Despite new diagnostic and treatment options, acute coronary syndrome (ACS) remains the leading cause of mortality globally, being responsible for almost 90% of cardiovascular deaths.1 Moreover, it has been observed that ACS has an increasing incidence, particularly in younger individuals, being frequently associated with severe complications such as ventricular dilatation, heart failure, or malignant arrhythmias.2
The underlying substrate of ACS is represented by the atherosclerotic process, a chronic inflammatory disease caused by subintimal accumulation of lipids, leading to gradual narrowing of the coronary arteries. It is assumed that the early key event in the pathogenesis of atherosclerosis is represented by endothelial injury. The latter is a complex process determined by the interaction between cell apoptosis, inflammation, and oxidative stress.
Thus, atherosclerosis involves the proliferation of the smooth vascular cell as a result of local invasion and the accumulation of pro-inflammatory cytokines such as C-reactive protein (CRP), interleukins (ILs), tumor necrosis factor α (TNF-α), matrix metalloproteinases (MMPs), soluble suppression of tumorigenicity 2 (sST2), and adhesion molecules.3 The link between atherosclerosis and inflammation is far from being completely understood.4 An important aspect is the role of CRP as an inflammatory marker in atherogenesis, specifically its capacity to bind to LDL, which favors endothelial dysfunction and plaque instability. It is assumed that plaque instability is also determined by higher levels of MMP-9.5,6
In most cases, after an ACS, because of the limited regenerative capacity of cardiomyocytes, the affected myocardium heals through irreversible fibrosis. A key feature of myocardial fibrosis is the abnormal deposit of extracellular matrix proteins (EMPs), which causes hypertrophy of the remaining myocardium. One such EMP is periostin (Pn), a novel inflammatory biomarker, involved not only in the myocardial healing process but also in the acute phase, triggering and maintaining the inflammatory cascade.7,8
Pn, also known as osteoblast-specific factor 2, is an EMP composed of four repeating domains of fasciline, which promotes cell adherence and motion, and the collagen formation process. The role of Pn begins from the intrauterine period, being involved in the formation of cardiac valves and outflow tracks, having a crucial role in providing the 3D collagen scaffolding throughout cardiac biogenesis.9 Literature evidence indicates that Pn plays a critical role in wound healing and scarring after injury, partly by promoting cell proliferation and differentiation in myofibroblasts. Pn secretion is upregulated immediately after the injury and continues to increase for up to 7 days. Similarly, Pn secretion is increased in response to myocardial hypoxia, contributing to interstitial cardiac remodeling and scar formation.7,10 It was described in the literature that Pn levels are directly correlated with Killip class, N-terminal b-type natriuretic peptide, sensitive troponin, and all cardiac biomarkers directly involved in heart failure and ischemic heart pathologies.11,12 Furthermore, Pn has been shown to be involved in collagen degradation, tissue remodeling, and reducing myocardial fibrosis during the recovery process following an ACS, while preserving the tissue matrix.9
Thus, it is well known that Pn is an inflammatory biomarker involved in the intricate process of myocardial healing after an acute coronary event; however, the link between Pn serum levels in inflammation and the severity of ACS has not been clarified so far. Therefore, the aim of this study was to investigate the correlation between the serum concentrations of Pn and other pro-inflammatory cytokines, and their impact on clinical outcomes after an ACS.
This case–control, observational study was conducted in the Cardiology Department of the Emergency County Clinical Hospital of Târgu Mureș, Romania, and involved a total of 92 patients with ACS.
The diagnosis of ACS was established according to the current European guideline for the management of ACS in patients presenting without persistent ST-segment elevation myocardial infarction (NSTEMI) and with ST-segment elevation myocardial infarction (STEMI)13 as myocardial ischemia on minimal exertion or at rest. Thus, the diagnosis was based on clinical symptoms, electrocardiogram (ECG) criteria, and the serum level of myocardial enzymes. For patients with STEMI, coronary angiography was performed immediately after admission, and for those with NSTEMI, coronarography was made based on the GRACE score in the next 24–72 h. After the percutaneous coronary angiography, the patients were admitted to the intensive care unit.
