Complicated aortic aneurysms are associated with a high mortality rate: abdominal aortic aneurysm (AAA) rupture is responsible for approximately 150,000–200,000 deaths worldwide annually.1 Current clinical practice guidelines recommend endovascular aneurysm repair (EVAR) as the treatment of choice for both elective and emergency AAA repair, provided anatomic conditions are suitable.2,3 The alternative option, open surgical reconstruction (OSR), has been associated with higher short-term morbidity and mortality in clinical registries and observational studies.4,5 However, randomized controlled clinical trials have confirmed this difference in mortality only for elective AAA repair6,7 not in emergent cases.8,9 Nevertheless, the widespread adoption of EVAR has been accompanied by a significant reduction in mortality from both ruptured and unruptured AAAs in the United States. This occurred simultaneously with an increase in elective AAA repairs and a decline in the incidence of ruptured AAAs.3
A similar decrease in AAA-associated mortality has been observed in most populations worldwide; one of the few exceptions was Romania, with a continuously growing incidence of deaths related to this condition.10,11 Specifically, between 1994 and 2010, the average annual increase in AAA-associated mortality in Romania was 1.7% for men and 1% for women.10 In absolute numbers, 421 people died from aortic aneurysms in 1990, compared to 889 in 2019 (an increase of 111.5%).12 Beyond scientific evidence, the choice of therapeutic approach may also be influenced by the availability of human and financial resources, especially in low- and middle-income countries such as Romania, as EVAR interventions are typically expensive procedures. Notably, although EVAR interventions have been funded by the government since 2010,13 the treatment of ruptured aneurysms in Romania was still predominantly performed using OSR as of 2011,14 and no reliable data are available about the present-day situation.
This study had the following objectives:
to identify the possible drivers of treatment selection strategy (OSR vs. EVAR for AAA);
to analyze hospitalization and procedural costs;
to analyze the morbidity and mortality associated with AAA repair;
to determine whether the introduction of EVAR lead to a reduction of AAA-related mortality in Romania.
As part of the project entitled “Development of public research and progress infrastructure and creation of new infrastructures – AngioNet” of the Romanian Academy of Medical Sciences,15 a double-center clinical registry of EVAR cases was initiated, involving the two tertiary cardiovascular centers of the north-western and central regions of Romania: the Emergency Institute for Cardiovascular Diseases and Transplantation from Târgu Mureș and the Niculae Stăncioiu Heart Institute from Cluj-Napoca. Consecutive patients with AAAs treated by endovascular stent graft implantation at these two centers have been prospectively enrolled in the registry since January 2016 (Târgu Mureș) and April 2017 (Cluj Napoca). These patients constituted the prospective arm of the present study. The registry data were analyzed in June 2021. The registry platform is accessible online at: http://anevrisme.angionet.ro/. Patients treated with OSR for AAA during the same period of time were retrospectively included from both centers and formed the retrospective arm of the study.
All patients were at least 18 years old at the time of inclusion in the study and signed a written informed consent regarding their participation in the trial (prospective arm) or regarding personal and medical data processing (retrospective arm). Only patients with incomplete clinical data were excluded from the analysis. The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the Emergency Institute for Cardiovascular Diseases and Transplantation (protocol no. 96/05.01.2016) and by the Ethics Committee of “Niculae Stancioiu” Heart Institute (protocol no. 3713/12.04.2017).
The same demographic, clinical, and procedural data were collected for both the prospective and retrospective arms of the study. Accordingly, the following were recorded for all patients: date of birth, age at the time of intervention, sex, date of hospital admission, type of presentation (elective or emergent), comorbidities, laboratory results, and computed tomography data (including maximum aortic diameter and the presence of aortic rupture). Comorbidity history included arterial hypertension, diabetes mellitus, and pulmonary, cerebrovascular, or cardiovascular disease (the latter defined as coronary artery disease and/or heart failure). The main laboratory parameters collected at the time of hospital admission (i.e., before the reconstruction procedure) were hemoglobin concentration and serum creatinine level.
EVAR procedures were performed by interventional cardiologists, whereas OSR interventions were carried out by cardiovascular surgeons in both institutions. Three types of stent grafts were used in EVAR procedures: the Medtronic EndurantTM (47 cases, 82.4%), the Jotec E-tegraTM (7 cases, 12.3%) and the Endologix Ovation iXTM (3 cases, 5.3%). In 95% of the EVAR cases, the access site was closed percutaneously. The choice of reconstruction technique was based on both anatomical criteria and the availability of local resources, including surgical teams and medical devices required for EVAR and/or OSR. Although a permanent cardiovascular surgery service was available for emergency cases in both hospitals, each institution had only one interventional team performing EVAR. Procedural techniques for both types of reconstruction were in accordance with the current clinical practice guidelines of the European Society for Vascular Surgery.2,16
Patients in the prospective arm were followed through regular clinical visits and/or telephone interviews. For patients in the retrospective arm, in-hospital evolution was obtained from clinical records. Mortality data (i.e., date of death) were provided by the Romanian National Health Insurance House database. As the exact cause of death was not available from this source, all-cause mortality during the follow-up period is reported in the present study.
The same outcomes were monitored in both study arms: procedural morbidity (i.e., the occurrence of complications following the reconstruction procedure) and post-procedural mortality (in hospital, at 30 days, and at 1 year after the intervention). The following procedural complications were recorded: major hemorrhage, infection, stroke, acute coronary syndrome, need for renal replacement therapy, respiratory failure, mesenteric ischemia, and any other significant complication occurring during hospitalization. Hemorrhage was defined as blood loss of class II or higher according to the Advanced Trauma Life Support classification. 17 Infection included access site/wound-related, endograft-related, respiratory, or systemic infections. Endoleaks following EVAR were actively assessed through contrast-enhanced computed tomography at 1, 3, and 12 months after the intervention. Additional variables analyzed included the time between hospital admission and intervention (preoperative days), length of stay in the intensive care unit (ICU), and total hospital stay. Mortality data were also compared with previously published results from Cluj-Napoca for the 2003–2011 period14 to evaluate potential changes in AAA-related mortality trends.
