Previously described as ‘allergic angina’ or ‘allergic myocardial infarction’, Kounis syndrome is a unique clinical entity that links allergic reactions to acute coronary syndromes, highlighting how the cardiovascular system can be unexpectedly affected by an inappropriate immune response.1 Kounis syndrome represents a rare cause of acute coronary syndrome, triggered by a constellation of inflammatory cell interactions that precipitate hypersensitivity, anaphylactic, or anaphylactoid reactions.2,3 Although the estimated annual prevalence of anaphylactic reactions with cardiovascular involvement is low (0.0079–0.0096%), an American study reported a 1.1% prevalence of Kounis syndrome among patients hospitalized for allergic and anaphylactic reactions, with a 7% inpatient mortality rate.3,4
Based on the status of the epicardial coronary arteries, three distinct variants of Kounis syndrome have been described in the literature. Type I involves coronary vasospasm in the absence of pre-existing coronary atheromatous disease, triggered by allergic reactions. Type II occurs in patients with known coronary artery disease, in whom hypersensitivity reactions precipitate vasospasm or plaque rupture. Type III manifests as stent thrombosis or restenosis secondary to an allergen response.5 Because recent evidence suggests that in-stent restenosis might also be caused by metal allergy from drug-eluting stents, Biteker et al. proposed a further subdivision of type III: type IIIa, stent thrombosis triggered by allergy, and type IIIb, stent restenosis due to allergen response.6 More recently, a type IV variant has also been reported, describing allergic reactions leading to coronary artery bypass graft thrombosis.7
Despite being a rare medical entity, with just over 200 cases of Kounis syndrome reported in the literature, increasing awareness of this condition is essential due to its diagnostic challenges, particularly in cases with mild or absent allergic symptoms. Moreover, even when correctly diagnosed, recurrence remains possible, especially if triggering factors persist.8,9 The following case describes an uncommon clinical presentation of Kounis syndrome, notable for the absence of signs or symptoms of an allergic response at onset. A comprehensive literature search was conducted in PubMed, Scopus, and Web of Science using the keywords ‘acute coronary syndrome’, ‘chronic spontaneous urticaria’, ‘idiopathic anaphylaxis’, and ‘Kounis syndrome’. Specific case reports and case series relevant to these topics were also reviewed.
A 55-year-old female patient, a non-smoker, with a history of well-controlled hypertension on metoprolol, unmedicated autoimmune thyroiditis, and recurrent allergic complaints, presented to the emergency department with typical anginal pain. The pain began about 1 hour before admission, awaking her from sleep, and was accompanied by nausea and vomiting. She reported no prior episodes of chest pain.
On admission, clinical examination was unremarkable. Blood pressure was 139/102 mmHg, and BMI was 25.1 kg/m2. Electrocardiography revealed pathognomonic ST-segment elevation in the anterior and lateral leads (Figure 1), and elevated myocardial necrosis markers confirmed ST-elevation myocardial infarction. Transthoracic echocardiography showed a nondilated left ventricle with hypokinesia of the apical half of the interventricular septum, apex, and apical half of the anterior wall, resulting in mildly reduced left ventricular ejection fraction (LVEF 40%). The right ventricle had preserved function, both atria were nondilated, and no hemodynamically significant valvopathies were identified.

Electrocardiogram on presentation showing QS wave in V1–V3, ST elevation of 4 mm in leads V3–V4, 1–2 mm in leads V2, V5–V6, and 0.5 mm in leads DI and aVL.
Emergency coronary angiography revealed no significant epicardial coronary stenoses, consistent with myocardial infarction with non-obstructive coronary arteries (MINOCA), with coronary vasospasm considered the likely mechanism. Consequently, beta-blocker therapy was switched to a non-dihydropyridine calcium channel blocker. Tests for SARS-CoV-2 and influenza A/B were negative.
During the first hours of hospitalization, the patient developed lower lip edema, apparently following angiotensin-converting enzyme inhibitor administration, which was discontinued. She also developed pruritic erythematous plaques, which improved with intravenous hydrocortisone, antihistamines, and topical corticosteroids. Given her clinical background, the allergologist retrospectively suspected recurrent chronic spontaneous urticaria, recurrent facial angioedema, mast cell activation syndrome, and Kounis syndrome type I.
Initially, continuation of antiplatelet therapy with aspirin was recommended. However, due to the absence of coronary atherosclerotic lesions and worsening cutaneous reactions, aspirin was discontinued and replaced with single antiplatelet therapy using clopidogrel. At discharge, echocardiography showed partial recovery of LV systolic function, with LVEF 45–50% and residual hypokinesia of the apical third of the interventricular septum.