At baseline, medical history and demographic data, such as sex, age, body mass index (BMI), smoking status, and possible complications during hospitalization were recorded for all patients. Additionally, an ECG was performed in all cases to determine the type of ACS – STEMI or NSTEMI.
The exclusion criteria included the following: patient refusal, intolerance to iodinated substances, active malignancy, pregnancy, acute renal failure, or end-stage renal disease.
Peripheral venous blood samples were collected from the antecubital vein immediately after admission to the intensive care unit, as well as on day 7, before discharge. All samples were centrifuged at 3,000 r.p.m., and the platelet-poor supernatant was pipetted and collected into sterile vials. The obtained samples were stored at −80 °C. Serum analysis was performed in the Centre for Advanced Medical and Pharmaceutical Research of the “George Emil Palade” University of Medicine, Pharmacy, Science and Technology, Târgu Mureș, as well as in the Cardiology Department of the County Clinical Hospital of Emergency, Târgu Mureș.
To examine the inflammatory profile, we measured serum albumin, alkaline phosphatase, and C-reactive protein at baseline and on day 7 using a Cobas Integra Plus analyzer (Roche Diagnostics). A FlexMap 3D analyzer (Luminex) was used to determine serum levels of P-selectin, and vascular and intercellular adhesion molecules (VCAM, ICAM). MMP-9 and sST2 levels were determined using a Dynes DSX ELISA (DYNEX Technologies), and IL-6 levels with an Immulite 2000 XPi analyser (Siemens Healthineers).
Regarding the presence of risk factors, smoking status was established from the patients’ personal history. A patient was defined as a smoker if he declared smoking for at least one month prior to enrolment. Hypertension was defined as blood pressure greater than or equal to 140/90 mmHg or active antihypertensive treatment. Obesity was defined as a BMI >30 kg/m2. The presence of stroke, peripheral arterial disease, or recurrent ACS were also noted.
Percutaneous coronary angiography was performed using a Philips Allura FD20/10 system (Philips Medical Systems Nederland) with ECG recording. The total amount of iodinated contrast substance was individualized for each patient according to body weight. In all cases, the approach was performed on the radial artery, using a 7 French catheter. Before the revascularization therapy, the patients received dual antiplatelet therapy and 70–100 IU/kg heparin intravenously.
The study population consisted of 92 patients with ACS. Based on the median Pn level of 30.63 pg/ml, the study population was divided into two groups – group 1, consisting of 46 subjects with low Pn serum levels, also called low Pn group (LP) and group 2, consisting of 46 patients with high Pn values, called high Pn group (HP).
For statistical analysis, Graph Pad InStat v.3.10 software (GraphPad Software) was used. Normality tests were performed for all data. Categorical variables are reported as absolute numbers and percentages, and numeric variables are reported as mean ± s.d. The study groups were compared using the Mann–Whitney test (for non-normally distributed variables), Student’s t-test (for normally distributed variables), and Fisher’s test (for categorical variables). The alpha value was set at 0.05.
The mean age of the 92 patients included in the study was 61.34 ± 10.29 years, and 67 patients (73%) were male (p = 0.04). We found an important association between STEMI and Pn levels, as STEMI occurred significantly more frequently than NSTEMI among patients with high Pn levels (p = 0.04). Regarding to the location of the culprit lesion, the left descending artery (LAD) was the most frequently involved in the HP group, but without statistical significance (p > 0.99). By contrast, in the LP group, the ACS occurred more frequently in the right coronary artery (RCA) (p = 0.67) or the circumflex artery (Cx) (p = 0.29). No significant association was found between Pn levels and obesity (p > 0.99), recurrent ACS (p > 0.99), dyslipidemia (p = 0.13), smoker status (p > 0.99), chronic renal disease (p > 0.99), diabetes mellitus (p = 0.6), or hypertension (p = 0.63). However, we found a positive association between Pn levels and heart failure (p = 0.002) as well as atrial fibrillation (p = 0.005). The baseline characteristics of the study groups are presented in Table 1.
