
Patent foramen ovale (PFO) is an interatrial communication that plays a crucial role during fetal development, serving as a bypass for blood entering the right atrium. It normally closes at birth due to increased left atrial pressure; however, this mechanism fails in a significant proportion of individuals. PFO is one of the most common congenital heart defects, reported in approximately 25% of the adult population. Although initially considered a benign finding, advances in imaging techniques and growing clinical experience have shown that PFO is associated with significant morbidity, particularly cryptogenic stroke and paradoxical embolism. This association has been confirmed by several randomized controlled trials, such as Randomized Evaluation of Recurrent Stroke Comparing PFO Closure to Established Current Standard of Care Treatment (RESPECT), Patent Foramen Ovale Closure or Anticoagulants versus Antiplatelet Therapy to Prevent Stroke Recurrence (CLOSE), and GORE Septal Occluder Device for PFO Closure in Stroke Patients (REDUCE), which demonstrated a reduced risk of recurrent stroke following percutaneous PFO closure.1
The cardiac septa form between days 27 and 37 of intrauterine life. The interatrial septum develops in several stages and involves the formation of the septum primum and septum secundum. The septum primum grows from the roof of the common atrium toward the endocardial cushions of the atrioventricular canal. Initially, it does not completely separate the two atrial cavities. The gap between the septum primum and the endocardium is called the ostium primum. Before the ostium primum closes, apoptosis in the superior portion of the septum primum leads to the formation of the ostium secundum, which maintains right-to-left shunting of oxygenated blood. Around the fifth week of intrauterine life, a fold forms in the atrial wall, giving rise to the septum secundum, which develops to the right of the septum primum. The septum secundum does not fully separate the atria. The remaining opening between the two chambers is the foramen ovale. The septum primum and septum secundum overlap, creating a valve-like structure that permits right-to-left shunting during fetal life. At birth, increased left atrial pressure functionally closes this valve, and over time the septal structures typically fuse, resulting in permanent closure of the foramen ovale.2–6
The atrial septal plane is oriented at approximately 65°, extending from the posterior right to the anterior left. The true interatrial septum is defined as the portion that can be removed without exiting the atrial cavities. The fossa ovalis is surrounded by a muscular rim. However, only a small part of this rim belongs to the true septum; the remainder consists of infolded right atrial wall. Posteriorly and inferiorly, the rim continues as the wall of the inferior vena cava, forming Sondergaard’s groove, which serves as a surgical access route to the left atrium. Between the superior vena cava and the insertion of the right pulmonary veins, the rim is derived from the embryological septum secundum. The aortic mound lies very close to the anterosuperior rim. During interventional procedures, a transseptal puncture performed at this level risks perforating the aortic root.7,8
In more than 70% of individuals, the valve of the fossa ovalis is large enough to overlap the rim completely, resulting in functional and eventual anatomical closure of the interatrial septum. However, in a significant proportion of the population, the valve is not sufficiently large. This results in a residual communication between the two atria, typically located in the anterosuperior quadrant of the rim. This communication is known as a patent foramen ovale (PFO). Autopsy studies have shown that PFO size varies widely, ranging from 1 mm to 19 mm, with a mean diameter of approximately 5 mm. In most cadaveric studies, the diameter was less than 10 mm.9–11
The anatomy of a PFO is highly variable, and accurate characterization is essential for selecting the appropriate closure technique. While most PFOs open and close intermittently, in some cases the valve may be held open by a fold of tissue on the left atrial side, resulting in a continuous left-to-right shunt. The mechanism and anatomical features are most commonly assessed using three-dimensional transesophageal echocardiography.12–15
Several additional anatomical features should be considered during PFO evaluation. An atrial septal aneurysm, defined as septum primum excursion of at least 10 mm between the atria, may retract the septum primum, increase the shunt area, and necessitate a larger occluder during percutaneous closure. Furthermore, embryologic remnants of the right sinus venosus valve, such as a prominent Eustachian valve or a Chiari network, can direct blood flow toward the right atrial aspect of the PFO, potentially increasing the technical difficulty of the closure procedure.16–21
Echocardiographic assessment of PFO typically includes contrast-enhanced transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE), with or without contrast.
