pulmonary hypertension, and the patient’s immobilization without anticoagulant therapy, an urgent thoracic computed tomography angiography was performed. Of note, anticoagulant treatment (apixaban 5 mg twice daily) had been discontinued after admission to the Neurology Department by the neurologist due to severe renal dysfunction, with a creatinine clearance of 10 ml/min.
Computed tomography angiography excluded pulmonary thromboembolism and confirmed the presence of a posterior left ventricular pseudoaneurysm with a maximum diameter of 6.03 cm. It also revealed a thrombus in the left atrial appendage and bilateral pleural effusions measuring 8.3 cm on the right and 4.4 cm on the left, with passive atelectasis of the adjacent lung parenchyma (Figure 3).
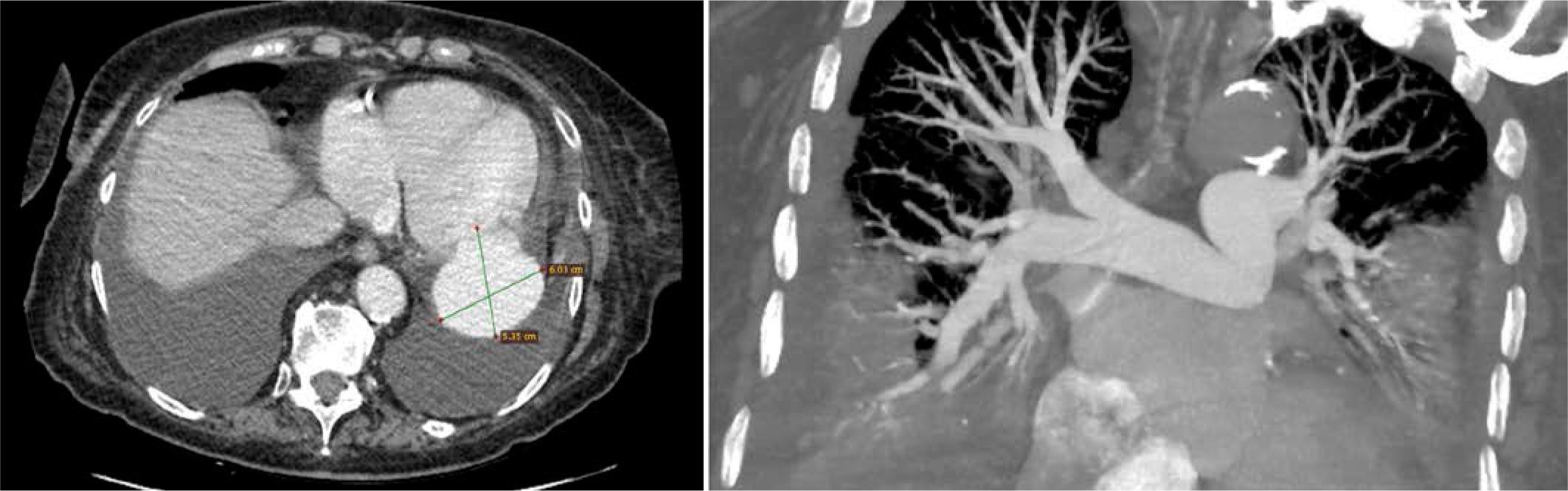
Thoracic CT angiography showing a posterior wall left ventricular pseudoaneurysm, bilateral pleural effusion, and thrombus in the left atrial appendage. No signs of pulmonary thromboembolism are present.
The patient’s symptoms were therefore interpreted as secondary to cardiac decompensation. Treatment for heart failure and associated comorbidities was initiated, including intravenous furosemide (20 mg/2 ml), resulting in diuresis of up to 3,500 ml/24 h; spironolactone 25 mg/day; atorvastatin 20 mg/day; clopidogrel 75 mg/day; digoxin 0.25 mg (¼ tablet/day); perindopril 2.5 mg/day depending on blood pressure values; reduction of bisoprolol from 10 mg/day to 5 mg/day; an SGLT2 inhibitor (dapagliflozin 10 mg/day); potassium and albumin supplementation; and proton pump inhibitors for gastric protection.