Pro-atherogenic and prothrombotic mechanisms of Lp(a)4
| Study population (n = 92) | Group 1 – LP (n = 46) | Group 2 – HP (n = 46) | p value | |
|---|---|---|---|---|
| Baseline characteristics of the study groups | ||||
| Age, years (mean ± s.d.) | 61.34 ± 10.72 | 61.38 ± 10.29 | 61.30 ± 11.27 | 0.92 |
| Male sex, n (%) | 67 (72.82%) | 37 (40.22 %) | 30 (32.61 %) | 0.04 |
| Weight (kg, mean ± s.d.) | 83.00 ± 20.99 | 83.84 ± 19.22 | 82.21 ± 22.77 | 0.71 |
| Height (m, mean ± s.d.) | 1.70 ± 0,07 | 1.71 ± 0.08 | 1.69 ± 0.07 | 0.38 |
| BMI (kg/m2, mean ± s.d.) | 28.02 ± 6.92 | 28.35 ± 4.81 | 28.47 ± 7.18 | 0.75 |
| ACS type | ||||
| STEMI, n (%) | 63 (68.47%) | 27 (29.35 %) | 36 (39.13 %) | 0.04 |
| NSTEMI, n (%) | 29 (31.52 %) | 19 (20.65 %) | 10 (10.87 %) | |
| Cardiovascular risk factors/comorbidities | ||||
| Obesity, n (%) | 23 (25.00%) | 11 (12.22 %) | 12 (12.22 %) | >0.99 |
| Recurrent ACS, n (%) | 9 (18.75%) | 4 (4.44 %) | 5 (5.56 %) | >0.99 |
| Heart failure, n (%) | 27 (29.34 %) | 7 (7.87%) | 20 (22.47 %) | 0.002 |
| Dyslipidemia, n (%) | 54 (58.69 %) | 30 (33.33 %) | 24 (26.67 %) | 0.13 |
| Smoker status, n (%) | 41 (50.00 %) | 21 (22.83 %) | 20 (21.72 %) | >0.99 |
| Chronic renal disease, n (%) | 7 (7.60 %) | 3 (3.26 %) | 4 (4.35 %) | >0.99 |
| Diabetes mellitus, n (%) | 19 (20.65 %) | 8 (8.70 %) | 11 (11.96 %) | 0.60 |
| Hypertension, n (%) | 69 (75.00%) | 35 (77.78 %) | 34 (72.34 %) | 0.63 |
| Atrial fibrillation, n (%) | 27 (29.34%) | 7 (7.78%) | 20 (22.22%) | 0.005 |
| Culprit lesion | ||||
| Left anterior descending artery, n (%) | 68 (73.91 %) | 33 (36.67 %) | 35 (38.89 %) | >0.99 |
| Circumflex artery, n (%) | 50 (54.34 %) | 27 (30.00 %) | 23 (25.56 %) | 0.29 |
| Right coronary artery, n (%) | 53 (57.60 %) | 27 (30.00 %) | 26 (28.89 %) | 0.67 |
We also found a statistically significant negative correlation Pn and IL-6 levels (p = 0.0009; Figure 1).
