
Acute coronary syndrome (ACS) encompasses various clinical symptoms indicative of acute myocardial ischemia. It comprises ST-elevation myocardial infarction (STEMI), non-ST-elevation myocardial infarction (NSTEMI), and unstable angina. STEMI occurs due to complete and prolonged occlusion of an epicardial coronary artery and typically involves coronary plaque rupture, resulting in thrombus formation and subsequent coronary artery occlusion, as defined by specific electrocardiogram (ECG) criteria. NSTEMI typically arises from severe narrowing of coronary arteries, transient occlusion, or microembolization of thrombotic or atheromatous material, and is characterized by elevated cardiac biomarkers without ST elevation on ECG. Diagnosis relies on a combination of history, physical examination, ECG, biochemical markers, and echocardiography. The management of ACS should prioritize prompt diagnosis, risk assessment, and initiation of therapies aimed at restoring coronary blood flow and alleviating myocardial ischemia.1,2 Moreover, noncoronary factors, such as cardiac contusion, myocarditis, or exposure to cardiotoxic agents, may provoke NSTEMI. Additionally, extracardiac factors unrelated to the coronary arteries or myocardium, such as hypotension, hypertension, tachycardia, aortic stenosis, and pulmonary embolism, may contribute to NSTEMI by escalating myocardial oxygen demand beyond the available supply.3,4
Despite intensive therapies and coronary revascularization, acute myocardial infarction remains the primary cause of cardiogenic shock (CS) and is linked with elevated mortality rates.5,6 Some studies have suggested that patients with STEMI have a higher prevalence of CS in the context of AMI-CS.7–9 However, information regarding the prevalence, in-hospital case-fatality, and the long-term prognosis of CS depending on the type of AMI is scarce. Rigorous studies have compared mortality between patients with STEMI and NSTEMI and concluded that STEMI has higher in-hospital death rates, whereas NSTEMI has a worse long-term prognosis.10 Predictors of in-hospital survival in CS described in the literature include older age, previous stroke, increased glucose and creatinine at admission, abnormal coronary flow after percutaneous intervention, and elevated serum lactate.11 Yet, information relative to the prognosis based on the admission ECG pattern is not well established.
Certain studies have indicated a greater occurrence of cardiovascular risk factors among patients with NSTEMI when compared to those with STEMI.12,13 In the CREDO registry,14 it was observed that 62% of patients with NSTEMI had multivessel coronary disease, a finding consistent with a previous multicenter Spanish registry.9 In-hospital death has been strongly associated with suboptimal final coronary perfusion, as noted in several studies.15 Patients with STEMI-CS exhibited approximately 40% higher 30-day case-fatality compared to patients with NSTEMI-CS. However, patients with NSTEMI-CS experienced higher long-term mortality, likely attributed to a higher burden of comorbidities. Consequently, the 5-year all-cause mortality was comparable between the two groups. In terms of clinical characteristics, patients with STEMI-CS presented with larger infarcts and a greater incidence of mechanical complications, whereas patients with NSTEMI-CS had a higher prevalence of comorbidities and multi-vessel involvement.16
The aim of this study was to evaluate the incidence of ventricular arrhythmias and hemodynamic instability in patients with NSTEMI compared to those with STEMI.
This is a single-center retrospective study investigating the incidence of ventricular arrhythmias and hemodynamic instability in patients with NSTEMI compared to those with STEMI.
The study included patients with STEMI and NSTEMI who were admitted between April and July 2021 to the Cardiology Clinic of the Târgu Mureș County Emergency Clinical Hospital and underwent revascularization therapy. A total of 172 patients were included, of which 108 had STEMI and 64 had NSTEMI. Ventricular arrhythmias, classified as either ventricular tachycardia or ventricular fibrillation, were monitored before or after hospital admission. Hemodynamic instability was defined as hypotension accompanied by tachycardia, necessitating intravenous inotropic support before or after hospital admission.
NSTEMI and STEMI were defined according to the standard criteria: STEMI was defined as a new ST-segment elevation of ≥1 mm at the J-point in two or more contiguous leads accompanied by an elevation of troponin levels above the 99th percentile. NSTEMI was defined as a new ST-segment depression of >0.1 mm or T-wave inversion of at least 0.3 mm in more than two contiguous leads accompanied by an elevation of troponin levels above the 99th percentile.