The discharge treatment included clopidogrel 75 mg o.d., rilmenidine 1 mg o.d., diltiazem 90 mg b.i.d., nitroglycerin 2.6 mg b.i.d., desloratadine 5 mg b.i.d., and pantoprazole 40 mg o.d. She remained under allergy specialist care; although no specific trigger was identified, total serum IgE was elevated at 473 U/L (normal <100 U/L). According to the chronic spontaneous urticaria protocol, omalizumab was initiated after one month of high-dose oral antihistamines (desloratadine 5 mg q.i.d.).
The patient continues monthly follow-up for monoclonal antibody therapy and, four years after the acute coronary event, remains clinically stable, without recurrence of angina or urticaria. No changes to her treatment regimen have been required, although a mildly impaired LV function persists.
Referral to the cardiology department was prompted by the presence of ST-segment elevation suggestive of acute coronary syndrome. Subsequent coronary angiography revealed non-obstructive arteries, establishing the diagnosis of myocardial infarction with non-obstructive coronary arteries (MINOCA). MINOCA is a unifying term that encompasses a wide spectrum of pathophysiological mechanisms of both coronary and non-coronary origin.10 The most common coronary causes include coronary plaque disruption, coronary artery spasms, spontaneous coronary artery dissection, coronary microvascular dysfunction, and coronary thromboembolism.11 Although not the predominant mechanism, studies report that 10–46% of patients with MINOCA have inducible coronary spasm at angiography.11
In many cases, coronary vasospasm involved in MINOCA cannot be identified during emergency angiography for STEMI, and provocative testing with acetylcholine or ergonovine may be required.12 However, due to limited availability, such testing was not performed in this case. Following a broader evaluation of the patient’s atopic background, the allergologist favored a diagnosis of Kounis syndrome type I, even in the absence of a clearly identified allergen.
Kounis syndrome type I involves coronary artery spasm caused by histamines and leukotrienes released during mast cell degranulation (Figure 2).13,14 Histamine induces vasoconstriction mainly through H1-receptor-mediated smooth muscle contraction, whereas leukotrienes promote vasoconstriction by modulating the lipoxygenase pathway.14 Therefore, it was considered highly likely that the ischemic event was caused by an allergic vasospasm. As with other complex allergic conditions, however, identifying the exact trigger proved challenging in the context of multiple possible environmental exposures.
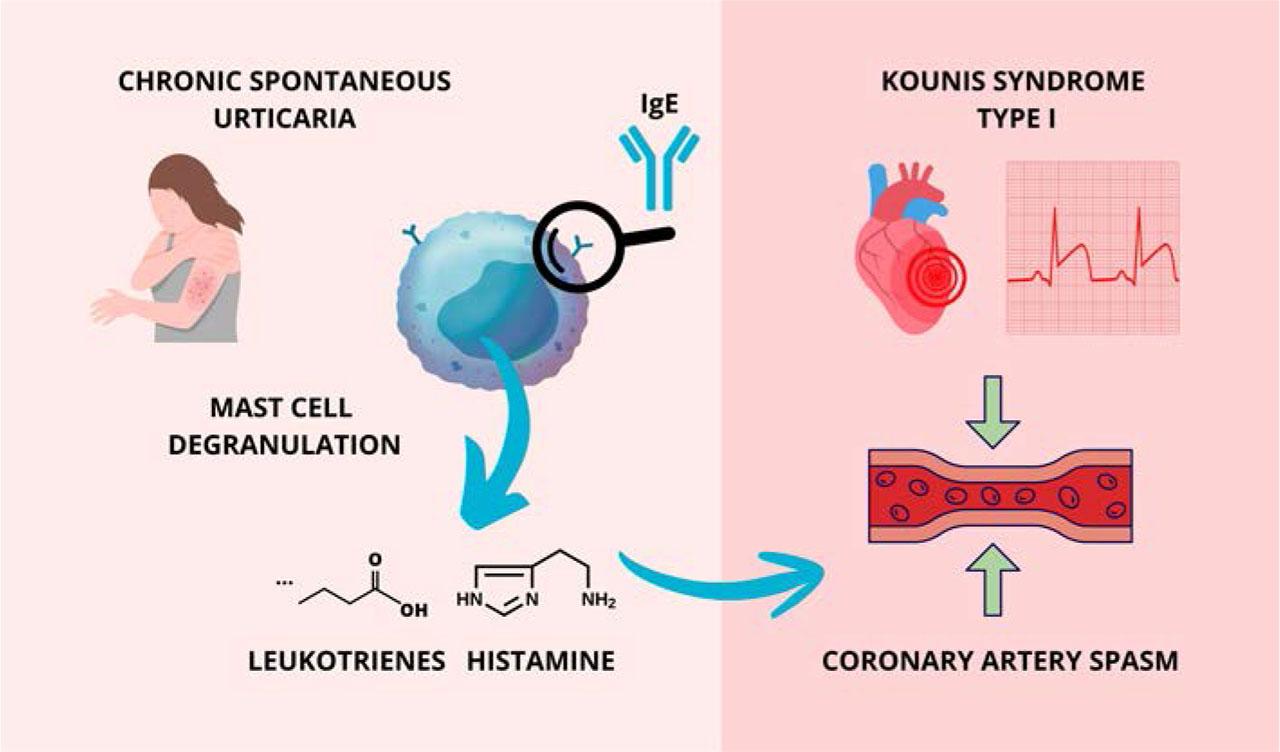
Pathophysiological link between chronic spontaneous urticaria and Kounis syndrome type I.