In TTE, the most commonly used contrast agent is agitated saline, although transpulmonary contrast agents such as SonoVue may also be used. For PFO assessment, agitated saline is preferred. Mixing saline with a small amount of air produces microbubbles that cannot pass through the pulmonary microcirculation, resulting in opacification of the right heart chambers only. The appearance of bubbles in the left heart chambers indicates the presence of a right-to-left shunt. The protocol should include at least one injection at rest, followed by two additional injections during provocative maneuvers, such as coughing or the Valsalva maneuver. The preferred TTE views are the apical four-chamber and subcostal four-chamber views. Shunt severity is graded semi-quantitatively based on the number of microbubbles crossing the PFO: mild (≤ 9 bubbles), moderate (10–20 bubbles), or severe (> 20 bubbles).22
TEE provides superior visualization of the interatrial septum and allows differentiation between an atrial septal defect and a PFO. It can be performed with or without contrast, typically using agitated saline. Assessment of the interatrial septum is performed in mid-esophageal views at 0–20°, 40–80°, and in the bicaval view (80–120°), with the addition of color Doppler imaging to detect shunting.22,23
Transcranial Doppler (TCD) ultrasound using agitated saline is a noninvasive, inexpensive, and relatively sensitive method for screening and diagnosing right-to-left shunts. A meta-analysis of 29 studies comparing contrast-enhanced TCD with contrast TEE reported a sensitivity of 94% and a specificity of 92% for TCD. The technique uses an ultrasound transducer (either a dedicated Doppler probe or a 2 MHz probe) to interrogate blood flow in the major cerebral arteries, most commonly the middle cerebral artery, through the temporal bone window. After obtaining an adequate pulsed-wave Doppler signal, agitated saline is injected. As with contrast-enhanced echocardiography, the assessment is performed both at rest and during provocative maneuvers, such as the Valsalva maneuver. Results are graded using a semiquantitative scale. The test is considered positive if at least one microbubble-triggered signal, visible on the pulsed-wave Doppler tracing and audible as a characteristic ‘blip’, is detected within 25 s after injection. The right-to-left shunt is graded as:24–28
Grade 1 – 1 to 10 microbubbles
Grade 2 – 11 to 30 microbubbles
Grade 3 – 31 to 100 microbubbles
Grade 4 – 101 to 300 microbubbles
Grade 5 – more than 300 microbubbles
Sectional imaging can also be used to detect PFO. However, cardiac computed tomography (CT) and CT angiography are less commonly used than echocardiographic techniques, mainly due to higher costs. ECG-gated cardiac CT offers certain advantages, particularly improved patient comfort. This may be especially relevant for patients with cryptogenic stroke, who may have difficulty cooperating with or tolerating TEE. On cardiac CT, left-to-right shunts can be identified by injecting saline after contrast administration. In some cases, saline may not be required, as a channel-like jet of contrast passing through the interatrial septum can be visualized. Nevertheless, single-phase cardiac CT is generally considered less sensitive than TEE for detecting PFO.29–32
Recent advancements in CT protocols, such as full cardiac cycle imaging, may improve the detection rate of PFO. This approach can also allow simultaneous assessment of coronary artery disease and interatrial communications in selected patients. In this subgroup, a coronary CT angiography protocol with ECG gating provides detailed anatomical information and enables imaging throughout the cardiac cycle, facilitating the identification of interatrial septal defects or PFO. The CT criteria used for PFO detection in these studies are:33
Presence of a flap in the left atrium at the expected location of the interatrial septum
Presence of a continuous column of contrast material across the septum
Presence of a jet of contrast material extending from the contrast column into the right atrium
In conclusion, although cardiac CT is not the gold standard for PFO imaging, it can provide valuable information about cardiac anatomy when echocardiographic assessment is inconclusive or not feasible. This may occur in patients with poor transthoracic acoustic windows or in those unable to tolerate TEE due to esophageal pathology or limited cooperation. Moreover, if a patient undergoes contrast-enhanced thoracic CT for another indication, careful evaluation of the interatrial septum should be performed to assess for the presence of a PFO.
