Thoracic aorta false aneurysms (TAFAs) result from a transmural disruption of the aortic wall, with the blood leak contained by the surrounding mediastinal structures. They are a rare but life-threatening complication of aortic surgery, infection, or trauma.1 The development of aortic pseudoaneurysms is often asymptomatic, and their evolution is unpredictable: they may progressively expand or compress and invade adjacent structures.2 The most frequent localization is at an anastomotic site. Current evidence suggests that they are more likely to form just behind the suture lines in the native artery, which is more elastic than the stiff anastomosis and prosthetic graft.3 Surgical and endovascular techniques have significantly advanced, and the optimal treatment strategy should be individually tailored to minimize perioperative complications.4
In connective tissue disorders (CTDs), the mechanisms behind inflammatory stimulation and aortic degeneration differ across conditions. Marfan and Loeys–Dietz syndromes are characterized by abnormal activation of the transforming growth factor-beta (TGF-β) signaling pathway, which plays a key role in initiating the inflammatory response.5 In healthy tissue, TGF-β is bound by fibrillin fibers within the extracellular matrix (ECM), where it participates in normal tissue remodeling. In Marfan syndrome, structural alterations in fibrillin impair its ability to bind TGF-β, resulting in increased TGF-β concentrations in the ECM.6 In Loeys–Dietz syndrome, gene mutations affect the TGF-β receptor, leading to dysregulated receptor activity.5 In both disorders, increased transcription of genes activated by the TGF-β pathway leads to decreased proliferation and increased apoptosis of vascular smooth muscle cells, increased destruction of normal ECM proteins, and increased collagen synthesis. In contrast, the mechanism of aortic degeneration in Ehlers–Danlos syndrome does not involve TGF-β dysregulation. In the vascular type, defective collagen synthesis weakens the structural integrity of the aortic wall and impairs its capacity for renewal.6
Although many studies have described CTDs as a risk factor for aortic aneurysms, their role in the development and management of pseudoaneurysms is not well known.7,8 Therefore, we sought to review the clinical presentation, etiologies, diagnostic methods, surgical techniques, and long-term outcomes of patients with TAFA who underwent surgery at our institution. Our aim was to compare cohorts of patients with and without CTDs.
A total of 116 patients were treated for pseudoaneurysm of the thoracic aorta at the Institute for Clinical and Experimental Medicine, Prague, Czech Republic, between January 1996 and August 2024. From this cohort, we retrospectively evaluated 18 patients with a confirmed CTD. During the same period, more than 1,500 patients underwent thoracic aortic surgery, all of whom were included in our postoperative follow-up program.
All patients with CTDs were diagnosed by genetic screening performed at our institution. Follow-up was obtained for all patients through echocardiographic or computed tomography (CT) assessment. Preoperative, operative, and postoperative data were obtained from the Cardiovascular Information Registry of the Institute for Clinical and Experimental Medicine. Additional information was provided by referring cardiologists and through systematic interviews with patients and family members.
The Kaplan–Meier method and the log-rank test were used to calculate and compare survival estimates for patients with aortic aneurysms and aortic dissections. Statistical analyses were performed using JMP v.15.2.0 (SAS Institute).
Thoracic aortic pseudoaneurysms were identified in 18 patients with CTD over a 28-year follow-up period. Their mean age at the time of aortic surgery was 52 ± 20 years, and 11 patients (61%) were female, whereas most patients without CTD were male. Only two patients were obese, with a BMI of >30 kg/m2.
Most patients (n = 14) had hypertension; atherosclerosis was present in three patients; stroke or other neurological disorders in three patients; and diabetes mellitus in one patient. Only one patient was treated with immunosuppressive therapy. Atrial fibrillation occurred in five patients. In both cohorts, the most common aortic valve disorder was aortic regurgitation, observed in 17 patients with CTD and 72 patients without CTD. Only one patient with CTD had no aortic valve disease. A comparison of the two cohorts is presented in Table 1.