Graph Pad Prism 9.0 software (GraphPad Software) was used for statistical analysis. All data were checked for normality before statistical analysis. The results were expressed as numbers and percentage. Statistical significance, expressed as p, was set at 0.05.
In the study population, a history of acute coronary syndrome had a higher incidence among patients with NSTEMI (Figure 1). However, no statistically significant differences were observed in the baseline characteristics, nor in the incidence of atrial fibrillation, diabetes mellitus, smoking, or arterial hypertension (Table 1).
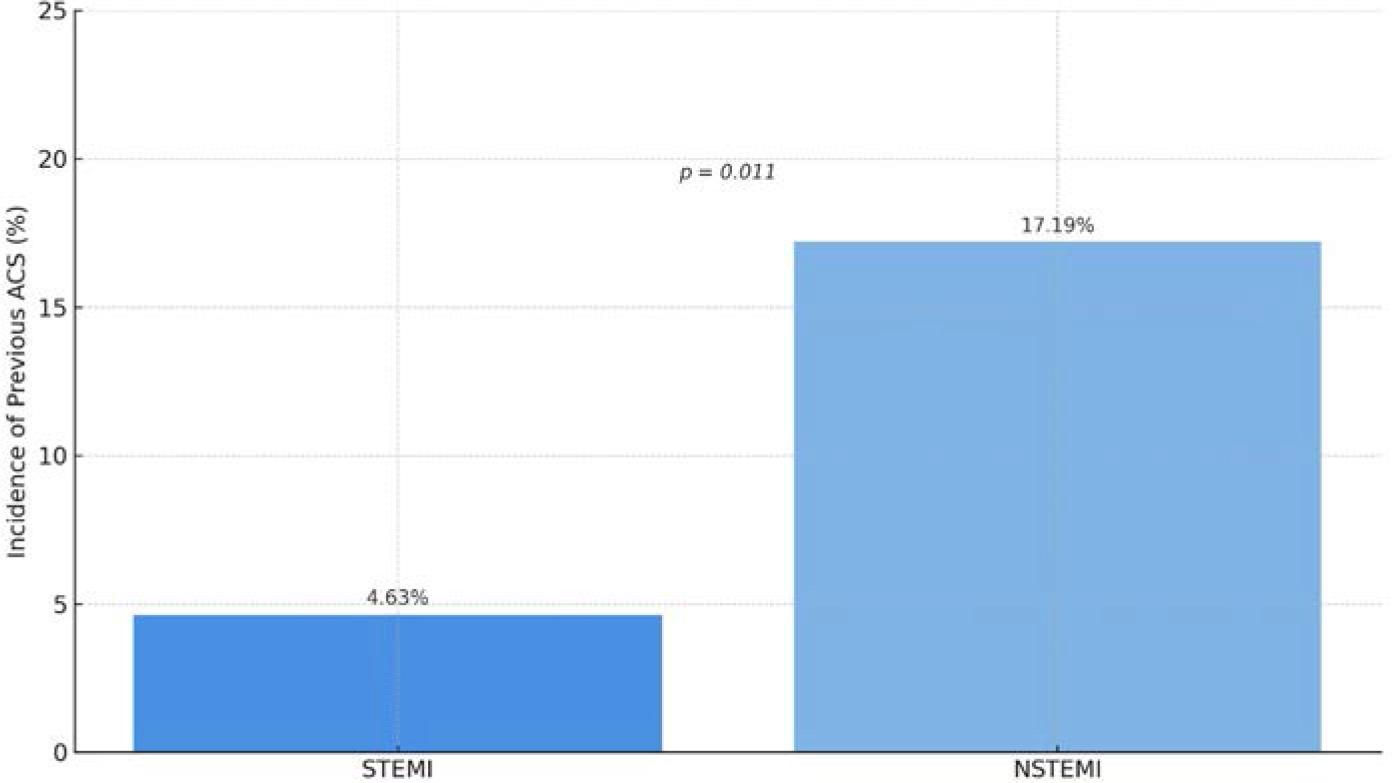
Advanced coronary artery disease, evidenced by a history of ACS, demonstrated a statistically significant higher prevalence in the NSTEMI group.