Considering the high thromboembolic risk (patient with atrial fibrillation, a thrombus in the left atrial appendage detected on angio-CT, and a pseudoaneurysm larger than 3 cm with increased risk of thrombus formation), anticoagulant therapy was reintroduced into the treatment plan. Enoxaparin 0.8 ml was administered subcutaneously once daily, at a therapeutic dose adjusted to the patient’s creatinine clearance at that time (28.77 ml/min). The patient’s weight was 80 kg, corresponding to a therapeutic dose of approximately 1 mg/kg of enoxaparin.
Right-sided thoracentesis was also performed, with evacuation of 1,200 ml of serocitrin pleural fluid, without periprocedural complications. Pleural fluid analysis confirmed the presence of a transudate.
Clinically, the patient showed significant improvement, with remission of the congestive syndrome and improvement of dyspnea. However, due to the presence of the giant pseudoaneurysm with a high risk of rupture, repeated consultations with cardiovascular surgery were requested. Eventually, a heart team meeting was convened, including a cardiologist, cardiac surgeon, anesthesiologist, and neurologist. The team concluded that the patient’s perioperative risk was extremely high, with a predicted mortality of 27.29% according to the EuroSCORE II. Surgery could be performed if the patient’s family accepted the associated risks; however, the family ultimately declined surgical intervention. We note that percutaneous closure of ventricular pseudoaneurysms is not available in our center and, to our knowledge, this procedure is not currently performed in our country.
On day 23 of hospitalization, the patient complained of abdominal pain in the right hypochondrium and epigastrium, associated with nausea and bilious vomiting. There were no signs of an acute abdomen and no jaundice. At the same time, monitoring revealed bradycardia of approximately 30 bpm (Figure 4). Treatment with bisoprolol and digoxin was discontinued, as the bradycardia was interpreted as a vagal reaction