The Romanian healthcare system is financed by the National Health Insurance House (NHIH) through a diagnosis-related group (DRG)-based payment system. However, certain specific (and typically expensive) therapeutic procedures are funded separately by the NHIH through national healthcare programs, based on a predetermined average cost for the medical devices used. In the case of AAA treatment, hospitalization costs are covered from two sources: the cost of medical devices used for both EVAR and OSR is reimbursed through the national cardiovascular healthcare programs, while the general hospitalization costs are covered under the DRG system.
Costs were measured at the patient level, accounting for all expenditures associated with hospitalization, using the standard controlling methodology for cost assessment18: operating room costs, ICU costs, medical device costs, diagnostic procedures, and general care costs. Due to the significant increase in salary levels in 2018,18 the year 2019 was chosen as the reference year for cost data. All unit costs were calculated for 2019 and applied to the other study years, with adjustments based on relevant medical parameters from each period, including OR time, ICU days, total length of hospital stay, and medical device costs. The average hospitalization cost for each intervention type (EVAR and OSR) was calculated for the entire study period. The year 2019 was used as the reference because, starting in 2020, the COVID-19 pandemic may have temporarily influenced healthcare costs.
Categorical variables were analyzed using Fisher's exact test, and continuous variables were compared using the Mann–Whitney test. Normality of data distribution was assessed using the Kolmogorov–Smirnov test. The EVAR and OSR arms of the study as well as the patients with and without AAA rupture were systematically compared with respect to predefined clinical outcomes. Procedural complications were analyzed both as binary variables (presence or absence of any complication) and as a count variable (total number of complications per case). Logistic regression was used to predict the occurrence of complications, in-hospital mortality and 1-year mortality. Cox proportional hazards regression was applied to assess the risk of mortality following aortic reconstruction interventions. A probability value of < 0.05 was considered statistically significant. Data analysis was conducted using R Statistical Software v.4.1.3 (R Core Team) and MedCalc v.20.110 (MedCalc Software).
A total of 119 patients were treated for AAA at the two participating centers during the study period. Two patients (one from each center) were excluded due to missing computed tomography data, resulting in a final study population of 117 patients, 57 of whom were treated by EVAR and 60 by OSR. The two centers included in the study serve patients from 12 of Romania's 41 counties, covering a total population of nearly 5.5 million inhabitants. At the beginning of the study, no other hospitals in the region were treating AAAs. After 2017, three additional hospitals began offering AAA treatment; however, their case volumes have remained significantly lower than those of the two tertiary centers. Of the included patients, 96 (82%) were from neighboring counties, while the remaining 21 were from other regions of Romania. The demographic and clinical characteristics of the study population are summarized in Table 1. Patients with ruptured AAA were significantly older, had larger maximum aortic diameters, and exhibited more comorbidities, including renal dysfunction, anemia, and a history of cerebrovascular disease.
Demographic and clinical variables of the analyzed patient population, considering the applied aortic reconstruction strategy and aneurysm rupture
| Parameter | EVAR (n = 57) | OSR (n = 60) | p value | Ruptured AAA (n = 46) | Non-ruptured AAA (n = 71) | p value |
|---|---|---|---|---|---|---|
| Included from Târgu Mureș (n, %) | 37 (64.9) | 36 (60.0) | 0.70 | 29 (63.0) | 44 (62.0) | 1.00 |
| Age (years)* | 67 (51–82) | 72 (52–87) | 0.07 | 73.0 (52–87) | 68 (51–82) | 0.01 |
| Male sex (n, %) | 53 (93.0) | 52 (86.7) | 0.36 | 41 (89.1) | 64 (90.1) | 1.00 |
| Emergent presentation (n, %) | 13 (22.8) | 48 (80.0) | <0.001 | 46 (100) | 15 (21.1) | <0.001 |
| Maximum aortic diameter (mm)* | 63 (37–120) | 80 (30–160) | <0.01 | 88 (33–160) | 63 (30–120) | <0.001 |
| Hemoglobin concentration (g/dl)* | 13.3 (7.4–17.9) | 10.42 (5.2–16.0) | <0.001 | 9.65 (5.2–14.6) | 13.6 (7.4–17.9) | <0.001 |
| Serum creatinine (mg/dl)* | 0.95 (0.73–2.40) | 1.28 (0.61–6.69) | <0.001 | 1.42 (0.72–6.69) | 0.98 (0.61–2.40) | <0.001 |
| Arterial hypertension (n, %) | 47 (82.5) | 45 (75.0) | 0.37 | 31 (67.4) | 61 (85.9) | 0.02 |
| Diabetes mellitus (n, %) | 11 (19.3) | 15 (25.0) | 0.50 | 9 (19.6) | 17 (23.9) | 0.65 |
| Cardiovascular disease history (n, %) | 19 (33.3) | 26 (43.3) | 0.32 | 17 (37.0) | 28 (39.4) | 0.84 |
| Pulmonary disease history (n, %) | 8 (14.0) | 8 (13.3) | 1.00 | 6 (13.0) | 10 (14.1) | 1.00 |
| Cerebrovascular disease history (n, %) | 0 (0.0) | 6 (10.0) | 0.02 | 5 (10.9) | 1 (1.4) | 0.03 |
| In-hospital mortality (n, %) | 2 (3.5) | 28 (46.7) | <0.001 | 29 (63.0) | 1 (1.4) | <0.001 |
| 1-year mortality (n, %) | 4 (9.8) | 30 (53.6) | <0.001 | 31 (72.6) | 3 (5.6) | <0.001 |
Median values with range are reported
A total of 73 patients (61.5%) were included from Târgu Mureș (Table 1). Except for the prevalence of arterial hypertension, there were no significant differences between the patient populations from the two centers (all p > 0.05 for the other parameters listed in Table 1). Specifically, 52 patients (71.2%) from Târgu Mureș and 42 patients (90.9%) from Cluj-Napoca were hypertensive (p = 0.01). The prevalence of AAA rupture was also similar between the centers: 29 cases (39.7%) in Târgu Mureș and 17 cases (38.6%) in Cluj-Napoca (p = 1.00). The median follow-up period of the included patients was 366 days (range 0–1,933 days). At the time of the database analysis, 97 patients (82.9%) had completed the 1-year follow-up, and two patients (1.7%) were lost to follow-up.