A right-to-left shunt may allow venous emboli to enter the systemic arterial circulation, potentially causing acute ischemic infarctions in various organs. The most commonly described manifestation is PFO-related stroke, often classified as a form of cryptogenic stroke.34
For a PFO-related stroke to occur, a thrombus must form in the PFO tunnel, the systemic venous circulation, or the right atrium. Thrombus formation may result from several mechanisms, including prolonged immobility (e.g., after surgery or long-distance travel), trauma, coagulopathies, or the presence of intravascular foreign material such as central venous catheters, pacemaker leads, or chemotherapy ports. Additionally, anatomical variants, such as prominent remnants of the right sinus venosus valve (Eustachian valve or Chiari network), may increase right-to-left shunting and thereby increase the risk of paradoxical embolism.35–38
Emboli can pass from the right atrium to the left atrium when hemodynamic conditions favor a right-to-left shunt. This occurs in two main situations. The first, and most commonly described mechanism, is a transient increase in right atrial pressure relative to left atrial pressure, such as during deep inspiration or early systole. This mechanism can be readily demonstrated during contrast (bubble) studies. The second mechanism involves alterations in normal right atrial blood flow from the inferior vena cava and has been described in association with platypnea-orthodeoxia syndrome. In 4D flow magnetic resonance imaging (MRI) studies, the normal pattern consists of clockwise blood flow from the venae cavae within the right atrium. However, in some individuals, inferior vena cava flow resembles the embryological pattern, with counterclockwise streaming that directs blood from the inferior vena cava across the PFO into the left atrium.39–41
After passing into the left ventricle, an embolus often reaches the cerebral circulation due to the anatomy of the aortic arch. Computational models of the aorta have shown that small emboli (1–2 mm) tend to travel toward the superior aspect of the arch, placing them closer to the origins of the carotid and vertebral arteries. Populationbased registries have reported that cardioembolic strokes more frequently involve the left hemisphere (approximately 56% of cases) compared with the right hemisphere (44%). It remains unclear whether this difference reflects true anatomical and hemodynamic factors or underdiagnosis of right hemispheric events, particularly transient ischemic attacks (TIAs), which may be less noticeable to patients. Even small emboli (1–2 mm) can cause clinically significant TIAs, whereas embolic infarctions of similar size in other organs may go undetected due to the absence of obvious symptoms.42–48
