Peripheral artery disease (PAD) affects about 6% of adults worldwide, with increasing prevalence.1 The most severe form, chronic limb-threatening ischemia (CLTI), involves rest pain, ischemic ulcers, or gangrene, and is linked to high rates of amputation, hospitalization, and mortality.2 Despite available advanced treatments, patient outcomes vary widely, indicating that factors like psychological or behavioral components may significantly influence results. Depression is found in 16% to 35% of patients with PAD,3 while anxiety disorders occur in 24.4% to 29%.4,5 Recent research highlights that both depression and anxiety are emerging as important risk factors affecting morbidity and mortality.6
For a better understanding of this association, different mechanisms have been theorized. From a behavioral perspective, the presence of affective disorders may impair adherence to pharmacological treatment, dissuade smoking cessation, and lead to improper wound care.7 Moreover, from a physiological standpoint, several stress–related and depression-mediated responses have been hypothesized, including hypothalamic–pituitary–adrenal (HPA) axis dysregulation, autonomic system dysregulation, immune system dysregulation, and endothelial and coagulation dysfunction, which may present with an increased risk of cardiovascular disease.7
This study aims to identify and analyze the risk factors associated with the presence of anxiety or depressive disorders in patients with CLTI. Considering the proposed function of systemic inflammation in the progression of CLTI and mood disorders, this study also analyzed specific inflammatory biomarkers to investigate whether detectable inflammatory activity is associated with the occurrence of depression or anxiety disorders.
In this monocentric, retrospective, observational study, all patients diagnosed with CLTI admitted to the Vascular Surgery Clinic of the Târgu Mureş County Emergency Clinical Hospital from January 2020 to December 2023 were included. Patients with a history of surgical or endovascular procedures were excluded from the study. Additionally, patients who tested positive for COVID-19 or had a confirmed diagnosis within the 3 months before admission were excluded due to increased systemic inflammation.8–12 A total of 113 patients were enrolled in the study, of whom 88 (77.88%) were male, with a mean age of 70.54 ± 8.96 years.
All information related to demographic data, comorbidities, risk factors, and laboratory data from the first 12 h of admission was collected from the hospital’s electronic database. Additionally, cardiovascular events (history of myocardial infarction or angina pectoris) and cerebrovascular events (including stroke or transient ischemic attack) were documented. The presence of depression or anxiety disorders was ascertained through documented diagnoses in the hospital’s electronic medical records. These diagnoses were based on previous evaluations conducted by treating physicians; however, they were not derived from standardized psychiatric assessments or validated screening instruments such as PHQ-9 and GAD-7. Regarding systemic inflammation, the biomarkers neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), and leukocyte glucose index (LGI) were used, calculated according to the published formulas.13–17 Systemic inflammation was quantified using calculated biomarkers derived from complete blood count and glucose values. No fixed clinical cutoff was applied; instead, biomarker values were analyzed as continuous measures to compare inflammatory burden between groups.
Statistical analyses were conducted using SPSS for Mac OS v.29.0.2.0 (SPSS). Comorbidities, risk factors, and clinical severity are presented as counts and percentages. Age and length of stay are reported as mean ± s.d. All laboratory data are expressed as medians with first (Q1) and third quartiles (Q3). The Mann–Whitney and Student’s t-tests were used to analyze differences in continuous variables, while the chi-squared test was used to assess differences between categorical variables. Univariate analysis identified risk factors associated with depression or anxiety disorders in patients with CLTI. All tests were two-tailed, with a p value < 0.05 indicating statistical significance.
A total of 113 patients with CLTI were enrolled in the study, with a mean age of 70.54 ± 8.96 years. Regarding comorbidities, the most prevalent were hypertension in 101 patients (89.38%), ischemic heart disease in 72 patients (63.72%), diabetes mellitus in 70 patients (61.95%), and chronic heart failure in 42 patients (37.17%). Active smoking was the most common risk factor, affecting 73 patients (64.60%), followed by dyslipidemia in 52 patients (46.02%) and obesity in 26 patients (23.01%) (Table 1). Additionally, 47 patients (41.59%) were diagnosed with stage III Leriche-Fontaine, and 66 patients (58.41%) were diagnosed with stage IV Leriche-Fontaine (Table 1). From the entire cohort, 14 patients (12.39%) were diagnosed with depression or anxiety disorder.