More than half of the patients (52.1%) were admitted as emergencies, and 39.3% of the included subjects presented with a ruptured AAA. However, EVAR was chosen as treatment modality in only one case of ruptured aneurysm. Consequently, while only 1.8% of the prospective study arm was treated for a ruptured AAA, 75% of the OSR procedures (45 interventions) were performed for rupture cases (p < 0.001). Importantly, there were no significant differences between the two participating centers in the choice of EVAR or OSR for either elective or ruptured AAA cases (all p > 0.05).
A high rate of postoperative morbidity was observed: 44 patients (37.6%) presented at least one significant adverse event following the reconstruction procedure. Complications were notably more frequent after open surgery: 5 patients (8.8%) in the EVAR group vs. 39 patients (65%) in the OSR group had at least one complication (p < 0.001). Not surprisingly, complications were also more frequent following the repair of ruptured AAAs, occurring in 38 patients (82.6%) with rupture and in only 6 patients (8.5%) without rupture (p < 0.001). A detailed breakdown of the various postoperative complications is presented in Table 2.
Postoperative complications in the analyzed patient population
| Parameter | EVAR (n = 57) | OSR (n = 60) | p value | Ruptured AAA (n = 46) | Non-ruptured AAA (n = 71) | p value |
|---|---|---|---|---|---|---|
| Hemorrhage (n, %) | 1 (1.8) | 17 (28.3) | <0.001 | 18 (39.1) | 0 (0.0) | <0.001 |
| Infection (n, %) | 4 (7.0) | 7 (11.7) | 0.52 | 7 (15.2) | 4 (5.6) | 0.10 |
| Stroke (n, %) | 1 (1.8) | 1 (1.7) | 1.00 | 2 (4.3) | 0 (0.0) | 0.15 |
| Acute coronary syndrome (n, %) | 0 (0.0) | 10 (16.7) | 0.001 | 10 (21.7) | 0 (0.0) | <0.001 |
| Mesenteric ischemia (n, %) | 0 (0.0) | 6 (10.0) | 0.02 | 6 (13.0) | 0 (0.0) | <0.01 |
| Dialysis (n, %) | 1 (1.8) | 14 (23.3) | <0.001 | 15 (32.6) | 0 (0.0) | <0.001 |
| Respiratory failure (n, %) | 2 (3.5) | 4 (6.7) | 0.67 | 5 (10.9) | 1 (1.4) | 0.03 |
| Endoleak (n, %) | 1 (1.8) | 0.0 | 0.48 | 0 (0.0) | 1 (1.4) | 1.00 |
| Other significant complications (n, %) | 0 (0.0) | 28 (46.7) | <0.001 | 27 (58.7) | 1 (1.4) | <0.001 |
Table 3 summarizes the results of the association analysis between clinical parameters and postoperative complications. Due to the low number of individual adverse events, complications were analyzed as a binary variable, dividing the patients into two groups based on the presence or absence of at least one postoperative complication.
Association between clinical parameters and postoperative complications
| Proposed predictors | With complications (n = 44) | Without complications (n = 73) | p value |
|---|---|---|---|
| Included from Târgu Mureș (n, %) | 29 (65.9) | 44 (60.3) | 0.56 |
| Age (years)* | 73.5 (54–87) | 68 (51–84) | <0.01 |
| Male sex (n, %) | 39 (88.6) | 66 (90.4) | 0.76 |
| Maximum aortic diameter (mm)* | 82 (30–160) | 63 (37–120) | <0.001 |
| Presence of aortic rupture (n, %) | 38 (86.4) | 8 (11.0) | <0.001 |
| Hemoglobin concentration (g/dl)* | 9.55 (5.2–14.8) | 13.4 (8.3–17.9) | <0.001 |
| Serum creatinine (mg/dl)* | 1.38 (0.72–6.69) | 1.01 (0.61–2.40) | <0.001 |
| Arterial hypertension (n, %) | 29 (65.9) | 63 (86.3) | 0.01 |
| Diabetes mellitus (n, %) | 10 (22.7) | 16 (21.9) | 1.00 |
| Cardiovascular disease history (n, %) | 17 (38.6) | 28 (38.4) | 1.00 |
| Pulmonary disease history (n, %) | 4 (9.1) | 12 (16.4) | 0.40 |
| Cerebrovascular disease history (n, %) | 5 (11.4) | 1 (1.4) | 0.02 |
| EVAR as treatment (n, %) | 5 (11.4) | 52 (71.2) | <0.001 |
Median values with range are reported
In summary, Table 1 and 2 show that OSR was associated with a higher likelihood of postoperative events and a greater number of complications. As OSR was preferentially used in cases of aortic rupture, these findings are at least partially explained by the severity of the clinical presentation.
The overall in-hospital and 1-year mortality in the study population were 25.6% and 35.1%, respectively. Mortality was especially high in the first 48 hours in the OSR group: 22 (78.6%) of the 28 patients who died during the index hospital admission passed away in the first 2 days postoperatively. Mortality rates stratified by type of reconstruction therapy and the presence of aortic rupture are presented in Table 1. Both OSR and aortic rupture were strongly associated with a significantly higher mortality rate. Potential predictors of short- and medium-term mortality are presented in Table 4.