Another embolic ischemic event associated with PFO is myocardial infarction. In this setting, an embolus may enter the coronary circulation and cause acute myocardial infarction with non-obstructive coronary arteries (MINO-CA). Because emboli are typically smaller than the diameter of the main coronary arteries, they tend to lodge in distal branches, leading to ischemia despite the absence of significant epicardial coronary obstruction.49,50
Migraine is a common headache disorder, affecting approximately 12% of adults. It is often preceded by neurological symptoms known as aura. Aura most frequently includes visual disturbances, such as scotomas, visual distortions, or photopsia. Sensory symptoms (e.g., paresthesia or numbness), language disturbances (paraphasia, receptive aphasia, or word-finding difficulty), tinnitus, vertigo, ataxia, and even motor symptoms such as hemiparesis or hemiplegia may also occur. Some aura manifestations can be difficult to distinguish from a TIA. Aura symptoms typically last between 5 and 60 min, are fully reversible, and are usually followed by headache.51–54
Epidemiological studies have shown a higher prevalence of PFO in patients with migraine with aura compared with individuals without migraine and even compared with those with migraine without aura. Several studies have described a progressively increasing degree of right-to-left shunting among individuals without migraine, those with migraine without aura, and those with migraine with aura. However, a clear and consistent association between shunt severity and the presence of aura has not been definitively established. Multiple hypotheses have been proposed to explain this association. One theory involves microembolization from the peripheral venous circulation to the cerebral circulation through the PFO, as suggested by the occurrence of microbubbles during contrast studies. Another hypothesis implicates vasoactive substances that bypass pulmonary metabolism via the PFO and subsequently trigger cortical phenomena leading to aura. Serotonin is one such candidate, as it functions both as a neurotransmitter and a vasoactive substance and is normally metabolized in the pulmonary circulation. An additional potential mechanism is microembolization from thrombi forming within the PFO tunnel, a hypothesis supported by case reports. These mechanisms are summarized in Figure 1.55–61
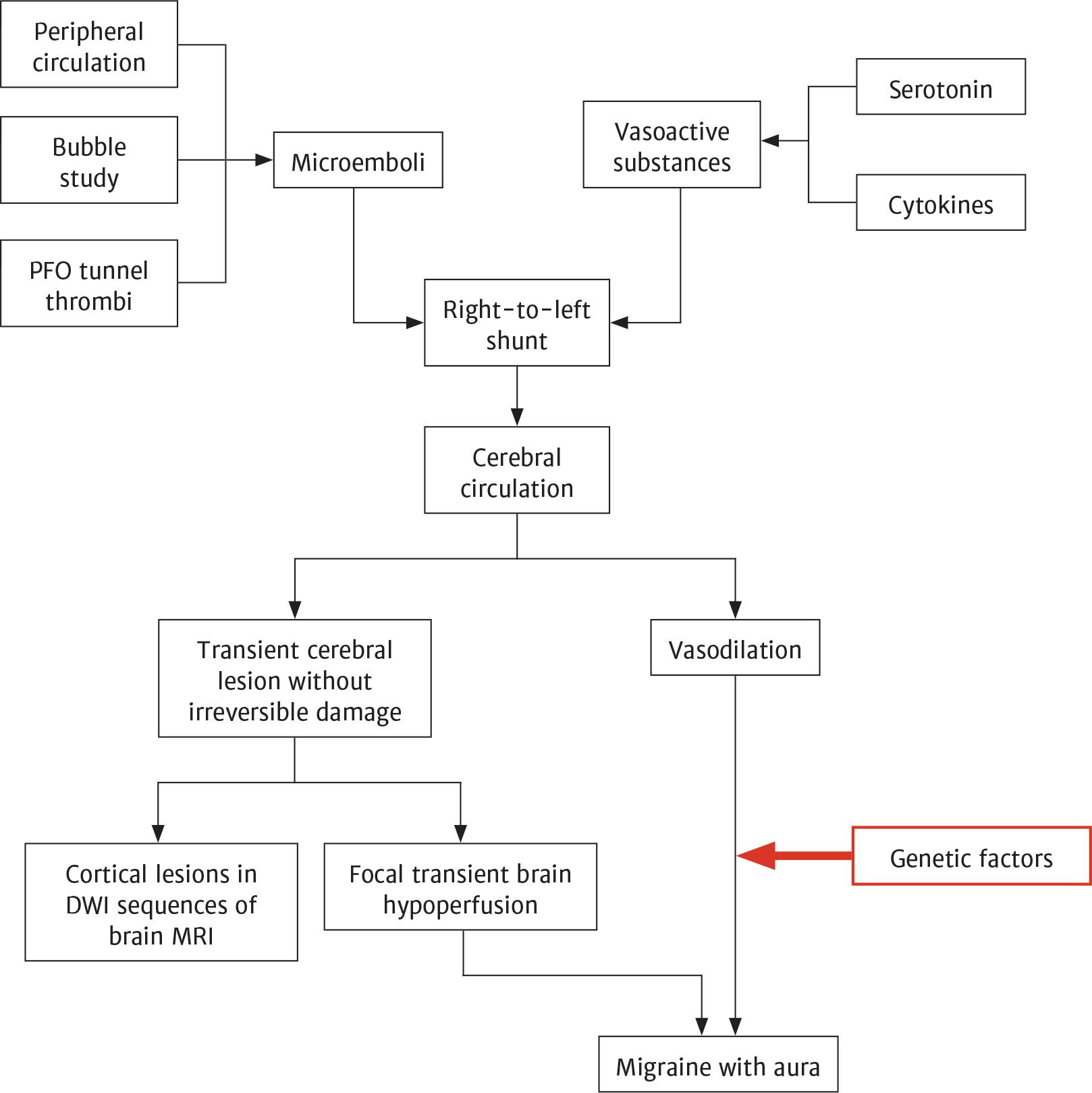
Proposed mechanisms for migraines with aura in PFO patients.