Preoperative demographic characteristics
| Variable | Patients with CTD | Patients without CTD |
|---|---|---|
| Age at the time of surgery, mean ± s.d. (years) | 52 ± 20 | 52 ± 22 |
| Male, n (%) | 7 (39%) | 70 (71%) |
| Female, n (%) | 11 (61%) | 28 (29%) |
| Obesity (BMI > 30 kg/m2), n (%) | 2 (11%) | 25 (25%) |
| Hypertension, n (%) | 14 (78%) | 84 (86%) |
| Diabetes mellitus, n (%) | 1 (5%) | 7 (7%) |
| Atherosclerosis, n (%) | 3 (16%) | 20 (20%) |
| Stroke/neurological disorder, n (%) | 3 (16%) | 25 (25%) |
| Renal failure, n (%) | 0 (0%) | 11 (11%) |
| Atrial fibrillation, n (%) | 5 (28%) | 40 (41%) |
| Immunosuppression, n (%) | 1 (5%) | 4 (4%) |
| Aortic valve disease | ||
| Aortic regurgitation, n (%) | 17 (94%) | 72 (73%) |
| Aortic stenosis, n (%) | 0 | 8 (8%) |
| Mixed aortic valve disease, n (%) | 0 | 3 (3%) |
| No aortic valve disease, n (%) | 1 (5%) | 16 (16%) |
Genetic screening was performed in all patients. Marfan syndrome was confirmed in 14 patients, Ehlers–Danlos syndrome in three patients, and Loyes–Dietz syndrome in one patient.
In all patients, TAFA developed after previous cardiovascular surgery. The indications for the initial aortic operation were either aortic dissection (72% in the CTD cohort and 65% in the non-CTD cohort) or aortic aneurysm (28% and 35%, respectively). Two patients with CTD and three without CTD had undergone their primary surgeries at other cardiovascular centers. In the CTD cohort, the most common procedures preceding TAFA development were the Bentall procedure (88%) and aortic valve resuspension with ascending aorta replacement (12%). The Bentall procedure was performed with direct coronary artery reimplantation using a continuous running suture. No aortic arch procedures were performed in the CTD cohort.
In the CTD cohort, the mean cardiopulmonary bypass time during aortic surgery was 174 ± 56 min, the mean aortic clamping time was 112 ± 32 min, and the mean circulatory arrest time was 16 ± 27 min. A proximal suture was stabilized with a continuous running suture reinforced with PTFE circumferential felt strip in two patients, and the distal suture was stabilized in the same manner in seven patients. Biological glue (Bioglue, Tisseal, GRF glue) was used in all cases.
Surgical re-exploration was necessary in two patients. No wound infections occurred. Four patients had undergone multiple surgeries before TAFA developed. Postoperatively, 17 patients were prescribed anticoagulation and one patient antiplatelet therapy; overall, anticoagulation after surgery was more frequently indicated than either antiplatelet therapy or no therapy in both cohorts. Peri- and postprocedural characteristics of the primary surgeries preceding TAFA development in patients with and without CTDs are presented in Table 2.
Peri- and postprocedural characteristics of primary surgery before TAFA development
| Variable | Patients with CTD | Patients without CTD |
|---|---|---|
| Duration of cardiopulmonary bypass, min, mean ± s.d. | 174 ± 56 | 182 ± 72 |
| Cross-clamp time, min, mean ± s.d. | 112 ± 32 | 112 ± 35 |
| Duration of circulatory arrest, min, mean ± s.d. | 16 ± 27 | 20 ± 28 |
| Proximal suture with PTFE circumferential felt strip, n (%) | 2 (11%) | 36 (37%) |
| Distal suture with PTFE circumferential felt strip, n (%) | 7 (39%) | 49 (50%) |
| Use of biological glue, n (%) | 18 (100%) | 94 (96%) |
| Surgical re-exploration, n (%) | 2 (11%) | 25 (25%) |
| Wound infection, n (%) | 0 (0%) | 9 (9%) |
| Multiple surgeries until TAFA development, n (%) | 4 (22%) | 8 (8%) |
| Antiplatelet therapy after surgery, n (%) | 1 (5%) | 26 (26%) |
| Anticoagulation after surgery, n (%) | 17 (94%) | 59 (60%) |
In the CTD cohort, the median interval between the primary operation and lesion detection was 6.2 ± 5.9 years, and the median interval between lesion detection and reintervention was 1.5 ± 2.1 years. The mean follow-up duration was 13.9 ± 21.5 years. The mean TAFA diameter was 50 ± 28 mm. In the cohort without CTD, these parameters were not significantly different. The median interval between the primary operation and lesion detection was 5.9 ± 6.2 years, and the median interval between lesion detection and reintervention was 1.6 ± 2.27 years. The mean follow-up duration was 12.9 ± 20.3 years. The mean TAFA diameter was 47 ± 27 mm.