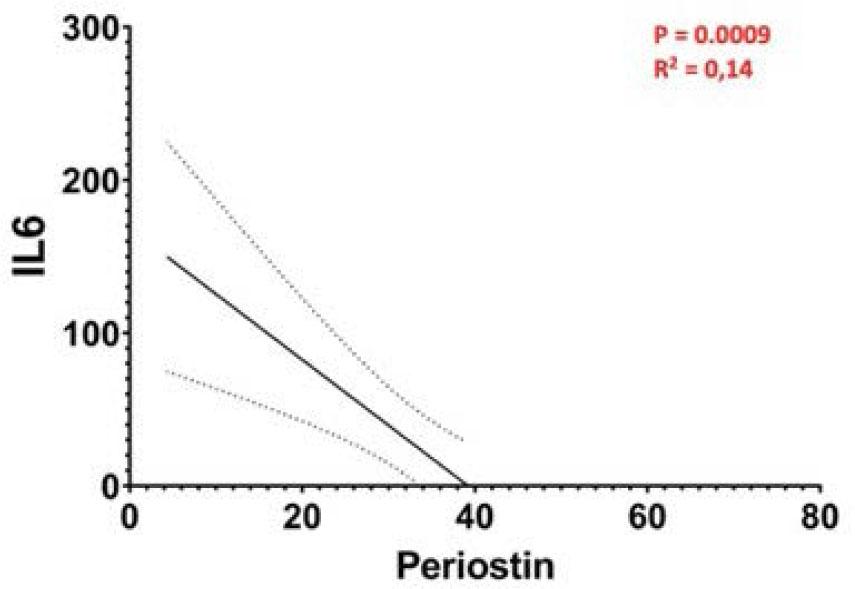
Correlation between Pn and IL-6 serum levels
Another important finding was the correlation between adhesion molecules and Pn levels (Figure 2). Although VCAM levels were higher in the HP group, the difference between the two groups was not significant (838.8 ± 179.7 ng/ml vs. 895.7 ± 212.2 ng/ml; p = 0.22). Similarly, there were no significant differences in ICAM levels between the two groups; however, they were higher in the LP group than the HP group (213.5 ± 100.9 ng/ml vs. 204.6 ± 116.5 ng/ml; p = 0.41).

Correlation between Pn and adhesion molecule serum levels
Analyzing the link between Pn and CRP serum levels in patients with ACS and periodontal disease, a negative correlation was observed (both p < 0.0001; Figure 3). At baseline, CRP levels were significantly lower in the HP group compared with the LP group (p = 0.0009; Figure 4). Next, we examined the correlation between the Pn and CRP serum levels on day 7 after the index event and found that the