Characteristics of the included patients
| Variable | Patients (n = 113) |
|---|---|
| Age, years, mean ± s.d. | 70.54 ± 8.96 |
| Male, n (%) | 88 (77.88%) |
| Comorbidities and risk factors, n (%) | |
| Hypertension | 101 (89.38%) |
| Ischemic heart disease | 72 (63.72%) |
| Chronic heart failure | 42 (37.17%) |
| Atrial fibrillation | 12 (10.62%) |
| Cardiovascular events | 16 (14.16%) |
| Cerebrovascular events | 21 (18.58%) |
| Diabetes mellitus | 70 (61.95%) |
| Chronic obstructive pulmonary disease | 12 (10.62%) |
| Obesity | 26 (23.01%) |
| Active smoking | 73 (64.60%) |
| Dyslipidemia | 52 (46.02%) |
| Laboratory data, median (Q1-Q3) | |
| Hemoglobin, g/dl | 13.0 (11.5-14.0) |
| Hematocrit, % | 38.20 (34.15-42.25) |
| WBC | 9.16 (7.32-10.51) |
| BUN, mg/dl | 38.5 (30.4-55.64) |
| Creatinine, mg/dl | 0.91 (0.78-1.16) |
| eGFR, ml/min/1.73 m2 | 84.76 (60.44-103.34) |
| Glucose, mg/dl | 117.0 (96.1-148.45) |
| Neutrophils, × 103/μl | 6.27 (4.73-7.71) |
| Lymphocytes, × 103/μl | 1.80 (1.44-2.26) |
| Monocytes, × 103/μl | 0.65 (0.51-0.85) |
| PLT, × 103/μl | 249.35 (205.25-307.1) |
| Clinical severity, n (%) | |
| Stage III Leriche-Fontaine, n (%) | 47 (41.59%) |
| Stage IV Leriche-Fontaine, n (%) | 66 (58.41%) |
| Depression or anxiety disorder, n (%) | 14 (12.39%) |
| Length of stay, days, mean ± s.d. | 6.27 ± 4.03 |
Based on the presence of depression or anxiety disorders, no significant differences were observed concerning demographic data, comorbidities, and risk factors, with the exception of cardiovascular events (35.71% vs. 11.11%; p = 0.013) and cerebrovascular events (64.29% vs. 12.12%; p < 0.001) (Table 2). Regarding laboratory findings, only blood urea nitrogen (BUN) levels were higher in patients with depression or anxiety disorder (p = 0.023). Furthermore, no differences were noted regarding the clinical severity of the patients (Table 2).
Demographic data, comorbidities, risk factors, and laboratory data based on the presence of depression or anxiety disorder
| Variable | Depression or anxiety disorder | p value | |
|---|---|---|---|
| No (n = 99) | Yes (n = 14) | ||
| Age, years, mean ± s.d. | 70.37±9.15 | 71.71±7.32 | 0.656 |
| Male, n (%) | 79 (79.80%) | 9 (64.29%) | 0.191 |
| Hypertension, n (%) | 90 (90.91%) | 11 (78.57%) | 0.161 |
| Ischemic heart disease, n (%) | 60 (60.61%) | 12 (85.71%) | 0.067 |
| Chronic heart failure, n (%) | 39 (39.39%) | 3 (21.43%) | 0.193 |
| Atrial fibrillation, n (%) | 11 (11.11%) | 1 (7.14%) | 0.652 |
| Cardiovascular events, n (%) | 11 (11.11%) | 5 (35.71%) | 0.013 |
| Cerebrovascular events, n (%) | 12 (12.12%) | 9 (64.29%) | <0.001 |
| Diabetes mellitus, n (%) | 61 (61.62%) | 9 (64.29%) | 0.529 |
| Chronic obstructive pulmonary disease, n (%) | 11 (11.11%) | 1 (7.14%) | 0.652 |
| Obesity, n (%) | 20 (20.20%) | 6 (42.86%) | 0.059 |
| Active smoking, n (%) | 64 (64.65%) | 9 (64.29%) | 0.979 |
| Dyslipidemia, n (%) | 45 (45.45%) | 7 (50.00%) | 0.749 |
| Hemoglobin, g/dl | 13.02 (11.62–14.03) | 12.40 (10.28–13.58) | 0.312 |
| Hematocrit, % | 38.25 (34.5–42.0) | 36.11 (32.95–42.8) | 0.593 |
| WBC | 8.94 (7.11–10.49) | 9.58 (9.16–10.52) | 0.118 |
| BUN, mg/dl | 36.44 (29.8–50.77) | 48.1 (38.1–71.4) | 0.023 |
| Creatinine, mg/dl | 0.91 (0.76–1.09) | 1.08 (0.83–1.29) | 0.305 |
| eGFR, ml/min/1.73 m2 | 85.82 (62.49–104.34) | 70.54 (43.31–99.80) | 0.199 |
| Glucose, mg/dl | 118.45 (96.13–150.4) | 114.0 (95.0–121.0) | 0.448 |
| Neutrophils, × 103/μl | 6.26 (4.56–7.65) | 6.27 (5.92–8.32) | 0.308 |
| Lymphocytes, × 103/μl | 1.80 (1.43–2.19) | 1.94 (1.55–2.92) | 0.426 |
| Monocytes, × 103/μl | 0.65 (0.50–0.86) | 0.73 (0.52–0.79) | 0.849 |
| PLT, × 103/μl | 246.5 (202.25–311.5) | 254.85 (232.5–290.1) | 0.657 |
| Stage III Leriche–Fontaine, n (%) | 42 (42.42%) | 5 (35.71%) | 0.634 |
| Stage IV Leriche–Fontaine, n (%) | 57 (57.58%) | 9 (64.29%) | |
| Length of stay, days, mean ± s.d. | 6.02 ± 3.96 | 8.00 ± 4.18 | 0.064 |
Regarding systemic inflammation, no differences were found between patients with depression or anxiety disorders and other patients in the mean levels of the following biomarkers: NLR (4.01 vs. 4.14; p = 0.905), PLR (143.43 vs. 158.43; p = 0.817), MLR (0.32 vs. 0.42; p = 0.371), and LGI (1.05 vs. 1.28; p = 0.885) (Figure 1).