induced by vomiting. An emergency abdominal–pelvic ultrasound was requested. The ultrasound confirmed the presence of symptomatic multiple gallstones. Laboratory tests showed a rapidly increasing inflammatory syndrome, mild hypoalbuminemia and anemia, and hyperglycemia, while liver enzymes and amylase remained within normal limits. Table 2 presents the results of the paraclinical investigations.
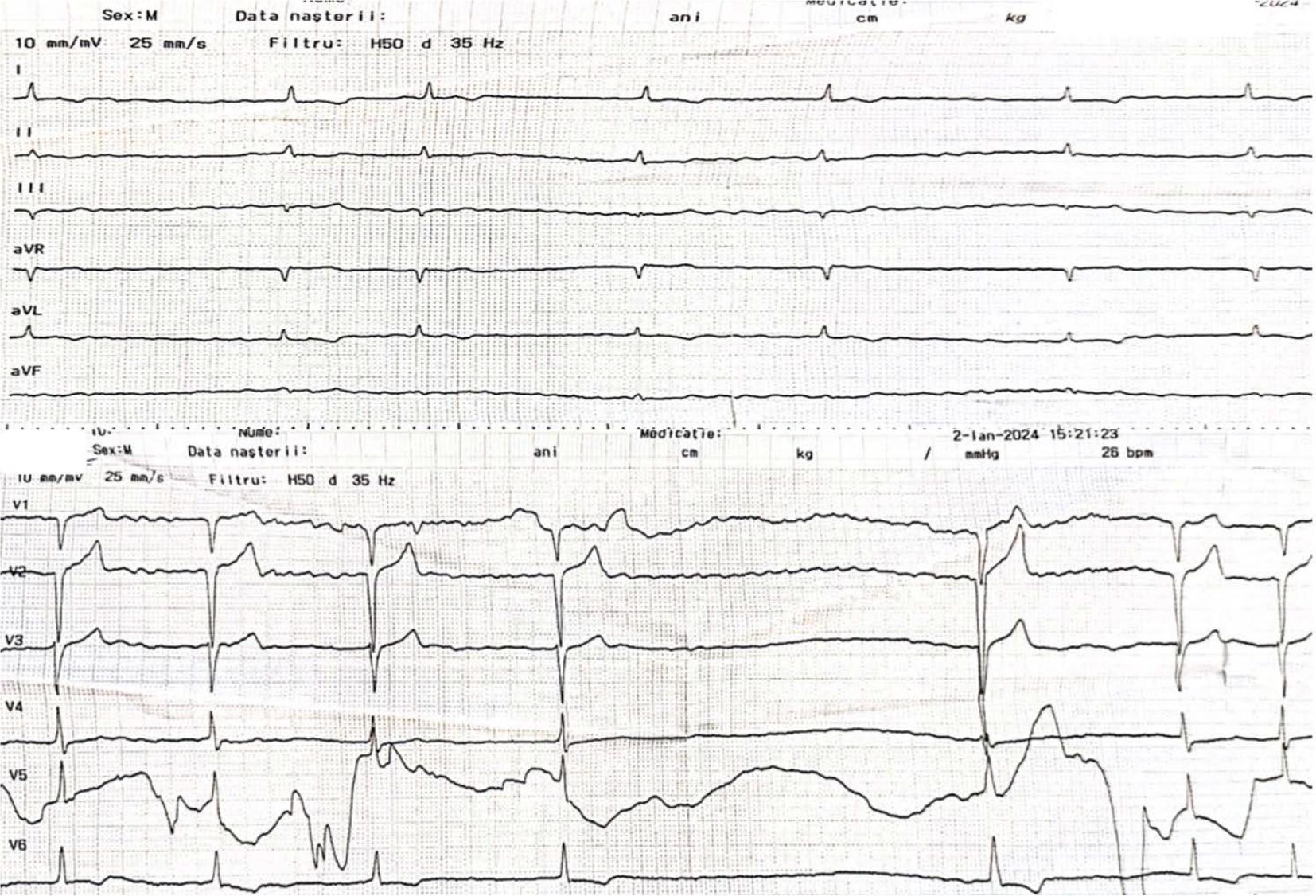
ECG showing significant bradycardia, interpreted as a vagal reaction secondary to the vomiting episode.
Paraclinical investigations on day 23 of hospitalization
| Laboratory finding | Value | Reference range |
|---|---|---|
| White blood cells | 16.67 × 109/L | 4–40 |
| Neutrophils | 82.9% | 50–75 |
| Lymphocytes | 10% | 20–40 |
| Hemoglobin | 11.8 g/dl | 12–17 |
| Ferritin | 530 ng/ml | 10–300 |
| C-reactive protein | 5.2 mg/dl | 0–1 |
| Creatinine | 1.81 mg/dl, eGFR 26.49 ml/min/1.73 m2 | 0.5–1.2 |
| Albumin | 3.3 g/dl | 3.5–5.2 |
| Glucose | 240 mg/dl | 70–110 |
| Total bilirubin | 0.57 mg/dl | <1 |
| Direct bilirubin | 0.02 mg/dl | <0.4 |
| Amylase | 26 U/L | 0–100 |
| Abdominal ultrasound | Dilated gallbladder with markedly thickened, echogenic walls and multiple gallstones. | |
A gastroenterology consultation was requested. Antispasmodic and antiemetic treatment, parenteral hydration, and abdominal–pelvic CT were recommended, with gastroenterological reassessment if necessary. Despite the prescribed treatment, the patient’s gastroenterological condition did not improve, with persistent abdominal pain, bilious vomiting, fever up to 38.3°C, and increased inflammatory markers (CRP 11.3 mg/dl, leukocytes 21,000/μl), while procalcitonin remained negative and liver tests within normal limits. Acute lithiasic cholecystitis was therefore suspected. The patient was also evaluated by an infectious disease specialist, who recommended initiation of antibiotic therapy with piperacillin/tazobactam (4 g/0.5 g) and a surgical consultation to evaluate the possibility of cholecystectomy.