negative correlation was maintained (p < 0.0001; R2 = 0.20), and CRP levels were significantly higher in the LP group (31.84 ± 29.4 mg/dl vs. 19.25 ± 26.77 mg/dl; p = 0.043; Figure 5). However, in the HP group we observed that although CRP levels were low at baseline, they gradually increased, almost doubling by day 7 (9.2 ± 12.87 mg/dl vs. 19.25 ± 26.77 mg/dl; p = 0.007).
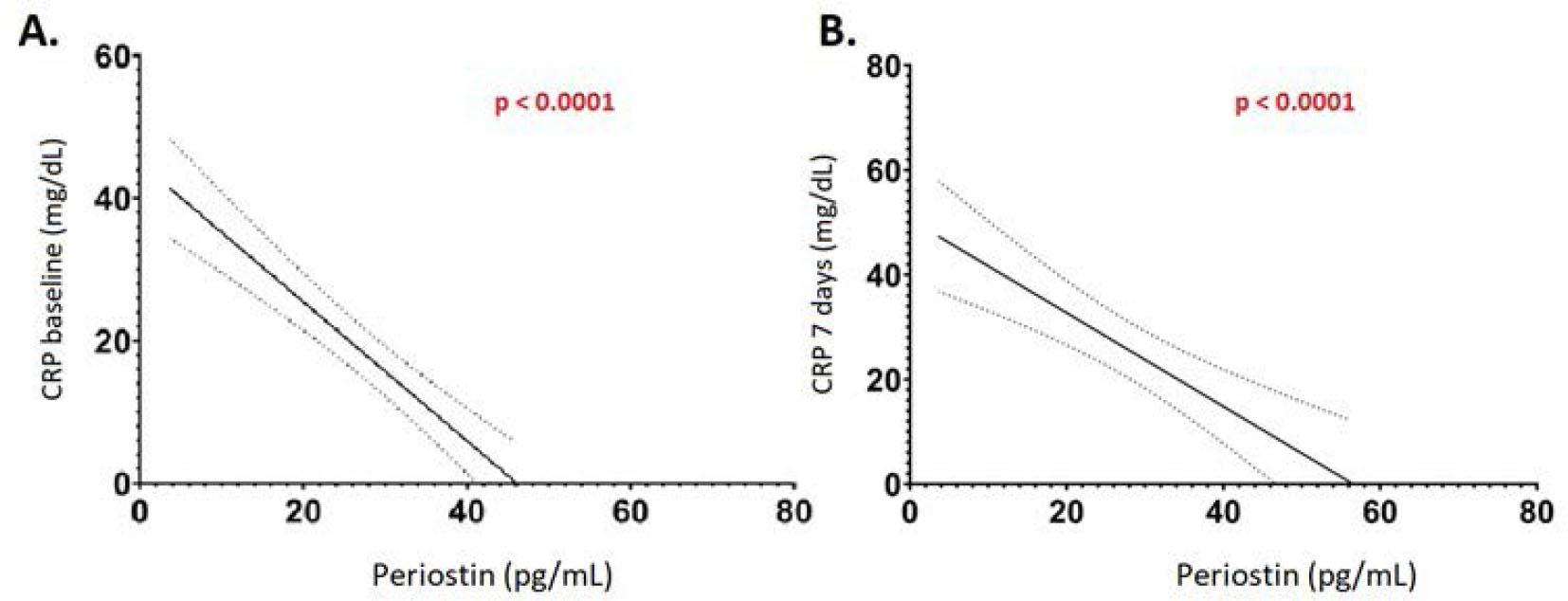
Correlation between Pn and CRP serum levels
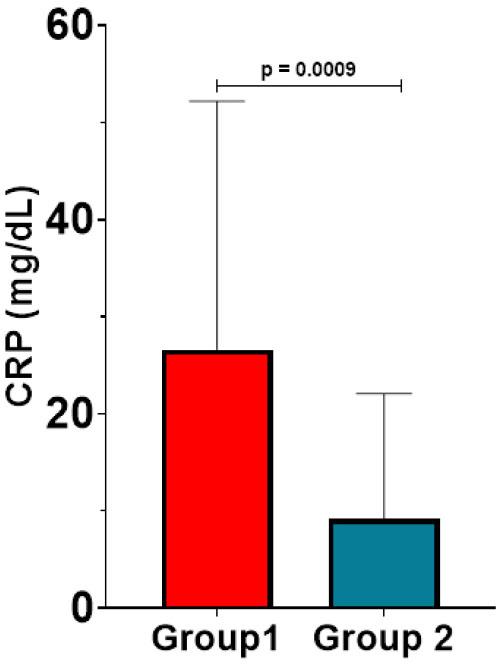
Comparison of CRP serum levels in the two groups at baseline
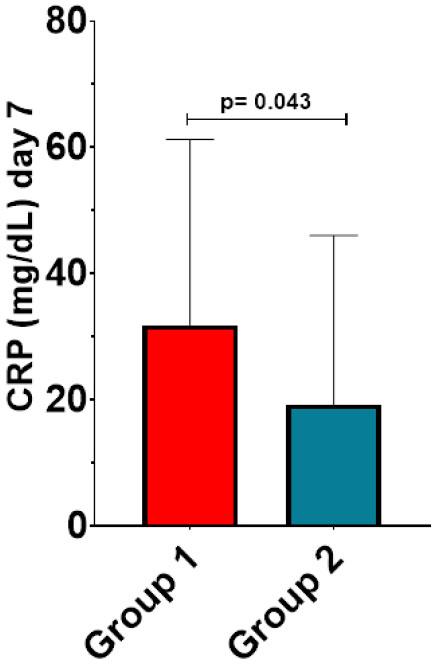
Comparison of CRP serum levels in the two groups on day 7
We found no significant association between Pn and P-selectin levels (78.78 ± 72.01 ng/ml vs. 106.2 ± 91.61 ng/ml; p = 0.17). However, in contrast to IL-6 and CRP serum levels, we found a significant positive correlation between MMP-9 and Pn levels (p < 0.0001), as well as a significant negative correlation between sST2 and total Pn levels (Figure 6).
