Fulminant myocarditis is a rare condition with a high mortality rate, characterized by sudden-onset and rapid progressive cardiac dysfunction secondary to severe diffuse myocardial inflammation leading to hemodynamic instability.1,2,3,4,5 This life-threatening syndrome requires timely recognition and a life support-based comprehensive treatment regimen, including both immunomodulation therapy with glucocorticoids and intravenous immunoglobulin to modulate the aggressive immune response, and mechanical circulatory support (MCS) to restore circulation stability.2,5,6 MCS is used as bridge-to-recovery or bridge-to-transplantation therapy, and the decision to initiate MCS is dictated by the hemodynamic status of the patient, end-organ function, and the availability of MCS devices or extracorporeal life support.4
Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) implies mechanical circulatory support and simultaneous extracorporeal gas exchange. It is recommended as a short-term option in conditions causing cardiogenic shock,4,7,8,9 but it implies multiple life-threatening risks such as thrombosis, hemolysis, bleeding, infection of ECMO loops, impaired distal extremity perfusion, systemic inflammatory response syndrome, or left ventricular distension with secondary pulmonary edema.2,9 LV distension is the major limitation of VA-ECMO, yet there is no established consensus regarding the timing and the optimal strategy for LV unloading.9,10
The present paper aims to highlight the challenges encountered in the management of a pediatric patient with refractory cardiogenic shock, in a country with a low number of available compatible heart donors, who required a temporary salvage VA-ECMO intervention for hemodynamic stabilization as bridge-to-transplantation therapy until a heart transplantation was possible.
We present the case of a 15-year-old male adolescent, without any significant medical history, who was practicing martial arts. He presented an acute respiratory infection without any significant peculiarities. After 2 weeks, he presented to the emergency department with vomiting, abdominal pain, chest pain, and exercise intolerance. At physical examination, he presented hepatomegaly. The laboratory examination showed elevated inflammatory biomarkers and cardiac enzymes. ECG tracing revealed sinus rhythm, heart rate of 115 bpm, left axis deviation, PR interval of 140 ms, QRS duration of 80 ms, corrected QT interval of 420 ms, ST-segment depression and T-wave inversion in inferior and lateral leads. Chest radiography revealed marked cardiomegaly, and transthoracic echocardiography showed dilated cardiomyopathy with left ventricular ejection fraction (LVEF) of 20% and bilateral pleural effusion. Based on both clinical and paraclinical parameters, the suspicion of acute myocarditis was raised, and the patient was admitted to the pediatric cardiology department.
A definitive diagnosis of acute myocarditis was not established, given that performing a cardiac magnetic resonance imaging was not possible at that moment in our clinic. However, the recent history of respiratory tract infection, clinical features, and paraclinical findings of the patient were highly suggestive for infective myocarditis. To determine the etiology of myocarditis, swabs were collected, which revealed the presence of Hemophilus influenzae antigens in respiratory tract secretions. The patient was started on heart failure treatment with beta blockers, diuretics, vasodilators (angiotensin-converting enzyme inhibitors), and also required inotropic support with dobutamine and levosimendan. He received i.v. antibiotics (meropenem and vancomycin), i.v. antiviral treatment (acyclovir), i.v. immunoglobulins, glucocorticoids, and supplemental oxygen therapy. Owing to the poor evolution of the patient, a heart transplant was also taken into account. A cardiac catheterization was performed, which showed pulmonary hypertension due to a postcapillary mechanism, with low pulmonary vascular resistance of 1.7 uW/m2. Hence, the patient was transferred to the pediatric cardiac intensive care unit to be listed on the transplant list.
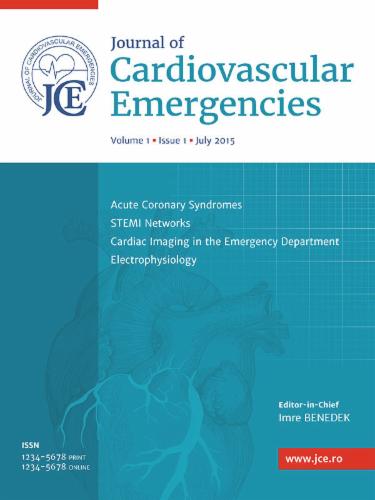
When the patient arrived to the intensive care unit he was in cardiogenic shock (orthopnea, marked hepatomegaly, hypotension, and renal failure). Transthoracic echocardiography showed a very low LVEF of 16%, decreased LV global longitudinal strain of −5.3%, right ventricular dysfunction, and aortic insufficiency (Figure 1A,B). The inotropic support was escalated, and adrenaline and milrinone were added to dobutamine. Vasopressor support with noradrenaline was also needed. However, the patient remained in a critical state, requiring mechanical circulatory support. A left ventricular assist device (LVAD) was not a suitable option because of the right heart dysfunction (poor contractility of the right ventricle, large tricuspid regurgitation); therefore, the patient received an extracorporeal membrane oxygenator (ECMO) by peripheric canulation (femoral artery and vein). However, severe congestion of the left heart was observed with pulmonary edema (Figure 1C).