The patient was transferred to the surgery department for evaluation and assessment of the indication for surgical treatment. However, due to multiple comorbidities associated with very high surgical risk, the absence of signs of acute abdomen or jaundice, and a slight decrease in leukocyte count under antibiotic therapy, conservative management was recommended, and the patient was subsequently referred back to our department.
From a gastroenterological perspective, under antibiotic, antispasmodic, and antiemetic treatment for acute lithiasic cholecystitis, the patient’s evolution was favorable, both clinically and biologically, with remission of the inflammatory syndrome. However, from a cardiological standpoint, on the 29th day of hospitalization, at 16:40, the patient developed cardiorespiratory arrest due to electromechanical dissociation. Resuscitation maneuvers were initiated, orotracheal intubation was performed, and ventilation with a bag-valve mask was started. After approximately 10 minutes, mechanical and electrical cardiac activity resumed. The monitor showed atrial fibrillation with a ventricular rate of 140 bpm and blood pressure of 70/30 mmHg. Vasopressor therapy with noradrenaline was initiated and titrated to maximum doses.
Approximately 2 hours later, the patient experienced another cardiorespiratory arrest due to ventricular fibrillation, for which external electrical defibrillation was performed, resulting in the resumption of cardiac activity. Emergency echocardiography revealed signs of cardiac tamponade secondary to rupture of the pseudoaneurysm. Five minutes later, the patient developed a new cardiorespiratory arrest due to asystole. Despite resuscitation maneuvers, no return of spontaneous circulation was achieved, and the patient was declared dead.
Left ventricular pseudoaneurysm (LVP) is a mechanical complication that most commonly occurs after acute myocardial infarction (55%) or cardiac surgery (33%), and much more rarely in a traumatic context (7%).4 It is characterized by rupture of the free wall of the left ventricle, most often involving the posterior wall, particularly following an infero-postero-lateral transmural infarction. Unlike a true ventricular aneurysm, the rupture is contained by the pericardium, pericardial adhesions, or thrombus formation.4
The exact timing of pseudoaneurysm formation after an acute event is not fully known and may vary from a few days to several years, although it is most often diagnosed approximately 2–3 months after myocardial infarction.5 The diagnosis may be incidental during routine evaluation, with more than 10% of patients remaining asymptomatic. However, patients may also present with symptoms such as dyspnea, angina, palpitations, cardiac decompensation, or even neurological manifestations.5,6 In addition, large pseudoaneurysms, usually greater than 3 cm, carry a high risk of thrombus formation, which may clinically manifest through embolic events.7
Physical examination findings may vary. Some patients may present no significant abnormalities, while others may have a holosystolic murmur, pericardial friction rub, or signs of cardiac decompensation or tamponade.8,9 ECG findings are often non-specific and typically reflect prior myocardial infarction, rhythm disturbances, or electrical alternans in cases of tamponade. Up to 20% of patients may present ST-segment elevation. Therefore, diagnosis based solely on clinical examination and ECG is difficult, and additional imaging investigations such as echocardiography, CT, or cardiac magnetic resonance are required.4,9
In our patient, the clinical presentation was that of cardiac decompensation, and the diagnosis was confirmed by echocardiography and cardiac CT. Cardiac auscultation did not reveal a holosystolic murmur or a pericardial friction rub. Thus, based only on clinical examination and ECG, which showed non-specific changes, it would have been impossible to identify the pseudoaneurysm as the cause of cardiac decompensation. No other causes of cardiac decompensation were identified at the time of diagnosis, making the large pseudoaneurysm the most plausible explanation.
The exact timing of pseudoaneurysm formation could not be determined with certainty. However, the diagnosis was confirmed approximately 4 months after the myocardial infarction. Its location at the posterior wall is typical given the infero-postero-lateral infarction previously experienced by the patient. Posterior LVPs are the most frequently encountered in clinical practice, being identified in approximately 82% of cases, compared with those located on the lateral wall (28%) or in the apical region (20%).3,5,10 Infero-postero-lateral infarctions may also be complicated by rupture of the posteromedial papillary muscle, leading to acute mitral regurgitation,5 an aspect that was not observed in our patient.