However, the impact of PFO closure on migraine has not been definitively established. Although the PREMIUM (Prospective Randomized Investigation to Evaluate Incidence of Headache Reduction in Subjects with Migraine and PFO Using the Amplatzer PFO Occluder Compared to Medical Management) and PRIMA (Percutaneous Closure of Patent Foramen Ovale in Migraine with Aura) trials reported reductions in migraine frequency and the number of migraine days, their results were not consistent. Moreover, some patients experienced an increased frequency of migraine after transcatheter atrial septal defect closure (non-PFO), which challenges the simple right-to-left shunt hypothesis. In patients undergoing atrial septal defect closure, dual antiplatelet therapy with aspirin and clopidogrel was associated with a lower frequency of migraine attacks compared with aspirin alone.62–65
Platypnea–orthodeoxia syndrome is characterized by dyspnea and systemic hypoxemia that worsen in the upright position. Although rare, it has been associated with right-to-left shunting through a PFO. Given the high prevalence of PFO in the general population, additional hemodynamic factors are required to trigger the syndrome.
To confirm PFO as the cause of systemic hypoxemia, cardiac catheterization may be necessary. Measurement of oxygen saturation in the right and left atria, as well as in each pulmonary vein, helps clarify the underlying mechanism. In platypnea–orthodeoxia syndrome, pulmonary venous oxygen saturation is normal, whereas left atrial oxygen saturation is reduced due to significant right-to-left shunting. These findings are particularly relevant in the absence of pulmonary hypertension, as assessed by echocardiography or confirmed during catheterization.67–69
The association between PFO and cryptogenic systemic thromboembolism has been extensively studied in epidemiological research. However, the evidence remains controversial and appears to vary depending on the clinical context and specific PFO characteristics.
The indication for PFO closure is determined by estimating the likelihood that the PFO contributed to the clinical event, as well as the risk of recurrence. Patients with a high probability of PFO-related events have a clear indication for closure, whereas in intermediaterisk cases, the decision should be guided by careful clinical judgment.28,70
Given that PFO is present in approximately 25% of the general population, additional factors clearly influence the risk of systemic thromboembolism in affected individuals. The European Society of Cardiology Position Statement on the management of patients with PFO outlines several variables that should be evaluated when considering interventional closure:
PFO morphology – size, location, and tunnel length
Adjacent anatomical structures – distances between the defect and major vessels (aortic root, venae cavae), as well as between the defect and the atrial free wall
Interatrial septal anatomy – presence of an atrial septal aneurysm or additional septal defects; thickness of the septum primum and septum secundum
Presence of a prominent Eustachian valve
Presence of a Chiari network
Shunt characteristics – degree of blood flow across the PFO, assessed by color Doppler echocardiography at rest and during a Valsalva maneuver.
The evaluation of cryptogenic thromboembolism affecting the left circulation should begin with a thorough search for arrhythmias. A 12-lead ECG and 24-hour Holter monitoring are recommended to detect paroxysmal atrial fibrillation. If atrial fibrillation is not identified, some authors suggest prolonged monitoring for up to 6 months using an insertable cardiac monitor, as randomized controlled trials and observational studies have shown higher detection rates of paroxysmal atrial fibrillation with extended monitoring.71–73
Once atrial fibrillation has been excluded in a patient with cryptogenic stroke and PFO, the risk of recurrent stroke and the patient’s age should be considered when selecting treatment.
Medical therapy includes two main classes of drugs: antiplatelet agents and oral anticoagulants. There are no large randomized controlled trials directly comparing individual drugs specifically in PFO-associated stroke. Most available data are observational, and only one randomized trial has compared oral anticoagulation with antiplatelet therapy in this setting. Although anticoagulants likely increase bleeding risk compared with antiplatelet agents, their superiority in preventing recurrent ischemic stroke remains uncertain. A meta-analysis evaluating secondary prevention in PFO-related stroke, including comparisons between these two treatment strategies, reported significant imprecision in the available evidence.74
When evaluating the potential benefit of PFO closure, the European Stroke Organization recommends an individualized approach. This includes assessing the Risk of Paradoxical Embolism (RoPE) score to estimate the likelihood that the PFO is causally related to the stroke, and further stratifying patients using the PASCAL classification system to guide management decisions.70,75 The RoPE score takes into account:
- A.