The majority of the patients were asymptomatic (78% in the cohort with CTD and 85% in the cohort without CTD). Symptomatic patients with CTD presented with dyspnea (11%), chest pain (5.5%), or superior vena cava syndrome (5.5%). In patients without CTD, the most frequent symptoms were combinations of dyspnea, chest pain, palpitation, hoarseness, vertigo, or manifestations of low cardiac output syndrome.
TAFA was diagnosed by CT (Figure 1) and completed with an echocardiogram to evaluate every case correctly.
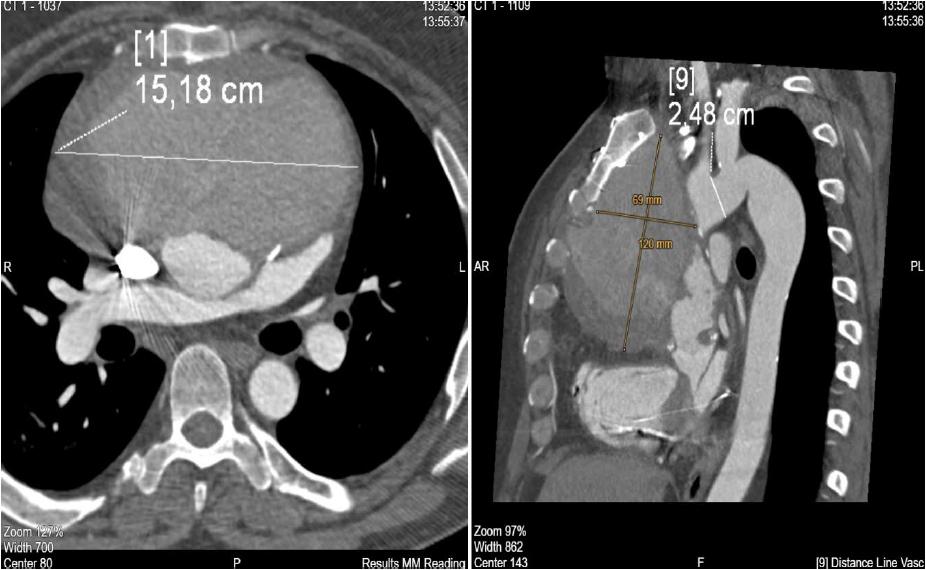
CT scan of aortic pseudoaneurysm.
In the CTD cohort, a single disruption site was identified in 12 patients (67%), two disruption sites in five patients (28%), and three disruption sites in one patient (5%). The most frequent locations were coronary artery reimplantation sites (left in 10 patients, right in 5 patients), followed by the distal anastomosis in eight patients, the proximal anastomosis in one patient, and another localization between the left carotid artery and the left subclavian artery in one patient.
In the cohort without CTD, one disruption site was present in 68 patients (69%), two sites in 25 patients (26%), and three sites in 5 patients (5%). The most common locations were the proximal anastomosis (44 patients), distal anastomosis (41 patients), coronary artery reimplantation sites (left in 17 patients, right in 21 patients), and other localizations such as central anastomosis of the aortocoronary bypass and Valsalva sinuses in seven patients.
A low-density lesion encircling the aortic prosthesis on the CT scan was present in 66% of patients with CTD and 81% of patients without CTD. This finding may be considered a negative prognostic factor and may warrant closer follow-up. A lesion of up to 10 mm observed in 39% of patients with CTD and 36% of those without CTD. A lesion greater than 10 mm was observed in 27% of patients with CTD and 45% of those without CTD on the first postoperative CT scan and persisted on subsequent scans. In the CTD cohort, lesion presence could not be confirmed in 17% of patients because surgery and CT scans were performed before digitalization and data archiving. No lesion was observed in another 17%. In the non-CTD cohort, lesion presence could not be confirmed in 12% of patients because surgery and CT scans were performed before digitalization and data archiving. TAFA development was already visible on the first postoperative CT scan in 4%, and no lesion was observed in 3% of patients.
The Kaplan–Meier method and the log-rank test were used to calculate and compare survival estimates for patients with aortic aneurysms and aortic dissections. In the CTD cohort, 1-year survival was 89% (100% for aortic aneurysm and 85% for aortic dissection). The 1-year and 10-year survival did not change, all patients survived. The differences in survival rates between patients with aortic aneurysm and aortic dissection were not statistically significant (p = 0.21).
In the cohort without CTD, 1-year survival was 98% (97% for aortic aneurysm and 98% for aortic dissection), 5-year survival was 87% (91% for aortic aneurysm and 85% for aortic dissection) and 10-year survival was 68% (72% for aortic aneurysm and 65% for aortic dissection). The differences in survival rates between patients with aortic aneurysm and aortic dissection were not statistically significant (p = 0.13) (Figures 2–4).