Baseline characteristics
| Variable | STEMI (n = 108) | NSTEMI (n = 64) | p value |
|---|---|---|---|
| Mean age | 61.5 | 64.03 | 0.19 |
| Male | 80 (74%) | 48 (75%) | >0.99 |
| Previous ACS | 6 (4.63%) | 11 (17.19%) | 0.011 |
| History of atrial fibrillation | 21 (19.44%) | 6 (9.38%) | ns |
| Diabetes mellitus | 26 (24.07%) | 16 (25.00%) | ns |
| Smoker | 44 (40.74%) | 18 (28.13%) | ns |
| Hypertension | 80 (74.07%) | 56 (87.5%) | ns |
| Peak hs-cTnI (ng/ml) | 10,422 ± 15,636 | 5,720 ± 8,272 | ns |
| NTproBNP (pg/ml) | 4,049 ± 6,990 | 2,707 ± 4,380 | ns |
| LVEF (%) | 40.74% | 43.45 | 0.05 |
Values are expressed as absolute values and percentages, respectively. All p values refer to between-group comparisons based on Fisher’s exact test. ns, nonsignificant; hs-cTnI, high-sensitivity cardiac troponin I; LVEF, left ventricular ejection fraction; NTproBNP, N-terminal pro-B-type natriuretic peptide.
The distribution of treated culprit lesions differed significantly between patients with STEMI and NSTEMI (Table 2). In the STEMI group, the most treated artery was the left anterior descending (LAD) artery, accounting for 58.16% of cases, followed by the right coronary artery (RCA) at 40.81%, and the circumflex artery (CX) at 14.28%. Only 2.04% of patients with STEMI had interventions involving the left main (LM) coronary artery. In contrast, among patients with NSTEMI, the LAD remained the most frequently treated vessel (53.7%), followed by the CX (16.66%) and RCA (7.4%), with a notably higher proportion of LM interventions (47.4%). The differences in LM and RCA involvement between groups were statistically significant (p < 0.0001), whereas differences in LAD and CX involvement were not statistically significant (Figure 2). These findings suggest distinct patterns of coronary involvement in STEMI vs. NSTEMI and underscore the higher prevalence of left main disease in the NSTEMI population.
Distribution of treated culprit lesions in patients with STEMI and NSTEMI. Left main artery involvement was significantly higher in NSTEMI patients (47.4% vs. 2.04%; p < 0.0001), whereas RCA lesions were more frequently treated in STEMI (40.81% vs. 7.4%; p < 0.0001). No statistically significant differences were observed for LAD or CX involvement.
The incidence of hemodynamic instability and ventricular arrhythmias, the frequency of PTCA, the distribution of culprit lesions across major coronary arteries with PTCA, and a subanalysis for culprit treated lesions and hemodynamic instability/ventricular arrythmias
| Variable | STEMI (n = 108) | NSTEMI (n = 64) | p value |
|---|---|---|---|
| Treated culprit lesions | |||
| PTCA | 98 | 54 | |
| Left Main | 2 (2.04%) | 4 (47.4%) | <0.0001 |
| LAD | 57 (58.16%) | 29 (53.7%) | ns |
| RCA | 40 (40.81%) | 4 (7.4%) | <0.0001 |
| CX | 14 (14.28%) | 9 (16.66%) | ns |
| Hemodynamic instability | 20 (0.18%) | 7 (10.93%) | 0.005 |
| Ventricular arrhythmias | 13 (12.03%) | 5 (7.81%) | ns |
| Hemodynamic instability | 4,049 ± 6,990 | 2,707 ± 4,380 | ns |
| PTCA - LM | 1 (5%) | 0 | – |
| PTCA - LAD | 8 (40%) | 4 (57.14%) | ns |
| PTCA - RCA | 8 (40%) | 2 (28.15%) | ns |
| PTCA – CX | 3 (15%) | 2 (18.15%) | ns |
| Ventricular arrhythmias | |||
| PTCA – LAD | 6 (46.15%) | 3 (60%) | ns |
| PTCA - RCA | 4 (30.7%) | 0 | – |
| PTCA – CX | 2 (15.38%) | 2 (40%) | 0.0001 |
Values are expressed as absolute values and percentages, respectively. All p values refer to between-group comparisons based on Fisher’s exact test.