Age – younger age is associated with a higher score:
18–29 years – 5 points
30–39 years – 4 points
40–49 years – 3 points
50–59 years – 2 points
60–69 years – 1 point
>70 years – 0 points
- B.
Cortical infarct on imaging – 1 point
- C.
Non-smoking status – 1 point
- D.
Absence of the following conditions – 1 point each:
Diabetes mellitus
Prior stroke or TIA
Hypertension
A high RoPE score is defined as ≥ 7 points. The PASCAL classification system categorizes strokes as unlikely related to PFO, possibly related to PFO, or probably related to PFO. According to this system, the presence of either a high-risk PFO feature, such as a large shunt (defined as > 20 microbubbles crossing on TEE) or an atrial septal aneurysm (≥ 10 mm excursion from the midline), or a high RoPE score classifies the stroke as possibly related to PFO. When both criteria are present, the stroke is considered probably related to PFO.
However, this scoring system has several limitations. First, it relies primarily on clinical variables and the presence of a cortical infarct on imaging, without incorporating morphological characteristics of the PFO, such as shunt size, tunnel length, or regional septal anatomy. In addition, it was designed to estimate the probability of a causal relationship between PFO and cryptogenic stroke, but it does not assess the risk of recurrence.76
In patients aged 18–65 years (according to the 2019 European Consensus Paper) or 18–60 years (according to the 2024 European Stroke Organization guidelines) who have no identifiable cause of stroke other than a PFO, guideline-directed PFO closure may be recommended in selected cases. The ESO guidelines specifically recommend PFO closure combined with antiplatelet therapy in patients aged 18–60 years who are classified as having possible or probable PFO-associated stroke according to the PASCAL classification.
PFO closure is typically performed in specialized centers using a femoral venous approach. In rare cases where access via the inferior vena cava is not feasible, a jugular approach may be considered. The procedure has a high success rate, exceeding 95%, with an acceptable complication profile. Intraprocedural imaging of the interatrial septum is essential for procedural success, as it enables appropriate device sizing and precise guidance during deployment. TEE under general anesthesia generally provides optimal image quality. When general anesthesia is not suitable, the procedure can be performed under local anesthesia with intracardiac echocardiography for imaging guidance. Careful anatomical assessment is crucial for selecting the appropriate device and minimizing complications.77,78
Commonly used PFO closure devices include those from Abbott (Amplatzer PFO Occluder, Amplatzer Multifenestrated Septal Occluder), Occlutech (Figulla Flex II), and Gore (Cardioform Septal Occluder).79
Preprocedural medical management usually includes antiplatelet therapy. During the procedure, unfractionated heparin is administered, with an activated clotting time maintained above 250 s to reduce the risk of device thrombosis.
In patients undergoing PFO closure, there is no clear consensus regarding the optimal dose and duration of antiplatelet therapy. In most clinical trials, patients received dual antiplatelet therapy (DAPT) with aspirin and clopi-dogrel starting on the morning of the procedure, without a loading dose. In contrast, in the REDUCE trial, patients received single antiplatelet therapy with clopidogrel, including a 300 mg loading dose on the day of the procedure. The SCAI guidelines recommend DAPT for at least one month after PFO closure but do not provide recommendations beyond this period due to limited evidence.80,81 A retrospective study comparing long-term antiplatelet therapy (defined as ≥ 6 months) with short-term therapy found no significant difference in clinical outcomes.82,83
According to the 2024 ESO guidelines for PFO management, dual antiplatelet therapy (aspirin plus clopidogrel) is suggested for 1–6 months, depending on the protocol used in the randomized trial of the specific occluder device. This is followed by long-term single antiplatelet therapy with aspirin for at least 5 years after percutaneous closure. Although based on very low-quality evidence, the guidelines recommend PFO closure combined with antiplatelet therapy over long-term anticoagulation alone in patients with possible or probable PFO-related stroke.70
The guidelines do not provide definitive recommendations for antiplatelet or anticoagulant therapy in patients who decline PFO closure, instead advising an individualized approach that considers bleeding risk and the risk of stroke recurrence. While oral anticoagulation has been associated with a lower risk of recurrent stroke compared with antiplatelet therapy, it carries a significantly higher risk of major bleeding.84 These recommendations apply primarily to patients aged 18-60 years. Data in older patients with PFO and cryptogenic stroke are limited. In this population, the risk of arrhythmia is higher, and expert consensus suggests prolonged cardiac rhythm monitoring to detect infrequent paroxysmal atrial fibrillation, which may warrant anticoagulation.