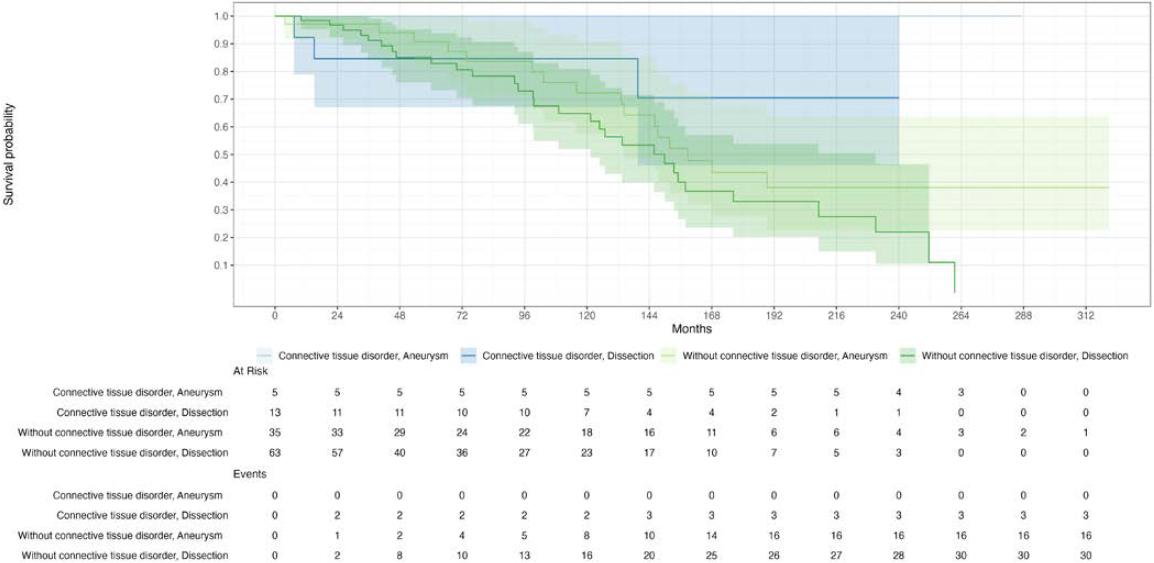
Kaplan–Meier analysis of survival of patients with TAFA (with CTD vs. without CTD)
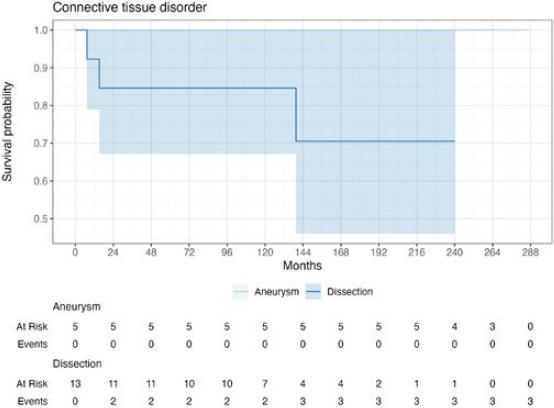
Kaplan–Meier analysis of survival of patients with TAFA and CTD (aortic aneurysm, dissection)
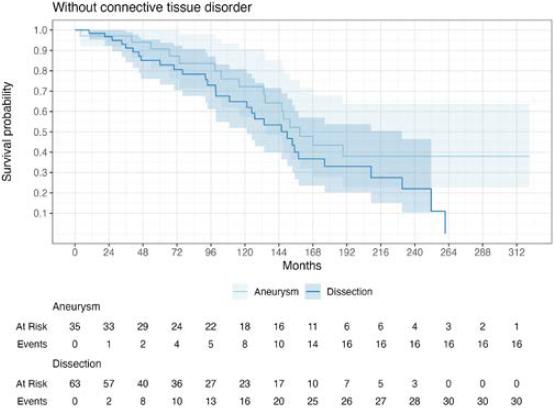
Kaplan–Meier analysis of survival of patients with TAFA and without CTD (aortic aneurysm, dissection)
Ten patients (56%) with CTD and 45 patients (46%) without CTD were indicated for reintervention. In the CTD cohort, open reoperation was performed in five cases, a combination of reoperation and endoluminal graft implantation in one case, open reoperation with occluder implantation in one case, and open reoperation with both endoluminal graft and occluder implantation in two cases. Only one patient underwent isolated endoluminal graft implantation. Eight patients declined reintervention or were deemed unsuitable for a redo procedure but were followed in the surveillance program.