Correlational analysis of potential predictors of in-hospital and 1-year mortality following AAA treatment
| Proposed predictors | Deceased in hospital (n = 30) | Discharged alive (n =87) | p value | Deceased at 1 year (n = 34) | Alive at 1 year (n = 63) | p value |
|---|---|---|---|---|---|---|
| Included from Târgu Mureș (n, %) | 21 (70.0) | 52 (59.8) | 0.38 | 26 (76.5) | 38 (60.3) | 0.12 |
| Age (years)* | 73.5 (54–84) | 68 (51–87) | <0.01 | 74 (54–87) | 68 (51–82) | <0.001 |
| Male sex (n, %) | 25 (83.3) | 80 (92.0) | 0.18 | 29 (85.3) | 58 (92.1) | 0.31 |
| Maximum aortic diameter (mm)* | 89.5 (40–160) | 64 (30–150) | <0.001 | 88 (40–160) | 64 (30–120) | 0.001 |
| Presence of aortic rupture (n, %) | 29 (96.7) | 17 (19.5) | <0.001 | 31 (91.2) | 12 (19.0) | <0.001 |
| Hemoglobin concentration (g/dl)* | 9.85 (5.2–14.6) | 13.2 (6.5–17.9) | <0.001 | 9.85 (5.2–15.3) | 13.3 (6.8–17.9) | <0.001 |
| Serum creatinine (mg/dl)* | 1.45 (0.72–6.69) | 1.01 (0.61–5.8) | <0.001 | 1.42 (0.81–6.69) | 0.96 (0.61–2.91) | <0.001 |
| Arterial hypertension (n, %) | 18 (60.0) | 74 (85.1) | <0.01 | 20 (58.8) | 55 (87.3) | <0.01 |
| Diabetes mellitus (n, %) | 5 (16.7) | 21 (24.1) | 0.45 | 7 (20.6) | 13 (20.6) | 1.00 |
| Cardiovascular disease history (n, %) | 15 (50.0) | 30 (34.5) | 0.19 | 15 (44.1) | 22 (34.9) | 0.38 |
| Pulmonary disease history (n, %) | 4 (13.3) | 12 (13.8) | 1.00 | 4 (11.8) | 9 (14.3) | 1.00 |
| Cerebrovascular disease history (n, %) | 5 (16.7) | 1 (1.1) | <0.001 | 5 (14.7) | 1 (1.6) | 0.01 |
| EVAR as treatment (n, %) | 2 (6.7) | 55 (63.2) | <0.001 | 4 (11.8) | 37 (58.7) | <0.001 |
| Any postoperative complication (n, %) | 28 (93.3) | 16 (18.4) | <0.001 | 30 (88.2) | 10 (15.9) | <0.001 |
Median values with range are reported
Table 5 summarizes the impact of clinical parameters on mortality. In-hospital mortality was predicted by the maximum aortic diameter and the presence of cardiovascular and cerebrovascular disease history. Treatment was once again statistically significant, OSR leading to higher mortality than EVAR. In addition, the occurrence of any postoperative complications was strongly associated with in-hospital mortality.
Multivariate stepwise regression models predicting mortality
| Model | Deceased in hospital | Deceased at 1 year | Cox regression |
|---|---|---|---|
| Included from Cluj-Napoca (Târgu Mureș as reference) | – | – | 0.454 (p = 0.046) |
| Age (years) | – | 0.205 (p = 0.002) | 1.002 (p = 0.934) |
| Male sex | – | – | 1.516 (p = 0.402) |
| Maximum aortic diameter (mm) | 0.029 (p = 0.044) | 0.049 (p = 0.020) | – |
| Hemoglobin concentration (g/dl) | – | – | – |
| Serum creatinine (mg/dl) | – | 1.504 (p = 0.025) | – |
| Arterial hypertension | –1.413 (p = 0.090) | –1.877 (p = 0.083) | – |
| Cardiovascular and cerebrovascular disease history | 2.727 (p = 0.003) | – | 2.101 (p = 0.035) |
| Pulmonary disease history | – | – | – |
| OSR (EVAR as reference) | 2.192 (p = 0.034) | – | 2.778 (p = 0.044) |
| Any postoperative complications | 3.799 (p < 0.001) | 2.618 (p = 0.001) | 8.457 (p < 0.001) |
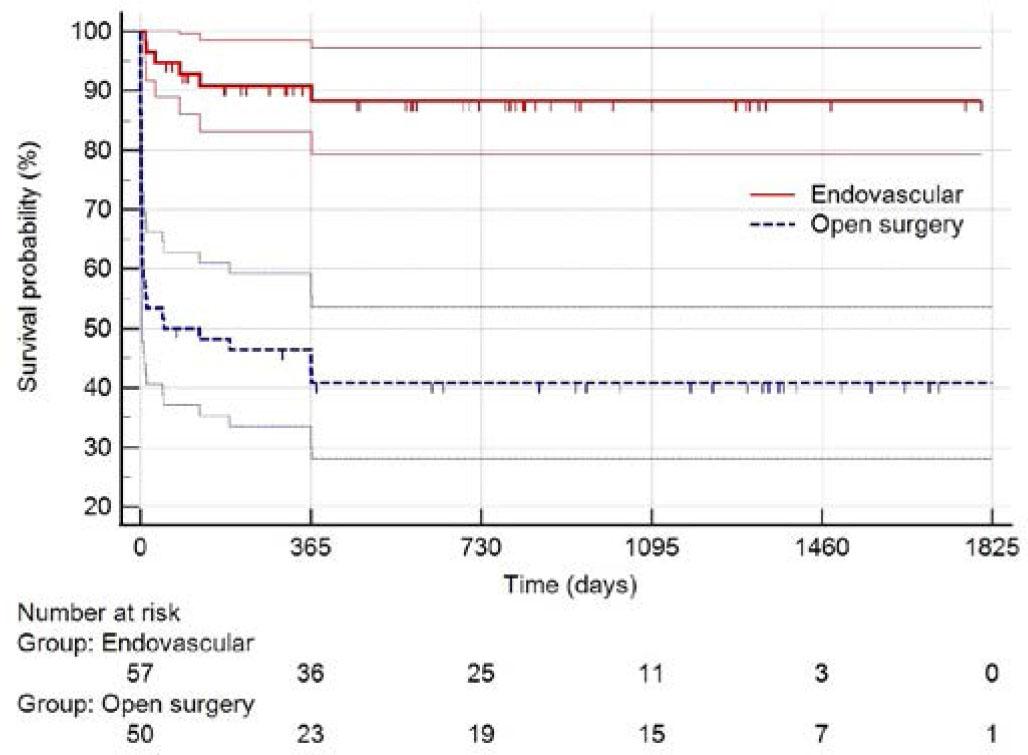
The logistic regression model predicting 1-year mortality, developed using stepwise selection of predictors, identified age, maximum aortic diameter, and serum creatinine as relevant predictors. The presence of any postoperative complications was strongly associated with increased 1-year mortality. The logistic model had a predictive power of 95.38%, compared with the baseline model, which had only 65% accuracy. The Cox proportional hazards regression, also based on stepwise selection of variables, showed that a history of cardiovascular and cerebrovascular disease had an adverse effect on mortality (HR = 2.101; 95% CI 1.053–4.19; p = 0.035). Once again, the occurrence of postoperative complications led to adverse outcomes (HR = 8.457; 95% CI 3.189–22.432; p < 0.001), and OSR resulted in higher mortality than EVAR (HR = 2.778; 95% CI 1.029–7.499; p = 0.044). The Kaplan–Meier curves presented in Figures 3 and 4 illustrate survival time by treatment and by the occurrence of complications, supporting the results presented in Table 5.