Procedural complications include:
Vascular complications
Cardiac tamponade
Hemothorax
Pneumothorax
Aortic root injury
Atrial fibrillation
Residual shunt
Device-related complications include:
Device thrombosis
Device migration
Nickel allergy
Vascular complications typically occur at the venous puncture site and include ecchymoses and hematomas. These are generally mild and rarely require surgical intervention.85
Severe, life-threatening complications, such as cardiac tamponade, hemothorax, pneumothorax, or aortic root injury, are very rare and usually occur during the procedure. Careful preprocedural assessment of cardiac anatomy and meticulous technique when crossing the interatrial septum are essential to minimize these risks.86
Postprocedural supraventricular arrhythmias are relatively frequent complications and may result from local atrial inflammation, reentry circuits related to the device, or transient left atrial dysfunction. A meta-analysis published in EuroIntervention in 2019 reported a significantly higher incidence of early-onset atrial fibrillation or atrial flutter (defined as occurring within 45 days after PFO closure) in the closure group compared with medical therapy alone (3.2% vs. 0.47%). Most episodes resolved spontaneously or after cardioversion and were not associated with documented long-term recurrence.87
However, the true incidence of PFO closure-associated atrial fibrillation may be higher than previously reported. A single-center prospective study using implantable loop recorders or 4-week external loop recorders found an incidence of 20.9% in high-risk patients (aged >55 years, with cardiovascular risk factors, prior palpitations, or supraventricular ectopy). In that study, 88.3% of patients with supraventricular tachyarrhythmia had atrial fibrillation lasting more than 30 s. Most episodes occurred within 2 weeks of the procedure, with few recurrences beyond one month.88 These findings underscore the importance of systematic rhythm monitoring in high-risk patients to enable timely diagnosis and appropriate management.
Residual shunt may be detected in up to 25% of patients at 6 months after PFO closure. Its occurrence has been associated with:
Use of larger closure devices
Extreme tunnel length (very short or very long)
Presence of an atrial septal aneurysm
A multiperforated interatrial septum
However, reported prevalence rates vary widely across studies, ranging from 0.6% to 29%, reflecting significant heterogeneity in study design and assessment methods. In addition, the impact of residual shunt on subsequent neurological events remains uncertain, as available studies have yielded conflicting results.79
Device embolization is an uncommon complication, reported in fewer than 1% of procedures. The risk is higher in patients with a thick septum secundum or a hypermobile septum primum, as incomplete anchoring of the device on both sides of the PFO may occur.89
Device thrombosis is more frequent than embolization and has been primarily associated with older-generation devices. In the major contemporary PFO closure trials (CLOSE, RESPECT, REDUCE), only two cases of device thrombosis were reported in the REDUCE trial, both with favorable outcomes under anticoagulation therapy.81,90,91
Nickel alloys are key components of most occluder devices. Although rare, nickel hypersensitivity has been reported after PFO closure. Case reports describe symptoms such as chest pain, dyspnea, migraine, and, in some instances, a significant inflammatory response. While symptoms may resolve spontaneously after endothelialization of the device, some patients have required corticosteroid therapy or even device removal. In patients with known nickel allergy, Gore Helex septal occluders appear to be less allergenic.92
PFO remains an important topic of interest for the medical community, as ongoing research continues to identify new clinical syndromes associated with PFO. Moreover, given that many current recommendations are based largely on expert consensus, further well-designed studies are needed to better define optimal medical and interventional management strategies and potentially establish new indications for PFO closure.