We previously emphasized that one of the particularities of this case is the absence of a clearly identifiable allergic trigger. As no discernible trigger was found during extensive evaluation, the presentation could initially have been misinterpreted as an anaphylactic reaction to an unknown allergen. Idiopathic anaphylaxis represents a phenotype of severe hypersensitivity reactions with multiorgan involvement in the absence of identifiable triggers and is associated with dysregulated mast cell activation.15 A few cases of idiopathic anaphylaxis–associated Kounis syndrome type I have been described in the literature.16,17 The main features of two such cases are summarized in Table 1 and Table 2.
Kounis syndrome associated with idiopathic anaphylaxis
| Sandhu et al., 2017 | Keber et al., 2017 | |
|---|---|---|
| Country | USA | Slovenia |
| Patient profile | 65, female, with a history of malignant idiopathic anaphylaxis | 48, male |
| Trigger | Idiopathic anaphylaxis | Idiopathic anaphylaxis |
| Allergic symptoms | Present (facial flushing) | Present (skin changes, dyspnea) |
| Presentation | Chest pain | Chest pain, dyspnea, nausea |
| Coronary artery disease | No, confirmed by computed tomography angiography | No, confirmed by coronary angiography |
| Biomarkers | Troponin rise | Troponin rise, elevated tryptase during attacks |
| Electrocardiogram | NSTEMI | STEMI |
| Therapeutic management | Loratadine, famotidine, corticosteroids | Antihistamines |
Kounis syndrome associated with chronic spontaneous urticaria
| Erxun et al., 2016 | Brancaccio et al., 2024 | |
|---|---|---|
| Country | China | Italy |
| Patient profile | 31, female, chronic autoimmune urticaria | 47, female, chronic spontaneous urticaria |
| Trigger | No apparent trigger | No apparent trigger |
| Allergic symptoms | Erythema and wheals on trunk and limbs | Edema and wheals on lips and eyelids |
| Presentation | Chest pain, diaphoresis, palpitations | Chest pain |
| Coronary artery disease | No, confirmed by coronary angiography | No, confirmed by coronary angiography |
| Biomarkers | Troponin rise, serum anti-high affinity IgE receptor antibody test positive | Troponin rise, elevated tryptase during attacks |
| Electrocardiogram | STEMI | STEMI |
| Therapeutic management | Cetirizine, methylprednisolone and then prednisone, azathioprine | Cetirizine, prednisone, omalizumab |
Key diagnostic elements that may help clarify Kounis syndrome include the onset of allergic manifestations with acute chest pain or dyspnea following an allergic insult, electrocardiographic evidence of acute myocardial infarction, transient left ventricular hypokinesia, and recovery of left ventricular function within four weeks of the acute coronary event.18 In Kounis syndrome associated with idiopathic anaphylaxis, elevated serum histamine, tryptase, cardiac enzymes, and troponins may serve as valuable diagnostic indicators.17 Histamine peaks approximately 5 min after release and returns to baseline within 30 min, making its measurement rarely feasible in clinical practice.18 Tryptase, a serine protease secreted exclusively during mast cell activation, has a half-life of about 90 min; if not measured within 30–120 min after symptom onset, its diagnostic value is limited.19
In our case, the patient did not present with allergic symptoms immediately prior to the onset of chest pain, and suspicion of Kounis syndrome was raised more than 48 h after admission. Therefore, histamine and tryptase were not measured. However, during flare-ups of her chronic spontaneous urticaria, serum histamine levels may have been transiently elevated while tryptase remained normal, as increased tryptase levels are typically associated with more extensive mast cell degranulation, such as in anaphylaxis.20
Following clinical assessment, the patient was diagnosed with chronic spontaneous urticaria, a mast-cell mediated disease characterized by recurrent episodes of transient wheals, angioedema, or both, persisting for over 6 weeks and sometimes associated with systemic symptoms, reflecting its multisystemic nature.21 Chronic autoimmune urticaria is a subtype of chronic spontaneous urticaria, characterized by the presence of functional autoantibodies targeting IgE or high-affinity IgE receptors, leading to chronic mast cell activation and urticarial symptoms.20 A few case reports have documented Kounis syndrome associated with chronic spontaneous urticaria.19,22 A common feature in these cases, including the present one, is the absence of an identifiable trigger, underscoring the diagnostic challenge.