Hemodynamic instability was significantly more prevalent among patients with NSTEMI compared to those with STEMI (10.93% vs. 0.18%; p = 0.005; Figure 3).
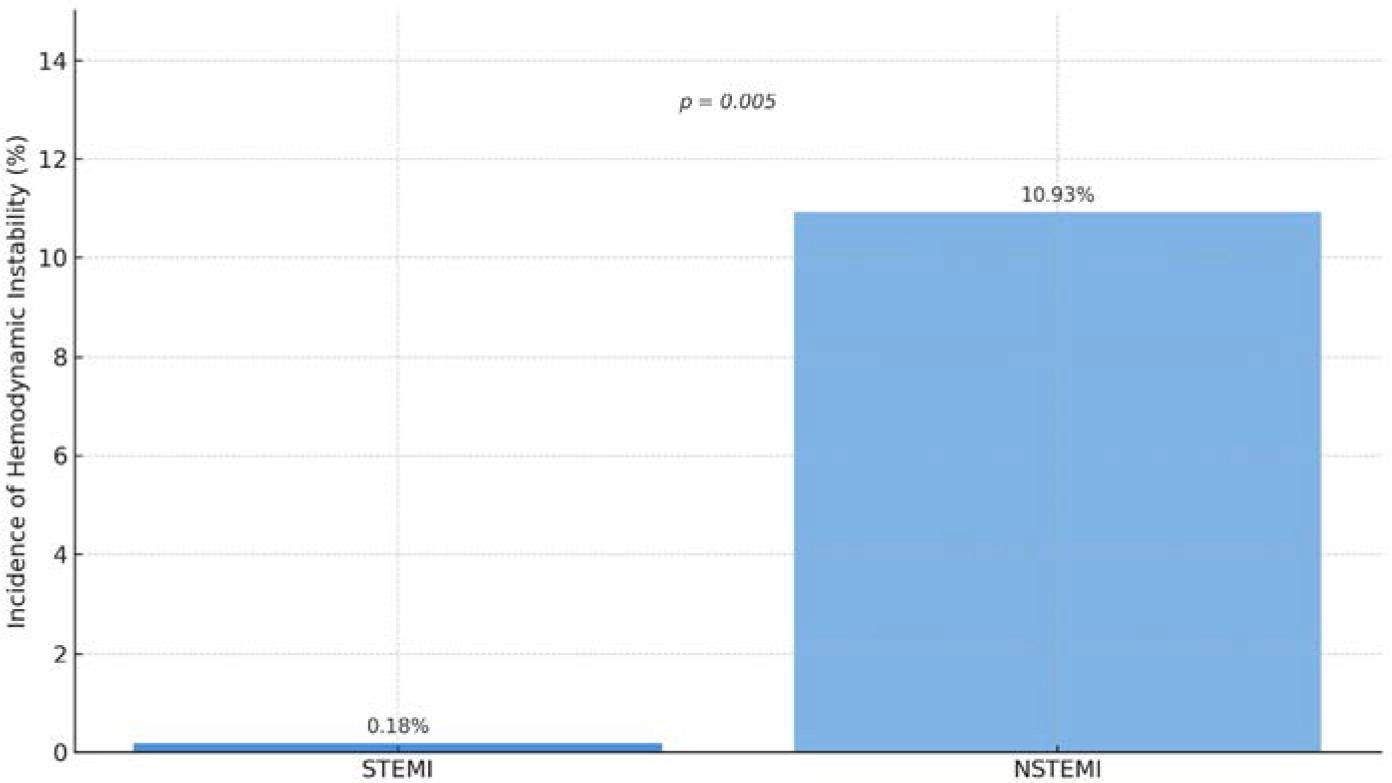
Distribution of hemodynamic instability in patients with STEMI compared to those with NSTEMI. The chart illustrates a significantly higher occurrence of hemodynamic instability in patients with NSTEMI (10.93%) compared to those with STEMI (0.18%), with statistical significance noted (p = 0.005).