Accurate diagnosis of this complication is crucial. Although the natural history of LVPs is not fully understood, they are known to carry a poor prognosis due to the high risk of rupture (approximately 45%).5,11 The risk of rupture is influenced by the size of the pseudoaneurysm and appears to be inversely related to the time elapsed since myocardial infarction. It tends to be lower in asymptomatic, stable patients with small (<3 cm) or chronic pseudoaneurysms.5,11,12 In contrast, pseudoaneurysms occurring early after myocardial infarction, in symptomatic patients, or when large in size are associated with a very high risk of rupture.5,11,12
For this reason, the presence of a large, symptomatic pseudoaneurysm is generally considered an indication for prompt surgical repair, whereas conservative management is associated with high mortality. In our case, the patient presented with a pseudoaneurysm of impressive size but also with an extremely high perioperative risk due to multiple severe comorbidities, which made surgical intervention impossible. As mentioned, the EuroSCORE II value was 27.29%, indicating a very high predicted perioperative mortality. In addition, the patient’s family declined surgical intervention given the associated risks. These factors made the case particularly complex from both clinical and therapeutic perspectives, creating a difficult therapeutic dilemma. In the absence of surgical treatment, the prognosis was clearly unfavorable; however, surgical intervention itself carried an extremely high risk of perioperative death. Although surgery does not necessarily imply a fatal outcome, perioperative risk scores such as EuroSCORE II are important tools for estimating mortality risk after cardiac surgery and must be carefully considered in clinical decision-making.
In such a complex clinical scenario involving an inoperable patient, the remaining therapeutic option is percutaneous closure of the left ventricular pseudoaneurysm, which represents a feasible alternative to surgical treatment.3 Percutaneous closure of LVP was first described in 2004 by Clift et al.,13 who performed closure using an Amplatzer occluder in a patient who had previously undergone ventricular reconstruction and coronary artery bypass grafting. Later, in 2016, Okuyama et al.14 reported the first successful percutaneous closure using a transapical approach.
Since then, multiple cases have been described in the literature, using different closure techniques and various devices such as ventricular septal occluders and coils.5 The complications of this procedure may include bleeding, hematoma, infection, device embolization, incomplete closure of the pseudoaneurysm, rhythm disturbances, pericardial effusion, cardiac tamponade, or even death.3 However, given that this intervention is relatively new and the number of procedures remains low due to the rarity of LVP, a larger number of cases is needed to better assess the potential long-term outcomes and complications. Nevertheless, it remains a promising option in patients with a high perioperative risk.
Although the theoretical solution was straightforward, percutaneous closure of the LVP was not available in our center, nor in other centers in the country. Therefore, the only remaining approach was conservative management, focusing on the treatment of heart failure and the associated comorbidities.
An important consideration is whether earlier cardiological evaluation, for example 1 month after the myocardial infarction, might have altered the clinical course. In such a scenario, the pseudoaneurysm would likely have been diagnosed earlier, before the development of acute heart failure, which might have reduced the patient’s mortality risk. However, the relatively late diagnosis in a patient with a giant LVP, with a striking clinical presentation of acute heart failure and multiple other important associated comorbidities, ultimately led to the patient’s death in the absence of appropriate treatment for the pseudoaneurysm. This once again confirms the importance of diagnosing this possible mechanical complication as early as possible, as well as the importance of treating the pseudoaneurysm, because in the absence of a specific therapeutic intervention the end result is invariably pseudoaneurysm rupture and the patient’s death.
In conclusion, LVP, although a mechanical complication of myocardial infarction that is rarely encountered in clinical practice, is associated with an extremely high risk of mortality in the absence of closure treatment. Mortality is mainly related to its complications, such as heart failure, ventricular arrhythmias, and pseudoaneurysm rupture, which is most often fatal for the patient.