In summary, we found that OSR is associated with a higher probability of in-hospital mortality and shorter lower survival time, but not with 1-year mortality. Meanwhile, the occurrence of any postoperative complications has an adverse effect on mortality regardless of how it is measured. These observations are at least partially explained by the fact that OSR was preferred over EVAR in emergency settings.
Regarding mortality trends, published data from Cluj-Napoca14 reported an overall OSR mortality rate of 20.3% between 2003 and 2011 (5.7% in elective cases and 46.0% in emergent cases). These figures are similar to the mortality rates observed in the current study population treated with either EVAR or OSR (overall in-hospital mortality of 25.6%, p = 0.36; 1.4% mortality among patients with intact AAA, p = 0.22; and 63.0% mortality among those with ruptured AAA during the index hospital admission, p = 0.10). However, the preferential use of OSR in emergency settings was associated with a significantly increased mortality rate for this procedure: from 20.3% in the 2003–2011 period to 46.7% in the 2016–2021 period (p < 0.001).
The total costs of OSR and of ruptured AAA treatment were significantly lower than the expenditures associated with EVAR and non-ruptured AAA, respectively (Table 6). This could be explained by the high early mortality rate in the OSR group and among patients with aortic rupture. Indeed, patients treated by OSR and those presenting as emergencies had similarly shorter hospital stays than those treated by EVAR or admitted for elective AAA repair, respectively (Table 6). Another explanation is the significantly higher costs of specific medical devices used during EVAR. While the median costs per patient increased by 235.2% due to device-related expenses in the case of EVAR, this increase was only 10.3% in the case of OSR. A similar discrepancy was observed when comparing the cost of devices used for ruptured AAAs (typically treated by OSR) and non-ruptured AAAs (mostly treated by EVAR): the median cost increase was 9.9% and 204.9%, respectively (Table 6).
Length of hospitalization and total costs per patient
| Parameter | EVAR (n = 57) | OSR (n = 60) | p value | Ruptured AAA (n = 46) | Non-ruptured AAA (n = 71) | p value |
|---|---|---|---|---|---|---|
| Length of hospital stay (days) | 8.0 (3–83) | 8.5 (0–50) | 0.44 | 6.0 (0.0–50.0) | 9.0 (3.0–83.0) | <0.01 |
| Length of ICU stay (days) | 1.0 (0.2–10.3) | 2.45 (0.0–42.7) | <0.01 | 2.7 (0.0–42.7) | 1.0 (0.2–8.0) | <0.01 |
| Preoperative period (days) | 3.0 (0.0–70.0) | 0.0 (0.0–9.0) | <0.001 | 0.0 (0.0–8.0) | 2.0 (0.0–70.0) | <0.001 |
| Total costs without specific medical devices (Euro) | 4,097 (1,195–22,606) | 5,430 (131–67,646) | 0.84 | 5,619 (131–67,646) | 4,306 (1,195–22,606) | 0.84 |
| Total costs including specific medical devices (Euro) | 13,734 (10,016–40,363) | 5,989 (690–68,205) | <0.001 | 6,178 (690–68,205) | 13,131 (3,107–40,363) | <0.001 |
Median values with range are reported
The median preoperative period (i.e., the time between hospital admission and the day of the reconstruction procedure) was significantly longer in EVAR cases – another potential contributor to higher overall costs. This finding indicates that endovascular procedures typically required more planning, including many times the acquisition of stent-grafts by the hospital, because even tertiary centers do not have an appropriately diversified stock of specific medical devices. Conversely, the limited availability of stent-graft stocks may partly explain why OSR was the preferred treatment for ruptured aneurysms, where the lifesaving intervention was performed on the day of hospital admission in most cases (Table 6). Notably, the only EVAR performed for a ruptured AAA was carried out after a 3-day planning period. OSR and AAA rupture were both associated with significantly longer ICU stays, emphasizing the higher morbidity associated with OSR. However, this difference did not increase the costs of OSR compared to those of EVAR.
To the best of our knowledge, this is the first study comparing endovascular and OSR procedures for AAA in Romania. The existing reports about EVAR describe only isolated cases of aortic aneurysms treated percutaneously19,20,21 or the outcomes of a limited number of elective EVAR cases.22,23
The main determinants of postoperative morbidity (occurrence of adverse events, length of ICU stay) were the presence of aortic rupture and the type of reconstruction therapy. However, these two variables were strongly associated with each other (odds ratio = 158.45, p < 0.001), making their inclusion in the same multivariate model inappropriate. This strong correlation is also reflected by the fact that only one patient with aortic rupture was treated by EVAR, whereas 75% of patients treated by OSR had a ruptured aneurysm. EVAR is known to be associated with lower rates of hemorrhage, acute renal failure, myocardial infarction and mesenteric ischemia.3,7,24 These observations were consistent with our results (Table 2).