We analyzed the distribution of culprit lesions treated by percutaneous transluminal coronary angioplasty (PTCA) among patients who experienced hemodynamic instability. In the STEMI group, hemodynamic instability was most frequently associated with PTCA of the LAD and RCA, each accounting for 40% of cases. A smaller proportion involved the CX (15%) and the LM (5%) arteries. By contrast, among patients with NSTEMI and hemodynamic instability, LAD interventions accounted for 57.14% of cases, followed by CX (18.15%) and RCA (28.15%), with no cases involving the LM. No statistically significant differences were observed between groups for any of the individual vessel distributions. These findings suggest similar patterns of hemodynamic compromise across major coronary territories in both patients with STEMI and NSTEMI.
Ventricular arrhythmias were observed in both patient groups, although the difference was not statistically significant. In the STEMI group, 12.03% of patients (n = 13) experienced ventricular arrhythmias, compared to 7.81% (n = 5) in the NSTEMI group (p = ns). While these findings suggest a numerically higher incidence in STEMI, the lack of statistical significance indicates that ventricular arrhythmias may occur with comparable frequency across both types of myocardial infarction.
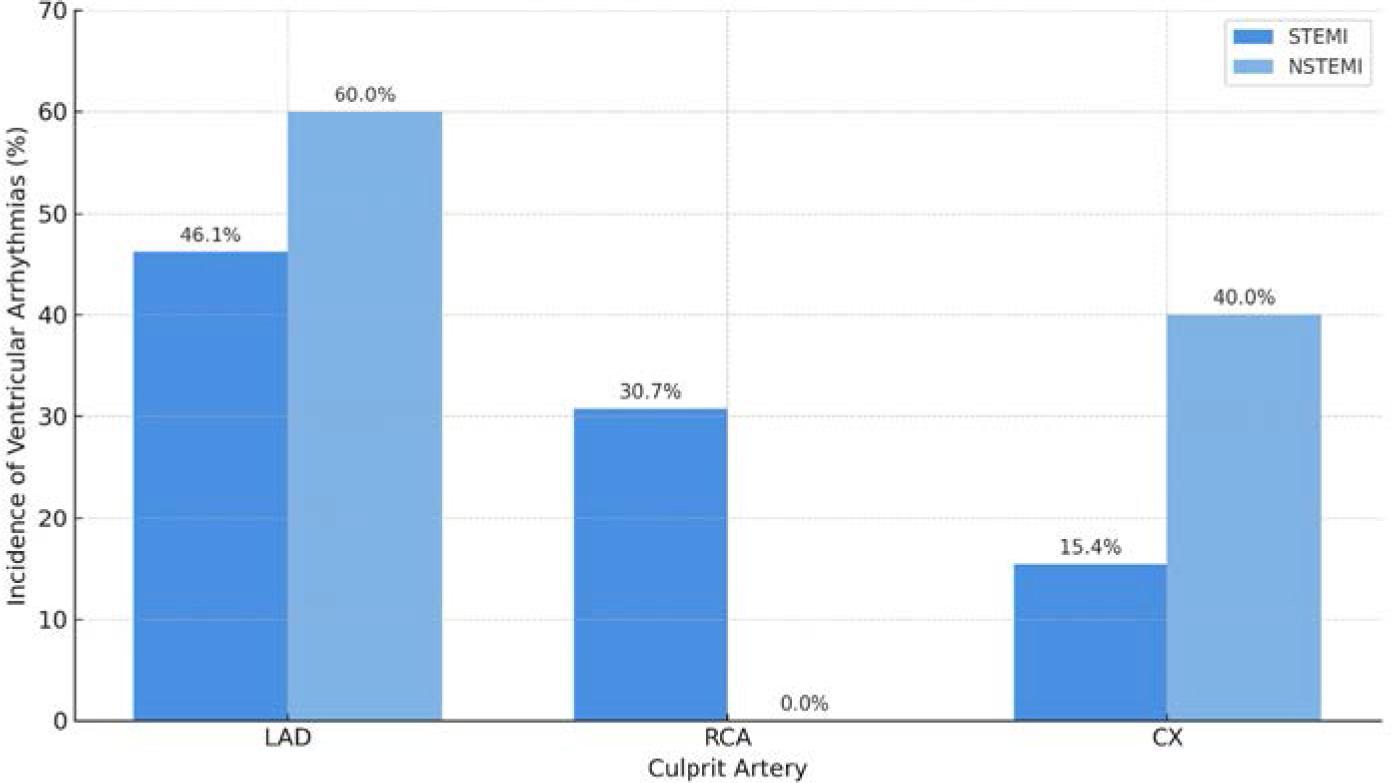
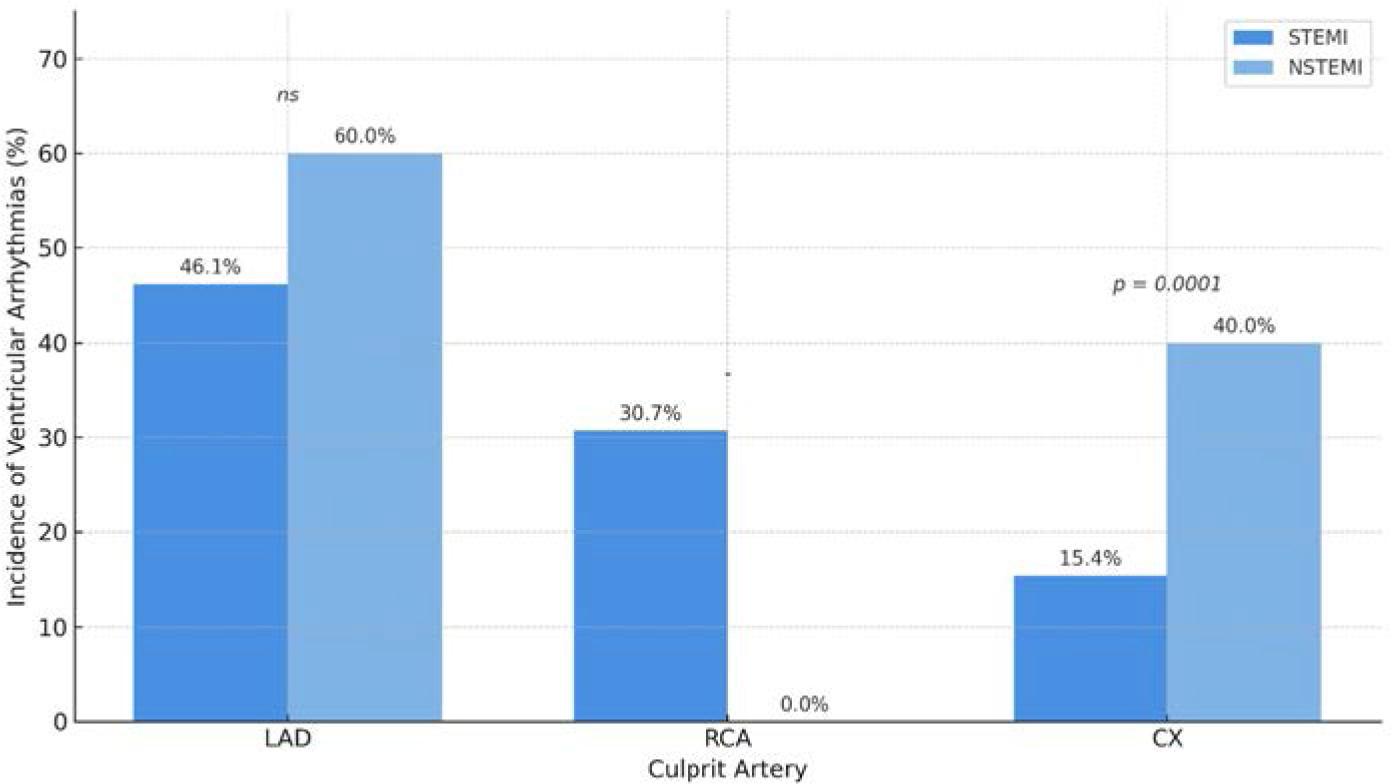
Among patients who developed ventricular arrhythmias, the distribution of angioplasty-targeted vessels revealed notable patterns. In the STEMI group, arrhythmias were most commonly associated with PTCA to the LAD (46.15% of cases), followed by the RCA (30.7%) and the CX (15.38%). In contrast, among patients with NSTEMI and ventricular arrhythmias, the LAD was involved in 60% of cases and the CX in 40%, and no arrhythmias were observed in association with RCA intervention. Notably, ventricular arrhythmias related to CX intervention were significantly more frequent among patients with NSTEMI (p = 0.0001; Figure 4). These findings suggest a potential association between CX involvement and arrhythmic complications in the NSTEMI population, warranting further investigation.