In the cohort without CTD, 32 patients underwent open surgical reoperation, a combination of reoperation and occluder implantation was performed in four patients, and a combination of reoperation and endoluminal graft implantation was performed in three patients. Four patients received isolated occluder implantation, one patient underwent isolated endoluminal graft implantation, and one patient underwent coil embolization. The remaining patients either declined reintervention or were deemed unsuitable for invasive treatment.
During reoperation, all patients were monitored with transesophageal echocardiography, and a median sternotomy was performed in every case. In the CTD cohort, arterial cannulation was achieved via the aorta in five patients, the femoral artery in two patients, and the axillary or subclavian artery in two patients. Venous cannulation was performed through the right atrium in five patients, the femoral vein in two patients, and the superior and inferior vena cava in two patients. In the cohort without CTD, arterial cannulation was performed through the femoral artery in 17 patients, the axillary or subclavian artery in 11 patients, the ascending aorta in seven patients, and the brachiocephalic trunk in one patient. Venous cannulation was achieved via the femoral vein in 17 patients, the right atrium in 16 patients, and the venae cavae in three patients.
Cardiopulmonary bypass was initiated before resternotomy in two patients with CTD and 9 patients without CTD due to the gigantic size of the aortic pseudoaneurysm.
In the CTD cohort, the aortic pseudoaneurysm was closed primarily with a suture in four patients with small defects. For larger defects, aortic repair was performed with interrupted pledget-supported sutures in one patient, whereas replacement with a tube graft was necessary in three patients. One patient underwent a combined procedure consisting of debranching and endoluminal graft implantation.
In the cohort without CTD, the aortic pseudoaneurysm was closed primarily with a suture in five patients and interrupted pledget-supported sutures in 14 patients. Replacement with a tube graft was performed in 11 patients. In the remaining cases, the exact type of repair could not be determined because the surgical protocols form earlier years were no longer available.
The coronary ostia were mobilized from the surrounding aortic tissue, and the coronary buttons were directly reimplanted in five patients with CTD and nine patients without CTD. In seven patients without CTD, coronary button reimplantation was reinforced using a saphenous vein. Concomitant procedures in the CTD cohort included aortic valve replacement in one patient and multiple combined procedures in two patients. In the non-CTD cohort, concomitant surgery was performed in six patients, and multiple combined procedures were performed in two patients.
Periprocedural complications in patients with CTD included profuse hemorrhage in one case during resternotomy due to inadvertent opening of the TAFA, and in another case during adhesiolysis. One patient experienced a postoperative neurological deficit. Secondary recurrence of TAFA occurred in four patients (22%): in one patient at the same disruption site, and in three patients at new sites. The mean time to recurrence was 4.1 ± 4.0 years.
Periprocedural complications were also observed in patients without CTD. Bleeding occurred in three patients during resternotomy, in two patients during adhesiolysis, and in five patients postoperatively. Postprocedural complications included stroke in two patients, severe neurological deficit in two patients, myocardial infarction in two patients, atrioventricular dissociation in one patient, and multiorgan failure in two patients. Secondary recurrence of TAFA occurred in 16 patients (16%): in nine patients, recurrence developed at the same disruption site, while in seven patients it developed at a different site. The mean time to recurrence was 3.1 ± 3.4 years.
The cause of death was determined by reviewing clinical records and death certificates. Operative mortality in patients with CTD was 11.1%. Two patients died of massive intraoperative hemorrhage. All patients managed conservatively survived, except for one who died a week before the scheduled surgery. Operative mortality in patients without CTD was 5.1%. Three patients died of massive hemorrhage, one of multiorgan failure, and another of severe neurological dysfunction.
Aortic pseudoaneurysms result from transmural disruption of at least one layer of the aortic wall, with extravasation of blood into the mediastinum. The leak is contained by the remaining vascular layers or by surrounding mediastinal structures.
Although many studies have described CTD as a risk factor for aortic aneurysms, their role in the development and management of aortic pseudoaneurysms is less well established.1 In this study, all patients underwent genetic screening, and a CTD was confirmed in 18 of the 116 patients (16%). A negative genetic screening result does not exclude the presence of a hereditary disease; rather, it reflects the current limitations in diagnostic methods and scientific understanding. We evaluated several known factors6,9 that may influence TAFA development and compared these characteristics between patients with and without CTD.