Severe left ventricular dysfunction. A. Severely dilated LV with impaired systolic function (auto 2D quantification). B. Decreased LV global longitudinal strain (GLS) C. Chest radiograph revealing pulmonary edema.
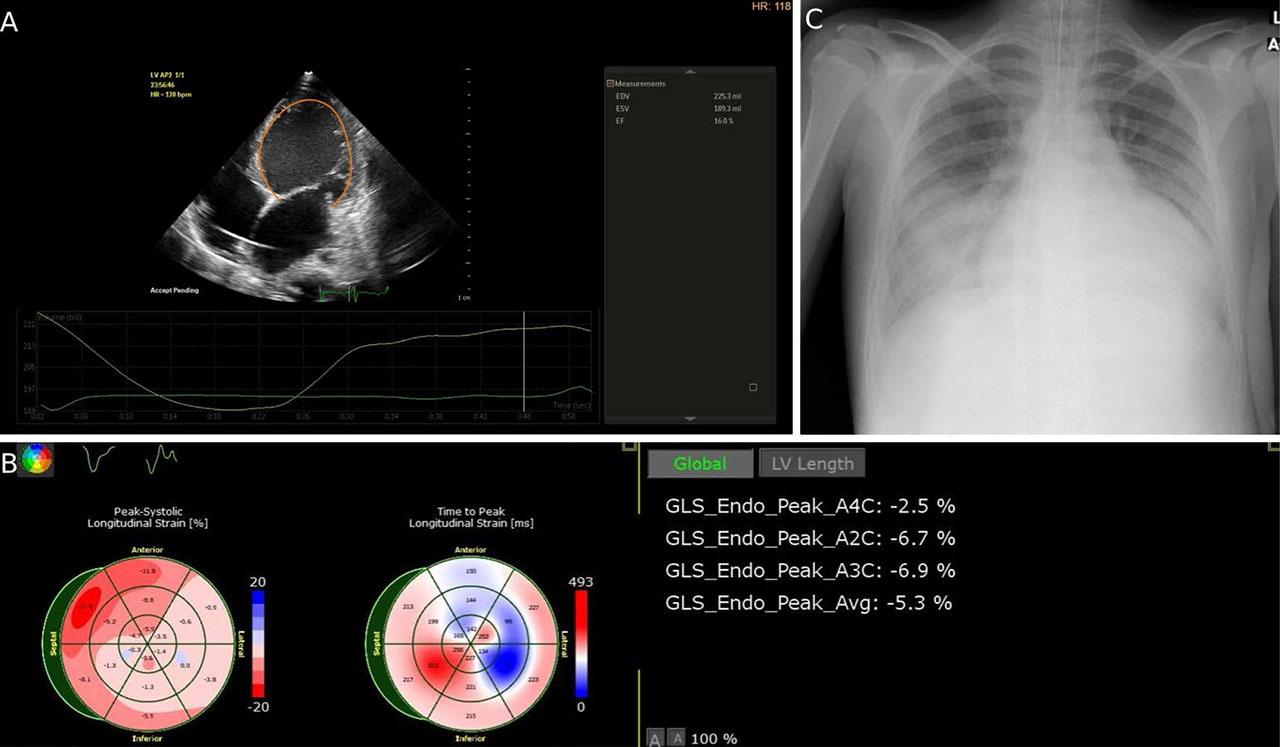
To decompress the left heart, the next day an echocardiography-guided transseptal puncture was performed through the interatrial septum, followed by balloon dilation of the interatrial communication, which did not manage to decrease the congestion of the left heart (Figure 2). After two more days of critical state of the patient, central cannulation was done (right atrium – ascending aorta) with another cannula for left atrial venting, and the patient remained with an open sternum. This led to a good decompression of the left heart. The patient was in a desperate situation, needing a heart transplant while being on VA-ECMO. After three more days, he underwent an orthotopic heart transplantation by bicaval technique.
Echocardiography-guided transseptal puncture through the interatrial septum. A. Transseptal needle. B. Balloon dilation of the interatrial communication. C. Doppler color-flow in atrial septal defect. D. Pulsed-wave Doppler revealing unrestrictive atrial septal defect.