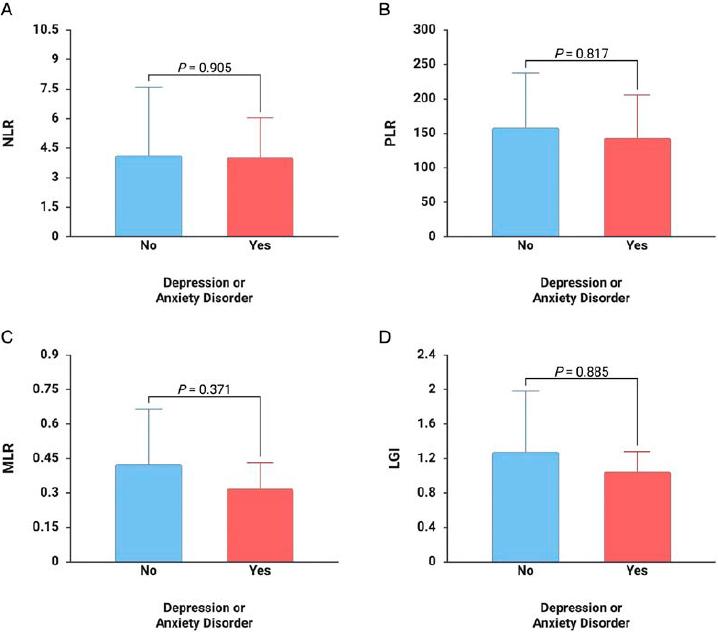
Differences between patients with and without depression or anxiety disorders for NLR (A), PLR (B), MLR (C), and LGI (D).
In the univariate analysis, although men appeared to have twice the risk of depression or anxiety disorder compared with women, the difference was not statistically significant (odds ratio (OR) 2.19; p = 0.199). Age and ischemic heart disease showed no association with these mental health conditions. In contrast, cardiovascular events (OR 4.44; p = 0.020) and cerebrovascular events (OR 13.05; p < 0.001) were linked to depression or anxiety. No connections were found between active smoking, obesity, or clinical severity and these disorders (Table 3).
Univariate analysis of risk factors for depression or anxiety disorder in patients with CLTI
| Variable | Depression or anxiety disorder | ||
|---|---|---|---|
| OR | 95% CI | p value | |
| Male | 2.19 | 0.66–7.27 | 0.199 |
| Age | 1.16 | 0.66–2.02 | 0.598 |
| Ischemic heart disease | 3.90 | 0.83–18.38 | 0.085 |
| Cardiovascular events | 4.44 | 1.26–15.67 | 0.020 |
| Cerebrovascular events | 13.05 | 3.74–45.49 | <0.001 |
| Active smoking | 0.98 | 0.31–3.16 | 0.979 |
| Obesity | 2.96 | 0.92–9.51 | 0.068 |
| Leriche–Fontaine classification | |||
| Stage III | 0.75 | 0.24–2.41 | 0.634 |
| Stage IV | 1.33 | 0.41–4.25 | |
The primary findings of this study demonstrate an association between a history of cardiovascular and cerebrovascular events and an increased risk of depression or anxiety disorders in patients with CLTI. Although the results did not attain statistical significance, patients with obesity or ischemic heart disease exhibited a tendency toward increased odds of depression or anxiety disorders, with OR values of approximately 3. These findings imply potential associations that merit further investigation in larger cohorts.