Hypertension and atherosclerotic disease are well-known predisposing factors for TAFA formation,3 and this was confirmed in our patients. Two additional risks were observed: aortic regurgitation and atrial fibrillation. The majority of patients with CTD were female (61%), whereas most patients without CTD were male (71%). No other significant differences in preoperative demographic characteristics were identified.
TAFA is a rare but life-threatening complication of aortic surgery or trauma.3 In all patients in our cohort, TAFA developed after previous cardiovascular surgery. The most frequent indication for primary aortic surgery was aortic dissection in both groups. We evaluated the peri- and postprocedural characteristics of the primary surgery preceding TAFA development. Cardiopulmonary bypass duration, cross-clamp time, and circulatory arrest were very similar between the two cohorts. Interestingly, PTFE circumferential felt strips were used more frequently in patients without CTD, both at proximal and distal anastomoses. In most operations, biological glue was used, which is a known risk factor for wall necrosis,6 although this association remains debated by some authors.10
The mean TAFA diameter was similar in both groups. The development of aortic pseudoaneurysms is often asymptomatic,4 and their evolution is unpredictable; they may progressively expand or compress and invade the surrounding structures. In published case series, the most frequent symptoms were chest pain caused by compression of surrounding structures, aortic stretching, or cardiac ischemia.11 When TAFA caused bronchial compression or when heart failure developed, patients typically presented with dyspnea. Heart failure was related to valvular regurgitation, compression of surrounding tissues, or cardiac compression. Compression of recurrent laryngeal nerve resulted in hoarseness.12 These literature findings are consistent with our observations in both cohorts.
Aortic pseudoaneurysms occur most commonly at anastomotic suture lines, coronary reimplantation sites, or aortotomy suture lines. They are more likely to form just behind the suture lines in the native aorta, which is more elastic compared to stiff segments of the anastomosis and prosthetic graft.5 In our study, the most frequent disruption sites were coronary artery reimplantation sites in patients with CTD, and proximal and distal anastomoses in patients without CTD.
Although 1-year survival was higher in the cohort without CTD (98%) than in the cohort with CTD (89%), 10-year survival was higher in patients with CTD (89%) compared to those without CTD (68%). The differences in survival rates between patients with aortic aneurysms and aortic dissection were not statistically significant in either group.
Accurate preoperative assessment of TAFA characteristics using CT and echocardiography is essential. Patients may be candidates for surgical reoperation, endoluminal graft implantation, occluder implantation, or coil embolization, whereas conservative treatment is reserved for small, stable TAFAs or for patients at unacceptable operative risk.13 As the TAFA diameter increases, wall tension rises for any given intraluminal pressure. Therefore, reintervention should be performed before symptoms develop.14 In both cohorts, most patients were indicated for open surgery, which remains the gold standard, with only a minority treated by endovascular approaches. Several surgical and endovascular techniques have advanced over time. Anastomotic technique is a key factor in TAFA development both in patients with or without CTD.15 In our cohort, continuous sutures were most commonly used in patients with CTD, whereas interrupted pledget-supported sutures were used primarily in those without CTD. After surgical reoperation, secondary TAFA recurrence was lower in patients without CTD (16% vs. 22%); however, when recurrence did occur, it appeared sooner in this group than in patients with CTD. Ultimately, the optimal treatment strategy must be individually tailored to minimize perioperative complications.6
Reported operative mortality varies from 5% to 40%,2,16 which aligns with our findings: operative mortality was 11.1% in patients with CTD and 5.1% in those without CTD.
This limited sample size significantly restricts the generalizability and statistical power of this study’s findings. To draw more robust conclusions about the clinical characteristics and outcomes of patients with TAFA associated with CTDs, a larger cohort would be necessary, which is a challenging task given the rarity of the disease.
Our aim was to establish whether a CTD is a risk factor for the development of thoracic aortic false aneurysms. Two cohorts of patients, with and without CTD, were evaluated and compared. The most significant differences were:
Although the 1-year survival was higher among patients without CTD (98%) than in those with CTD (89%), at 10 years, survival was higher in patients with CTD (89%) compared to those without CTD (68%).
After surgical reoperation, secondary TAFA recurrence was lower in patients without CTD (16% vs. 22%). Nonetheless, when recurrence did occur, it appeared sooner among patients without CTD.
Operative mortality was 11.1% in patients with CTD and 5.1% in those without CTD.