Besides treatment choice and the presence of rupture, other determinants of postprocedural complications included larger aneurysm diameter and the presence of anemia (Table 4, Figures 1 and 2). Both factors are known predictors of morbidity following AAA repair.25,26 Moreover, the two conditions are often interrelated and have also been associated with reduced long-term survival after AAA repair.27
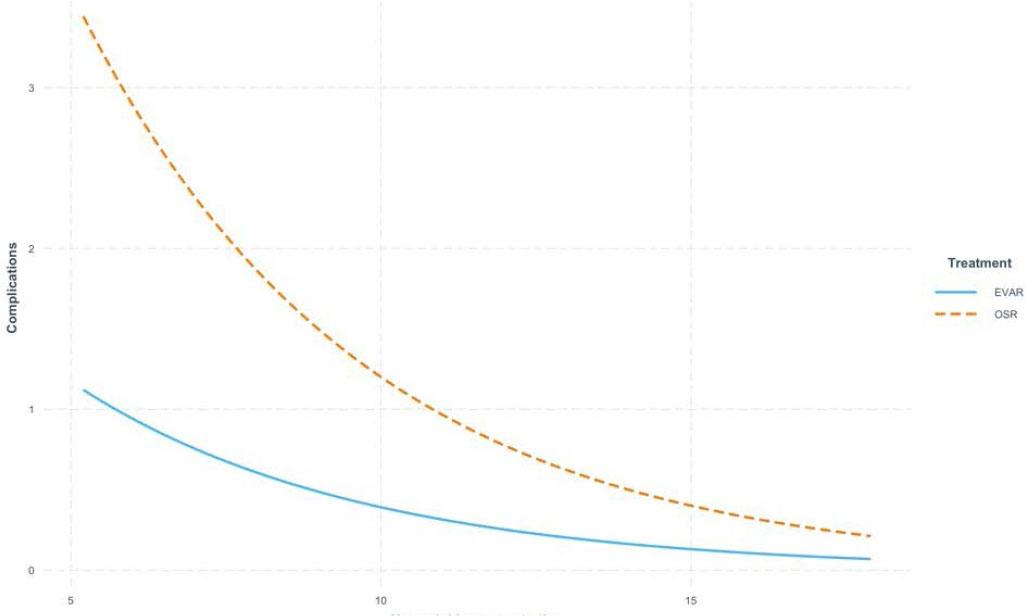
The effect of hemoglobin concentration (g/dl) on the number of complications according to the chosen treatment strategy. As hemoglobin levels increase, the difference in complication rates between EVAR and OSR decreases.
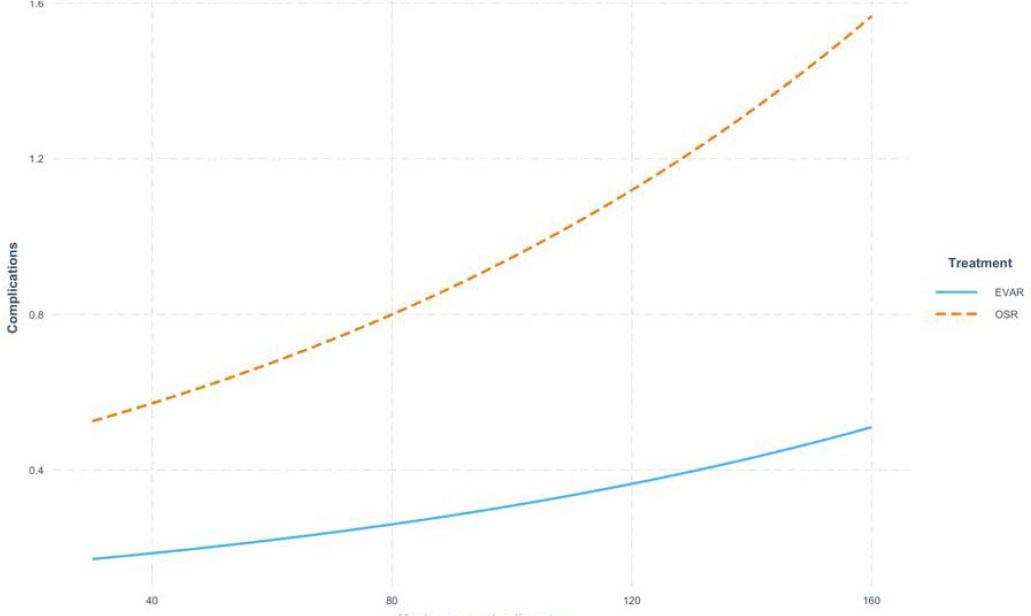
The effect of the maximum aortic diameter (mm) on the number of complications, according to the chosen treatment strategy. As the aortic diameter increases, the number of complications resulting from OSR increasingly diverge from those resulting from EVAR.
Regarding ICU stay, the main determinants of longer duration, aside from specific local protocols (Cluj-Napoca reported a significantly longer median ICU stay), were the type of treatment and the presence of arterial hypertension. OSR was a significant predictor of prolonged ICU stay. These findings are consistent with previous studies showing longer hospital stay after OSR compared to EVAR.3,28 Interestingly, arterial hypertension was associated with a shorter ICU stay, which was an unexpected result. This may be explained by the fact that, in our study population, patients with aortic rupture were more likely to be free of arterial hypertension (Table 1). As discussed earlier, aortic rupture could not be included in the multivariate model due to its strong association with the type of reconstruction therapy. The other two determinants of complications – anemia and larger aneurysm diameter – were only marginally associated with a longer ICU stays (p = 0.08 and p = 0.05, respectively, in the stepwise multiple linear regression analysis).
Early- and mid-term mortality following AAA reconstruction remained high during the study period, especially among patients undergoing OSR and those presenting with ruptured AAAs. As expected, both OSR and AAA rupture were associated with significantly higher in-hospital and 1-year mortality. However, similarly to the postoperative morbidity analysis, these two variables were not included in the same multivariate model due to their strong interdependence. Nevertheless, the observed mortality rates were consistent with those reported in previous clinical studies.6,7,8,14,29,30,31,32 Given the well-established association between aortic rupture and increased rates of postoperative complications and mortality,2,3 and the inability to statistically isolate the effects of rupture and treatment type in this analysis, we believe that the increased complication and mortality rates observed were more likely determined by the presence of aortic rupture. Moreover, the strong statistical association between rupture and treatment type indicates that rupture strongly influenced treatment selection in the studied population. Indeed, broader availability of emergency EVAR would most likely lower mortality rates in cases of ruptured AAA as well as among patients currently treated with OSR in emergent conditions.