Multiple overlapping biological mechanisms likely explain the connection between CLTI and affective disorders.18 Atherosclerosis and the accompanying systemic inflammation are mechanistically linked to depression and anxiety: increased peripheral cytokines and other inflammatory mediators are associated with both mood disorders and poorer PAD outcomes.18–21 CLTI is a severe condition marked by persistent ischemia and repeated tissue damage, leading to increased pro-inflammatory signaling and changes in neurotransmitter metabolism, HPA-axis activity, and neural plasticity, key physiological pathways linked to major mood disorders.18–21 In patients with PAD, inflammatory markers are associated with the severity of depressive symptoms, indicating a biological connection between vascular issues and mood disorders.18–21
Patients with CLTI face various challenges related to symptom burden and sensory experiences, both of which are significant psychological stressors that can lead to mood disorders.21,22 Ongoing ischemic rest pain, nonhealing ulcers, nocturnal discomfort, and sleep disruption cause chronic nociceptive input, diminishing quality of life.21–23 Chronic pain conditions are closely linked to depression and anxiety, and in CLTI, the severity of pain is strongly associated with functional limitations and loss of independence.23,24 Patients with CLTI often present with diabetes, coronary artery disease, chronic kidney disease, and polypharmacy.25,26 Independently, these conditions have been shown to be risk factors for depression.7 In addition, behavioral risk factors like smoking, physical inactivity, and poor diet, combined with social determinants such as low socioeconomic status and limited access to care, are associated with worse outcomes in patients with CLTI or PAD and with a higher risk of affective disorders.27,28
Healthcare experiences and treatment-related factors also contribute to cognitive disorders.29 Repeated hospital admissions, surgical interventions, prolonged wound care, and risk of amputation are linked to depressive or anxiety symptoms.30–32 Opioid exposure for ischemic pain and sedating medications can worsen mood or mask symptoms, further affecting proper clinical diagnosis and adequate treatment, along with future complications related to substance abuse.33 Additionally, fragmented care leads to under-detection of psychiatric disorders and poorer overall clinical outcomes in patients with CLTI.34 Neuroinflammation, cortisol, and hippocampal volume have crucial roles in depression, anxiety, borderline personality disorder, and poor quality of life.35–39
This study has several limitations that need to be acknowledged. Firstly, it was a monocentric, retrospective, observational study, which could introduce selection and information biases. The relatively small sample size restricts the generalizability of the results and the capacity to perform multivariate analysis to control for potential confounders. Another limitation is that depression and anxiety diagnoses were obtained from medical records rather than standardized psychiatric assessments, potentially causing underdiagnosis or misclassification of affective disorders. Larger, multicenter prospective studies are needed to confirm these results, investigate causality, and better understand how inflammation and neurovascular mechanisms contribute to the development of affective disorders in patients with CLTI. Although theoretical models strongly associate inflammation with mood disorders and CLTI severity, the specific biomarkers examined in this study (NLR, PLR, MLR, LGI) did not demonstrate a significant correlation with depression or anxiety. This may be attributable to the limitations inherent in these surrogate markers, which reflect only certain facets of the inflammatory response, as well as the relatively limited sample size and the multifactorial complexity of inflammation in advanced vascular disease. A more comprehensive inflammatory profiling may be necessary to identify clinically meaningful associations.
The absence of significant differences in NLR, PLR, MLR, and LGI between patients with and without depression or anxiety may indicate that these routinely available biomarkers do not fully capture the complex inflammatory milieu characteristic of CLTI. Inflammatory responses in CLTI involve chronic ischemia, endothelial dysfunction, oxidative stress, and neuroimmune interactions, which simple leukocyte ratios may not adequately reflect. Additionally, the small number of patients with affective disorders reduces statistical power. Future studies incorporating broader cytokine panels or longitudinal inflammatory profiling may better elucidate these relationships.
A history of cardiovascular and cerebrovascular events was strongly linked to an increased risk of depression or anxiety in patients with CLTI. This emphasizes the close connection between vascular disease and mental health, indicating that neurological and cardiac conditions might worsen psychological distress in this at-risk group. Although systemic inflammatory biomarkers showed no significant differences between groups, these associations highlight the need to consider both biological and psychosocial factors when managing CLTI. Routinely screening for depression and anxiety, especially in those with a history of cardiovascular or cerebrovascular issues, should be part of vascular care protocols to enable early detection and treatment. Addressing emotional health in CLTI patients can improve treatment adherence, boost rehabilitation success, and possibly decrease morbidity and mortality.