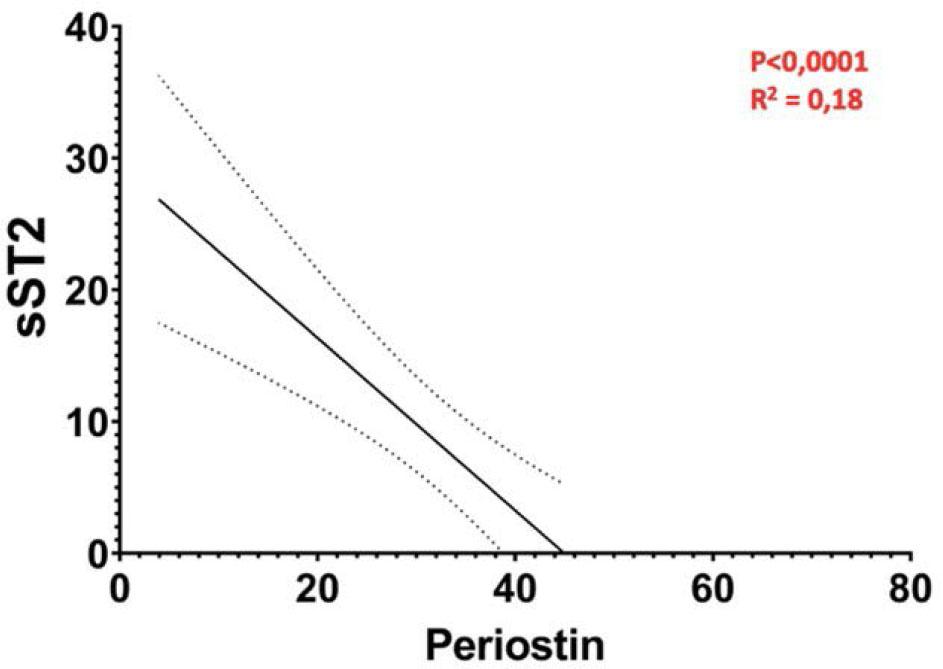
Correlation between Pn and sST2 levels
Current data regarding the correlation between Pn and inflammatory biomarkers are limited. Although it is well known that Pn plays an important role in the healing process after an ACS, in the healthy myocardium it is found only in the valves. After a cardiac injury, Pn serum levels begin to rise after approximatively 3 days and persist in the blood up to 28 days after the acute event.14 Contrary to other biomarkers, Pn levels remain augmented for up to four months, which may be explained by an early suppression after myocardial infarction.15
Comparing demographic variables between the two groups, we found no significant differences regarding age, height, weight, and BMI. However, we observed that high Pn levels were more often associated with female sex. Similar results were obtained by Azharuddin et al., who demonstrated that in a group of 40 patients with ACS, Pn serum levels were correlated with the BMI.16 Also, we found no correlation between Pn levels and traditional cardiovascular risk factors or comorbidities. Similar results were obtained by Ling et al., who found that the mean age of onset of an ACS was 63 years, and there was no significant association between Pn serum levels and history of hypertension, diabetes, smoking, or increased serum levels of glucose, creatinine, and urea.12
Another important finding of this study was the association between Pn levels and STEMI compared with other types of ACS. Moreover, in most cases, the culprit coronary artery involved in the acute event was the LAD. Data from the literature highlight a more frequent association between high Pn levels and STEMI, multivessel coronary involvement, and a higher risk of mortality.15,17 In addition, Ling et al., have found a positive correlation between Killip classification and Pn serum levels. We found no significant association between the involved artery and Pn levels, but we observed that higher Pn levels were correlated with more frequent LAD restenosis.12 Furthermore, we found a significant positive association between Pn levels and major adverse cardiovascular events in patients with STEMI; this effect is presumed to persist even after the acute phase.15
In this study, heart failure and atrial fibrillation were often associated with higher Pn levels. These findings are supported by data from the literature showing that Pn levels are positively correlated with atrial fibrosis and with worse long-term outcomes in patients with heart failure.18 Recent data have confirmed that most patients with cardiovascular disease develop heart failure, which worsens due to ischemia or myocardial infarction. Therefore, these patients have a doubled risk of cardiovascular events compared to those without heart failure.19 A study conducted by Wang et al. demonstrated that Pn is an independent risk factor for heart failure,20 and serum levels of this biomarker increase with the severity of heart failure based on the New York Heart Association classification.11 Also, it was observed that Pn levels and intramural fibrosis are significantly higher in patients with atrial fibrillation or heart failure, thus Pn may serve as a specific marker for atrial fibrillation.21 A recent study of atrial appendages from patients with atrial fibrillation showed a clear link between Pn levels in atrial tissues and deteriorated heart failure, as well as decreased ejection fraction.22
In terms of the correlation between Pn and inflammatory biomarkers, literature data are limited. Our results have shown a negative correlation between serum Pn levels and IL-6; however, the difference between our study groups was not significant. According to study results reported in the literature, Pn levels are directly correlated with IL-6 serum levels, and both are elevated in older patients.23 Another study conducted on mice had demonstrated that Pn levels are lower in mice with high IL-6 levels.24