OSR had the strongest effect on survival at the beginning of the follow-up period, i.e., during the index hospital admission (Figure 3). Although OSR was associated with a significantly lower survival probability in the first year following the intervention (Cox proportional hazards regression: HR = 2.778; 95% CI 1.029–7.499; p = 0.044), the overall 1-year mortality did not differ significantly between OSR and EVAR (logistic regression analysis p = 0.76; Table 6). It is worth mentioning that the high mortality rate observed after OSR does not reflect the performance of the operating teams, but rather the convergence of three factors: (1) OSR was preferentially used as emergency treatment; (2) it was performed in patients with more severe disease (e.g., larger or ruptured AAAs); and (3) it was applied in a patient population with poorer general condition (e.g., older age, higher prevalence of anemia, renal insufficiency, and a history of cerebrovascular disease). The early survival benefit of EVAR, which diminishes over time, has also been demonstrated in randomized controlled trials comparing endovascular and open elective AAA repair.6,7,29 Moreover, previous studies have shown that long-term survival after AAA repair becomes comparable between treatment modalities once patients survive the initial 90-day period.33 Our findings support this trend. Specifically, the Kaplan–Meier survival curves for the two treatment arms diverge at the beginning of the follow-up period (Figure 3), consistent with the preferential use of OSR for ruptured AAAs, as confirmed by the strong association found using Fisher's exact test. The comparable mid-term outcomes of OSR and EVAR for ruptured AAA repair are also supported by single- and multicenter observational studies.34,35,36
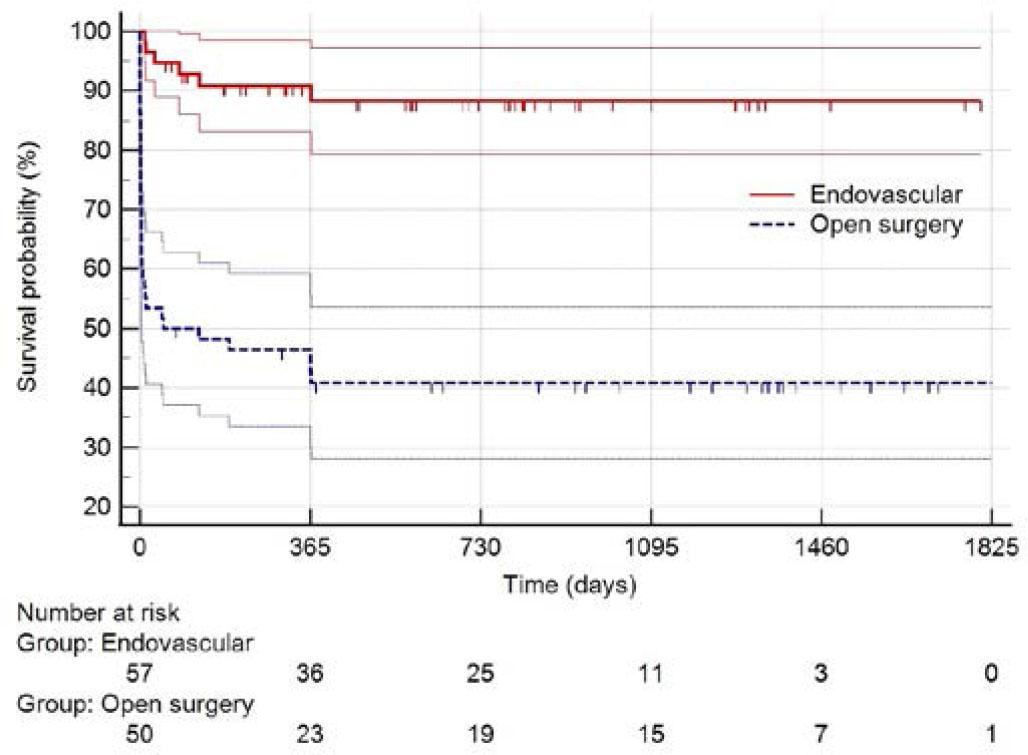
Survival time (days) after endovascular vs. open surgical aortic repair. Although survival time decreases immediately after the intervention for both EVAR and OSR, the decline is less pronounced with EVAR, and survival time remains consistently higher compared to OSR. These findings are supported by the log-rank test (Χ2 = 30.6; p < 0.001).
Survival time (days) in relation to the occurrence of postoperative adverse events. Patients without complications (strata = 0) had a longer survival time compared to those who experienced adverse events (strata = 1). These findings are supported by the log-rank test (X2 = 61.3, p < 0.001).
A third predictor of mortality was the occurrence of any postprocedural complication. Numerous complications associated with AAA reconstruction are documented predictors of both short- and mid-term mortality.2 Specifically, postoperative hemorrhage, renal failure, cerebrovascular incidents, abdominal compartment syndrome, entero-mesenteric ischemia, and multisystem organ failure have all been linked to increased in-hospital mortality.2 Our findings are consistent with these observations, as the occurrence of any postoperative adverse event was a significant predictor of mortality not only during the index hospital admission but also after 1 year of clinical evolution. Accordingly, postoperative complications should be actively identified and if possible, prevented.
Larger aneurysm diameter, renal dysfunction, and advanced age were all independent predictors of 1-year mortality following AAA repair. Each of these variables is a well-established predictor of mid-term mortality.37,38,39 In addition, larger aneurysm size was independently associated with an increased risk of procedural complications, as discussed earlier. The effect of advanced age became more apparent over time: although it was not a predictor of in-hospital mortality, younger patients demonstrated significantly better 1-year survival. Furthermore, the finding that a history of cardiovascular and cerebrovascular disease predicted in-hospital mortality highlights the importance of comprehensive cardiovascular risk assessment prior to AAA reconstruction.