Comparison of ventricular arrhythmias between the two groups. The analysis showed no statistically significant difference in the incidence of hemodynamic instability between patients with NSTEMI and STEMI.
This study provides new evidence of important clinical and angiographic differences between patients presenting with STEMI and those with NSTEMI, particularly with regard to the incidence of hemodynamic instability and ventricular arrhythmias.
A somewhat unexpected finding was the significantly higher incidence of hemodynamic instability in patients with NSTEMI compared to those with STEMI. Although STEMI has traditionally been associated with a greater risk of cardiogenic shock due to larger infarct size and complete coronary occlusion,7,8 recent studies have suggested that patients with NSTEMI often carry a higher burden of comorbidities and multivessel disease, which may predispose them to hemodynamic compromise even in the absence of complete vessel occlusion.12,13 Our results support this view, as patients with NSTEMI in our cohort had a significantly higher prevalence of LM coronary artery involvement (47.4% vs. 2.04%; p < 0.0001), a finding consistent with the CREDO registry and other large observational studies.14
In terms of coronary lesion distribution, patients with STEMI showed a significantly greater incidence of RCA involvement, whereas left main disease was predominantly observed in NSTEMI cases. RCA occlusion has been classically linked with inferior STEMI and often results from acute, complete thrombotic events.15 On the other hand, left main and multivessel disease, more commonly seen in NSTEMI, may reflect chronic atherosclerotic progression and higher baseline cardiovascular risk. These differences align with previous observations that patients with NSTEMI tend to be older and present with more advanced atherosclerosis and higher long-term mortality, despite lower inhospital death rates compared to patients with STEMI.9,11,16
Although the overall incidence of ventricular arrhythmias did not differ significantly between groups, our subanalysis revealed a statistically significant association between ventricular arrhythmias and CX involvement in the NSTEMI group (p = 0.0001). This may be related to the posterior and lateral myocardial territories supplied by the CX, which are less well represented on standard 12-lead ECG, potentially leading to delayed recognition and treatment.15 Previous studies have suggested that CX-related infarctions are frequently underdiagnosed and may carry a higher risk of arrhythmic complications, particularly in NSTEMI.16
These findings challenge the conventional perception that NSTEMI represents a less severe clinical entity than STEMI. Although STEMI typically presents with dramatic ECG changes and abrupt vessel occlusion, patients with NSTEMI may present with subtle clinical signs but carry substantial anatomic and physiological risk due to multivessel or left main involvement. The higher prevalence of previous ACS and reduced left ventricular ejection fraction observed in our NSTEMI cohort further supports the notion that NSTEMI often occurs in the setting of cumulative myocardial injury and chronic ischemia.
In light of these observations, our results underscore the need for thorough hemodynamic and rhythm monitoring in patients with NSTEMI, alongside early coronary angiography and tailored intervention strategies. Risk stratification tools should consider both anatomical lesion complexity and the potential for electrical instability, particularly in patients with CX involvement.
This study provides clear evidence of distinct clinical and angiographic differences between patients with STEMI and NSTEMI. Hemodynamic instability was significantly more common in NSTEMI, whereas RCA involvement predominated in STEMI. Left main disease was notably higher in NSTEMI cases. Although overall arrhythmia rates were similar, ventricular arrhythmias linked to CX lesions were more frequent in NSTEMI. These findings highlight the need for tailored risk assessment and management strategies, particularly in patients with NSTEMI.