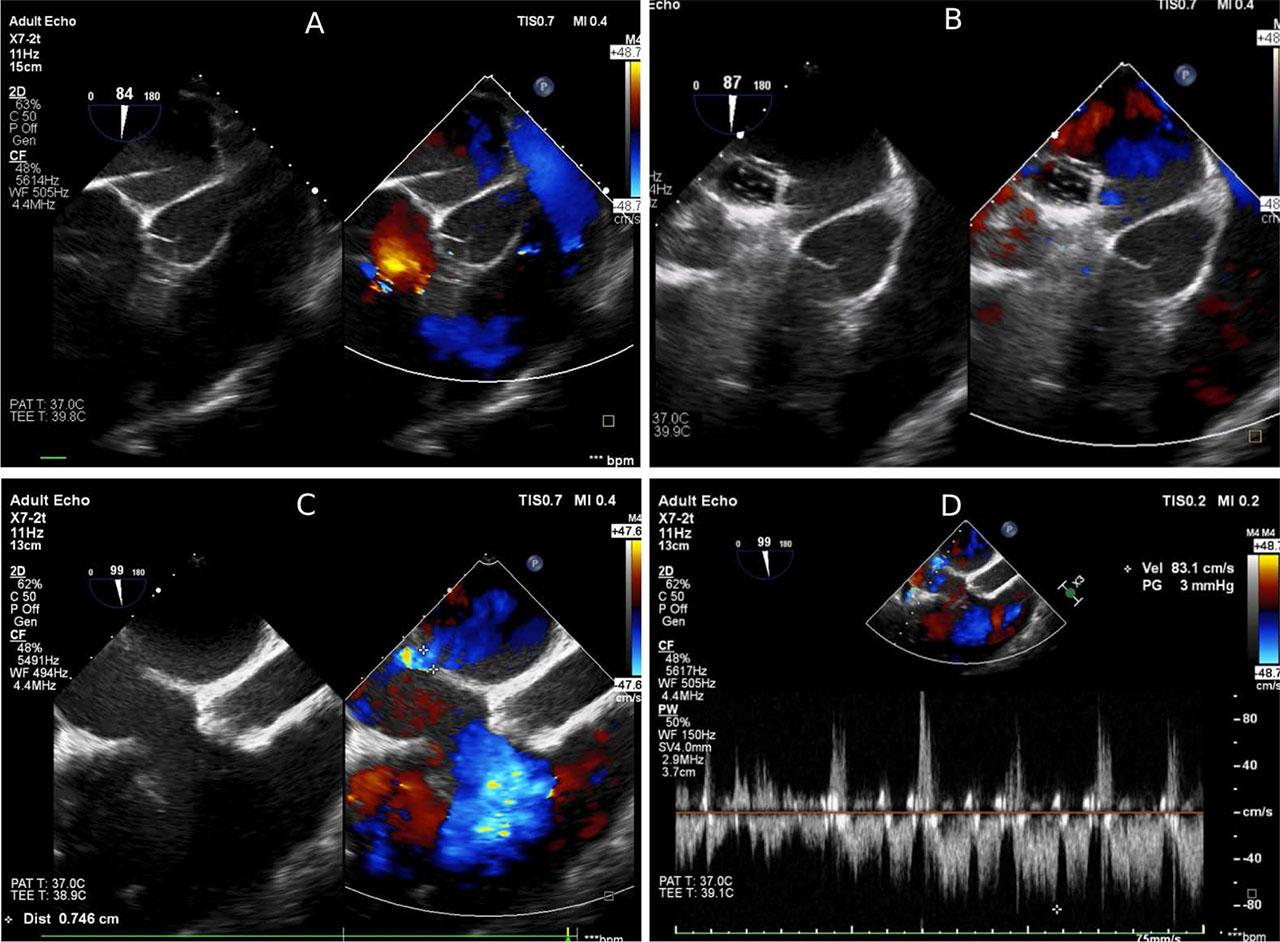
In the early follow-up, immediately after the heart transplant, he developed contractile dysfunction secondary to primary graft dysfunction (long ischemia time) and needed inotropic support (dobutamine 3 days, milrinone 16 days). The patient also developed new-onset neurological dysfunction with bulbar involvement: insomnia, apathy, muscle weakness, and swallowing and speaking dysfunction. Head computed tomography (CT) scan revealed hypodense image with hyperintense contour in the brain stem, interpreted as a bulbar ischemic injury (Figure 3A). He was treated with anticoagulants, vitamins and phenobarbital with slow, total remission of neurological symptoms. Moreover, Candida albicans colonization of the respiratory tract was revealed, and the patient received antifungal therapy with fluconazole.
Complications of VA-ECMO. A. Thromboembolic event: head CT scan revealing a bulbar ischemic stroke. B. Ultrasonic image of left inguinal seroma. C. Pelvic CT scan revealing a large, thin-walled left inguinal collection.