An important finding of this observational study is that although EVAR has gained popularity in Romanian hospitals in recent years, it is currently available only for elective cases. As a result, ruptured AAAs continue to be treated exclusively by OSR. This situation contrasts with reports from other countries4,40,41,42,43 as well as with current clinical practice guidelines.2,3 This Romanian specificity allowed us to test whether the selective introduction of EVAR for elective cases alone affects overall AAA-related mortality. Notably, randomized controlled trials comparing EVAR and OSR for the treatment of ruptured AAAs have not demonstrated any reduction in mortality with endovascular repair.8,9,28,44 However, these findings are in contrast with the results of many observational and registry studies worldwide.30,31,45,46 Moreover, national data from the United States indicate that increased use of EVAR for ruptured AAAs is associated with lower mortality rates.42,43 Therefore, the lack of decline in mortality following the introduction of EVAR solely for intact AAAs in Romania may provide further evidence for the clinical benefit of the procedure in emergency settings.
According to our findings, the overall mortality rate of AAA has remained unchanged over the past two decades (2003–2011 vs. 2016–2021), despite the widespread adoption of EVAR in elective cases in the more recent period. While EVAR has become the preferred approach for elective AAA repair, OSR has remained the primary treatment option in cases of rupture, a strategy that was accompanied by a rise in OSR-associated mortality. Taken together, our findings suggest that treating ruptured AAAs by EVAR is important to acquire the mortality benefit of this new approach observed at the population level. In other words, it is not enough to treat only elective patients by EVAR to reduce overall AAA-related mortality. In our opinion, this observation may be particularly relevant for other services planning to implement an endovascular program for the routine treatment of AAAs.
Little is known about trends in AAA-associated mortality in Romania. A global epidemiological study reported decreasing AAA-associated mortality in many countries worldwide, but not in Romania in the 1994–2010 period. 10 Another analysis focusing on national epidemiological data also confirmed increasing AAA-related mortality in both men and women between 2001 and 2015.11 While these trends could be related to poor cardiovascular risk factor control and the lack of a dedicated AAA screening program in Romania,10,11,12 the preferential use of OSR for ruptured AAAs clearly supply additional explanations for the increasing mortality. The high number of ruptured AAAs relative to the number of elective procedures underscores the need for a screening program in Romania. The present study, although not a nationwide evaluation, shows an unchanged (but still high) in-hospital mortality rate for AAA requiring reconstruction therapy in the north-western and central regions of Romania. This finding is even more disappointing considering the recent large-scale availability of EVAR in this area. Accordingly, while in 2011 patients with AAA requiring reconstruction were treated by OSR in Cluj-Napoca,14 during the period analyzed in this study, half of the included patients were treated by EVAR. Indeed, cardiovascular diseases are known to have high mortality rates in Romania.47
One important cause of this change is the improvement in EVAR funding in Romania. While the Romanian National Health Insurance House initially provided funding for EVAR procedures only to cardiovascular surgery units in 2010,13 this support was extended to interventional cardiology services in 2013.48 To the best of our knowledge, this is the first study to report hospitalization and procedural costs associated with AAA treatment in Romania. While the costs of EVAR are comparable to those in other countries, expenditures related to OSR were significantly lower than in other European settings. For example, in the Netherlands, the cost of primary procedures calculated at the 2019 price levels (excluding the price of stent graft) was €6,576 for EVAR and €20,041 for OSR.49 Our analysis confirms that EVAR is more expensive than OSR in Romania. This cost difference is primarily due to the significantly higher prices of specific medical devices, such as percutaneously implantable stent grafts, but also reflects inconsistent use of other healthcare resources. For example, patients typically waited a median of 3 days in hospital before undergoing elective EVAR. Moreover, the total length of hospital stay did not differ between elective EVAR and OSR procedures.
These observations support the conclusion that the current management of AAA requiring with reconstruction in Romania needs to be reorganized. Given that performing endovascular repair in elective cases alone appears insufficient to reduce the persistently high AAA-related mortality, the facilitation of emergency EVAR procedures should become an important healthcare objective. In addition to implementing an efficient screening program, a possible solution would be to establish centers of excellence for aortic disease care, offering 24/7 access to emergent interventional treatment for ruptured AAAs. This requires not only an adequate number of qualified personnel, but also a sufficiently diversified inventory of dedicated medical devices. Furthermore, there is an urgent need for a more consistent and efficient use of existing resources. Improved allocation and management strategies would support the sustainable funding of such specialized centers.
The three most important limitations of this study are its observational design, the relatively small sample size, and the inclusion of both intact and ruptured AAA cases in the analysis. An additional limitation is the retrospective enrollment of patients in the OSR arm. We tried to mitigate the impact of the limited sample size by including all consecutive patients treated at two tertiary cardiovascular centers from a Romanian region covering 12 of the country's 41 counties. Notably, the patient populations from the two hospitals were homogenous regarding the baseline clinical characteristics. There were no significant differences between centers in treatment selection strategies or in the incidence of most predefined outcomes, such as in-hospital mortality and complications. The longer ICU stay observed in Cluj-Napoca likely reflects a local variation in postoperative management protocols. Although stepwise Cox regression identified higher mortality during follow-up in Târgu Mureș, neither in-hospital nor 1-year mortality differed significantly between the two hospitals based on correlation and logistic regression analyses.
We consider it important to report morbidity and mortality data for both intact and ruptured AAAs, because very little is known about this subject in Romania. To our knowledge, this is the first study to report such data from the country. The lack of information on cardiovascularcause mortality and reliance on all-cause mortality is another limitation. On the other hand, in order to assess whether the introduction of EVAR is associated with reduced AAA-related mortality from a global epidemiological perspective, it was necessary to include both intact and ruptured AAA cases in the analysis.
Finally, cost analysis was performed only for the year 2019, and the resulting data were used to estimate costs for the other periods (as detailed in the section entitled Hospitalization and intervention costs).
The possibility of treating ruptured AAAs by EVAR seems to be important to achieve the population-level survival benefit of this treatment modality. The main predictors of morbidity, in-hospital mortality, and 1-year mortality following AAA reconstruction identified in our study align with those identified in the literature. EVAR is more expensive than OSR in Romania. According to our findings, the reorganization of AAA management, especially for emergent cases, might be an important objective in the northwestern and central regions of Romania.