Omalizumab, a humanized anti-IgE antibody, has proven effective against urticarial symptoms in chronic spontaneous urticaria, with over 50% of patients reporting improvement within the first week of therapy.21 It is approved at doses of 150 or 300 mg every four weeks; however, current guidelines recommend an initial dose of 300 mg every four weeks, with the option of uptitration to 600 mg every two weeks in refractory cases.23,24 Omalizumab binds circulating IgE, preventing its attachment to mast cell receptors, thereby suppressing mast cell responsiveness and downregulating IgE receptors.23 The ASTERIA I, ASTERIA II, and GLACIAL trials confirmed symptom reduction after omalizumab initiation, with maximum benefit observed by week 12.25 In chronic spontaneous urticaria–associated Kounis syndrome refractory to antihistamines and corticosteroids, omalizumab has also been effective in reducing recurrence.19
Paradoxically, anti-allergic therapies such as omalizumab have been associated with anaphylaxis or anaphylactoid reactions, an important consideration in Kounis syndrome. Although rare, anaphylaxis occurs in approximately 0.2% of cases, usually within the first 2 h after injection.26 Nonetheless, when administered in an appropriate setting, the overall safety profile of omalizumab remains favorable.26 According to current guidelines, patients with urticaria refractory to omalizumab may be considered for ciclosporin, an immunosuppressant that directly inhibits mast cell mediator release; however, its use is limited by significant adverse effects and it is not recommended as first-line therapy.20
Interestingly, L-type calcium channel blockers, traditionally used for coronary artery spasm, also display anti-allergic properties. Their broader value in Kounis syndrome type I lies in inhibiting extracellular calcium influx, thereby suppressing mast cell activation and alleviating not only the vasospastic component but also the upstream allergic mechanism.27
Another contemporary condition to consider in the differential diagnosis of this case of Kounis syndrome case is SARS-CoV-2 infection. The presented case occurred at the end of September 2021, during the COVID-19 pandemic in Romania. Zhao et al. reported 15 cases of Kounis syndrome following COVID-19 vaccination, noting that it occurred more frequently after the first vaccine dose compared with subsequent doses, and that symptoms typically developed within 2 h post-vaccination.28 However, clinical signs of anaphylaxis may complicate recognition of severe Kounis syndrome in this context, as cardiogenic shock can mask allergic manifestations.29 In addition, SARS-CoV-2 infection itself may directly precipitate Kounis syndrome through mast cell activation and proinflammatory, prothrombotic pathways.30
In the present case, however, the patient had not been vaccinated, and reverse transcription polymerase chain reaction testing for SARS-CoV-2 was negative. Although the precise causative factor remains uncertain and could be the most debated element of this case, what likely had the greatest impact on the patient’s recovery after the acute coronary syndrome was the impairment of left ventricular systolic function.
Improvement in left ventricular ejection fraction dysfunction following an ischemic event in the context of Kounis syndrome is generally expected within a few days of symptom onset, although recovery depends on the severity of the initial reaction.13 In patients with Kounis syndrome type I, who do not develop lasting complications such as malignant arrhythmias or extended ischemic territories, long-term survival and clinical outcomes are typically favorable.31
Despite its generally favorable prognosis, a major concern with Kounis syndrome is the possibility of underdiagnosis. Approximately 6% of patients with acute myocardial infarction undergoing angiography are found to have MINOCA, and one study concluded that up to 50% of these cases are attributable to coronary vasospasm.32 Considering that only a few hundred cases of Kounis syndrome have been reported in the literature, uncertainty remains regarding its correct diagnosis, especially in patients with minimal or absent allergic symptoms. Furthermore, an incomplete diagnosis can lead to incomplete or even inappropriate therapy, as certain standard acute coronary syndrome treatments may themselves act as atopic triggers capable of inducing vasospasm. Another therapeutic challenge lies in the potential for recurrence upon re-exposure to the trigger, which can provoke both allergic reactions and coronary vasospasms. Nevertheless, recurrent Kounis syndrome appears to be relatively uncommon, with most reported cases involving type III presentations.19
We aimed to highlight the importance of reporting Kounis syndrome cases to improve recognition, particularly in patients without prominent allergic manifestations or an identifiable trigger, and especially when associated with chronic spontaneous urticaria. Awareness of Kounis syndrome should extend beyond cardiology to include allergology, emergency medicine, and internal medicine. Because type I Kounis syndrome may be misdiagnosed as acute coronary syndrome without obstructive coronary artery disease, thorough anamnesis and close clinical observation are essential to ensure the correct diagnostic pathway. The continued publication of case reports and the development of dedicated registries will be crucial for refining diagnostic criteria and therapeutic strategies for this rare condition.