Two weeks after the heart transplant, a fluctuant collection became visible in the left inguinal region. Ultrasound and CT imaging revealed a large, thin-walled fluid cavity, suggestive for seroma (Figure 3B,C). It was drained by two needle puncture aspirations, but with recurrence. Hence, a surgical excision with hemostatic material was necessary, with total remission of the seroma afterwards. The patient also developed venous thrombosis at multiple sites (right jugular vein, left subclavian vein). In this context, thrombophilia testing was performed, which revealed heterozygote mutation for the MTHFR and PAI-1 genes. Anticoagulant treatment with heparin was initiated, which was later changed to enoxaparin and then to apixaban, with resolution of the thrombi.
The first endomyocardial biopsy performed 1 month after the heart transplant showed an ISHLT score of 0, and afterwards the patient was discharged and followed as an outpatient. The patient’s medical history timeline is presented in Figure 4.
Medical history timeline of the patient
In the absence of cardiovascular risk factors and the presence of a recent history of upper respiratory infection, the suspicion of myocarditis should be raised in young patients presenting with de novo acute heart failure.1 A sudden onset and a rapid progression into hemodynamic instability are highly suggestive for fulminant myocarditis.1,2
The management of fulminant myocarditis is challenging and implies a well-trained multidisciplinary team. Owing to the severe cardiovascular compromise, most patients require temporary MCS as bridge-to-recovery or bridge-to-transplantation therapy.1 The predictors of MCS requirement are cardiogenic shock, LVEF of less than 30%, and the presence of life-threatening arrhythmias.4,11
In terms of choosing MCS, our patient was not eligible for LVAD implantation given that he presented significant right ventricular systolo-diastolic dysfunction.12 Although the implantation of a biventricular assist device in pediatric patients has been reported to yield positive results,13 we excluded this option because of a lack of experience with these devices in our center. Moreover, this technique does not provide oxygenation (respiratory) support,14 and our patient needed additional oxygenation. Therefore, according to the guidelines of the European Society of Cardiology, peripheral VA-ECMO was considered a feasible short-term option.4,15
Although VA-ECMO effectively decreased right ventricular preload and peripheral venous congestion through systemic venous drainage,9,16 it had deleterious effects on the LV. Increased arterial flow provided by ECMO increased LV afterload. The LV with severely impaired systolic function could not overcome the ECMO-induced increased afterload, with the result of reduction of LV systolic ejection.9,16 This lead to LV volume distension and increased LV end-diastolic filling pressure, with a subsequent increase in myocardial wall stress and pulmonary edema.9,16,17 Despite the initiation of conservative LV unloading therapy with vasodilators, inotropic agents, and titration of ECMO flow,10,18 the patient remained in a critical state, requiring further strategies for LV and left atrium (LA) unloading.
To decompress the LA, first we performed an echocardiography-guided transseptal puncture followed by balloon dilation of the interatrial communication, which is a commonly used procedure in pediatric patients.9,16 However, the patient’s evolution was critical, therefore we performed central cannulation (right atrium – ascending aorta). We also placed a LA venting cannula connected to the venous circuit of VA-ECMO, and the chest was left open, all of these leading to a good decompression of the left heart.
The echocardiographic diagnostic criteria of LV distension in children are not standardized as in adults,16 and further studies on larger cohorts are needed to establish the most suitable echocardiographic parameters in pediatric patients.16,17 Eckhauser et al. showed in their study on peripheral VA-ECMO in pediatric patients aged between 2 and 12 years that in cases with depressed LV ejection fraction, the association of an E/A ratio higher than 2 and a deceleration time of early filling velocity lower than 150 ms might predict increased LA pressure and the need for decompression.16,17
Given that VA-ECMO was just a bridge-to-transplantation therapy, our patient was in desperate need for a heart transplantation in a country with a low number of donors. Fortunately, he received an orthotopic heart transplantation after 5 days on VA-ECMO. In the early follow-up he developed multiple complications, and the question arises whether they are the consequences of ECMO support, given that some of these complications are known to be associated with VA-ECMO.2,9,18
VA-ECMO is known to determine a prothrombotic inflammatory reaction and platelet damage secondary to the interaction of blood with the non-endothelialized surface of the ECMO circuit.9 This can lead to thromboembolic events and stroke.9 Furthermore, our patient associated positive heterozygote mutation for thrombophilia. Both of these situations could compete in the onset of the bulbar ischemic injury.
Moreover, recurrent inguinal seroma, which is a well-known complication of femoral cannulation, could be secondary to cannulation of the inferior limb needed in the first place for peripheral VA-ECMO.
VA-ECMO is a potential option for bridge-to-transplantation therapy in the temporary management of fulminant myocarditis with refractory cardiogenic shock in the absence of available compatible organ donors. One of the major limitations of VA-ECMO is the risk of LV distension and pulmonary edema. Timely and optimal LV unloading is crucial in the hemodynamic stabilization of the patient.