Similar results were obtained regarding Pn and CRP levels, higher Pn levels being associated with lower CRP levels. Additionally, a comparative analysis of Pn and CRP levels showed that CRP levels were higher in the HP group, and these findings were also observed on day 7 following the ACS. Moreover, CRP levels increased from baseline to day 7 in the HP group. In a study by Cheng et al., the authors found no significant correlation between CRP and Pn levels, but they studied the link between high-sensitivity CRP and Pn.17 However, Ling et al. have shown that CRP levels are higher in patients with STEMI compared with patients with unstable angina, and also found a positive correlation between CRP and Pn levels.23
We also found a direct relationship between MMP-9 and Pn levels. Specifically, MMP-9 levels were significantly higher in the HP group, indicating a worse outcome and an increased risk of myocardial rupture in the first days following an ACS. In atherosclerotic plaques, Pn levels are elevated and contribute to atherogenesis by promoting smooth muscle cell migration, calcification, endovascular remodeling, and MMP-9 production.24 The findings of Zhao et al. support our results regarding the direct correlation between Pn and MMP-9 levels.25 Similar results were obtained by Tanabe et al., who have demonstrated that Pn induces MMP-9 secretion.26 The in vitro study of Shimazaki et al. showed that deficient Pn secretion is commonly associated with mechanical complications such as cardiac rupture.14 Furthermore, many studies have shown that the higher Pn serum levels are directly correlated with worse long-term outcomes, and that by stimulating the secretion of MMP-9, Pn contributes to the atherosclerotic process and the formation of vulnerable plaques.12,27 Following a myocardial injury, the expression of MMP is upregulated, with various cells involved in their production. Among these, MMP-1, MMP-2, and MMP-9 are particularly important for post-injury remodeling and have been studied as potential biomarkers of cardiovascular disease and outcomes after ACS.28
Regarding the correlation between Pn and sST2 levels, our study did not find significant differences between the LP and HP groups. However, some studies in the literature have reported that higher Pn levels are associated with increased sST2 serum levels, and these cases are linked to an unfavorable prognosis.11 Another biomarker studied was P-selectin. The comparative analysis of the two groups did not demonstrate a statistically significant correlation, but P-selectin levels were slightly higher in the HP group. Based on these results, the association between the two inflammatory markers suggests that endothelial dysfunction may be the main mechanism of atherosclerosis, potentially induced by Pn secretion. Similar results were published in the literature.29
The main limitation of this study is the small number of enrolled patients. The differences between our results and those in the literature may be attributed to the limited number of studies available on the topic, and the fact that most studies have been conducted on laboratory animals or focused on pathologies other than ACS. To the best of our knowledge, this is the first comprehensive study examining the correlation between Pn, inflammation, and cardiovascular outcomes in patients with ACS.
Our results suggest that patients with high Pn levels have an increased risk of developing major acute cardiovascular events. Owing to the more pronounced inflammatory process, coronary occlusion is often complete, leading to the onset of STEMI. As the condition progresses, patients may also develop heart failure or atrial fibrillation, which further increase mortality. Pn is a novel cardiac marker associated with a more pronounced inflammatory process, particularly during the acute phase. It is therefore useful in cardiovascular risk stratification due to its influence on atherosclerosis and the destabilization of coronary plaques.