
The treatment of ventilator associated pneumonia (VAP) caused by organisms like Pseudomonas aeruginosa, and Acinetobacter spp can be challenging and is associated with increased morbidity, mortality and healthcare costs [1, 2]. With the rise of antibiotic-resistant organisms, often treatment with high-dose, broad-spectrum antibiotics are required [3,4,5,6]. However, commonly used antibiotics like B-lactams, colistin and aminoglycosides when administered intravenously, have reduced lung bioavailability as shown by reduced concentrations of lung epithelial to plasma concentrations [7,8,9]. Furthermore, prolonged use of systemic antimicrobial therapy like aminoglycosides and polymyxins are associated with significant side-effects like nephrotoxicity and ototoxicity in both adults and children [7, 10,11,12,13].
Delivery of antibiotics through inhalation or nebulization has significant advantages over systemic antibiotic therapy in treating lower respiratory tract infections. Nebulized antibiotics can achieve a high concentration in the lung tissue, effectively reducing the bacterial load of these pathogens while reducing the risk of systemic toxic effects [8, 9, 14, 15]. These drugs, when nebulized, have shown to have negligible to low trough plasma levels [14].
A recent meta-analysis in adults, investigating the use of inhaled colistin, in the treatment of VAP, found increased microbiological clearance but no significant difference in clinical outcomes [16]. Yet in a recent multicenter study in adults, nebulized amikacin reduced the risk of developing ventilator-associated pneumonia as compared with placebo [17]. While the Infectious Disease Society of America [18] supports the use of inhaled antibiotics in VAP, the position paper by the European Society of Clinical Microbiology does not support the use of inhaled antibiotics in ventilated adults [19].
The use of inhaled antibiotics in the management of children with VAP has rarely been described and the practice is varied among intensive care units. Hence, we conducted this systematic review and meta-analysis to determine the effect of inhaled antibiotics on (a) eradicating bacteria, (b) improving clinical outcomes (days of intubation, days in ICU), (c) reducing mortality and (d) risk of adverse effects in children treated for VAP.
The report follows the framework of the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) 2020 statement [20]. The protocol was registered in the National Institute for Health and Care Research International Prospective Register of Systematic Reviews (PROSPERO) with registration number CRD42024504982. We excluded studies with bronchiectasis and tracheostomy-dependent children as a comprehensive review has been recently published [21].
The clinical question under the PICO (Patient-Intervention-Comparator-Outcome) framework format was: For children with VAP, do inhaled antibiotics versus other treatment modalities improve the clinical, microbiological, and safety outcomes? The PICO questions are as follows:
Q: Does inhaled antibiotic treatment improve the clinical, microbiological and safety outcomes for children with VAP?
P: Children ≤ 18 years old with VAP
I: Inhaled antibiotics
C: Placebo or no therapy or other therapy (Intravenous and/or oral antibiotics)
O: Microbiological clearance, clinical success, clinical failure, duration of mechanical ventilation, duration of ICU stay, VAP and other-cause mortality, adverse effects
A comprehensive search of Web of Science, SCOPUS, MEDLINE Complete, AND CINAHL Complete online databases was done using the search terms (Inhaled OR aerosoli* OR nebuli*) AND (antibiotics OR antimicrobial) AND (pediatric OR pediatric OR child* OR neonate OR toddler OR adolescent) AND ventilator-associated pneumonia OR nosocomial infection OR hospital-acquired infection). Results were limited to articles published in English from 1st January 2014 to 30th June 2025. We also searched the ClinicalTrials.gov trials registry.
Studies that fulfilled the following criteria were included: 1) Study design: All observational and randomized trials, 2) Participants: All pediatric patients with VAP, 3) Trials using inhaled antibiotics as intervention were compared with placebo, with no treatment or other routes of antibiotic administration. Exclusion criteria were: 1) Adults >18 years old, 2) Tracheostomy-dependent children and bronchiectasis (including cystic fibrosis) and 3) Case reports and case series.
Two authors (SW, AMN) screened all the studies identified in the literature search by screening the titles, abstracts and full texts using EndNote Version 21. Any disagreements between the two reviewers were resolved by a third author (RZ).
One author extracted data and confirmed it with another. Using a pre-developed data extraction sheet in Microsoft Excel, the following data were extracted from included studies: the first author’s name, year of publication, country of origin, study design, and study population (inclusion/exclusion criteria).
The primary outcomes searched for were the (a) type of intervention (medication, dosage and duration), (b) clinical and microbiological outcomes, (c) duration of mechanical ventilation (MV), (d) duration of stay in ICU, (e)eradication of infection and (f) adverse effects including nephrotoxicity and bronchospasm, VAP-related mortality, all-cause mortality, and study limitations.
The risk of bias was assessed using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for observational studies and the Cochrane risk of bias tool for randomized controlled trials [22]. The STROBE statement contains a 22-item checklist that guides the reporting of observational studies to facilitate critical assessment and interpretation of results. The checklist is divided into sections: title, abstract, introduction, methods, results, discussion, and other information (funding). It was decided to have scores of 0 if the item was not fulfilled, a score of 1 if the item was fulfilled, and a score of NA (non-applicable) if the item was not applicable for the specific publication. The total number of items that fulfilled the criteria was added and divided by the total number of items for each study, respectively, and multiplied by 100 to get the results in percentages [23]. Randomized trials were assessed using the Revised Cochrane risk-of-bias tool for randomized trials (RoB 2) and the Review Manager 5.4 risk of bias tool. The tool assessed the following: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, selection of the reported result and overall bias [24]. Each item was graded to determine whether the studies were considered high, low, or unclear risk of bias. An appointed third reviewer (RZ) resolved any differences in the assessment process. Studies that had a score of <60% were considered as high risk and were excluded.
The meta-analysis was performed when sufficient data for each outcome were reported with a similar study design. All statistical analyses were performed using Review Manager (RevMan) version 5.3 (Cochrane Collaboration, London, UK). Data Estimation and Conversion for Meta-analysis (DECoMA) version 1.0 was used for data conversion. Continuous outcomes were presented as mean and standard deviation (SD). Dichotomous data were presented as risk ratios (RR) and 95% confidence interval (CI). Meta-analysis was performed using a fixed-effect model if there was no heterogeneity between studies or a random-effect model if there was significant heterogeneity. Statistical heterogeneity was measured through the I2 statistic and classified as low (I2 < 25%), moderate (I2 25–50%), or high (I2 > 50%).
Our initial search of the literature yielded a total of 343 searches: Web of Science (212), Scopus (60), MEDLINE Complete (53) and CINAHL Complete (17). We also gathered data from ClinicalTrials.gov for unpublished trials and found one study of interest which has not started recruitment yet [25]. This multicenter randomized controlled trial study will evaluate the benefit of a 3-to-7-day prophylactic course of inhaled colistin vs placebo among children with VAP. [25]. After screening through duplicated records, titles and abstracts, we retrieved 11 potentially relevant full-text articles for evaluation. Four articles were excluded for reasons stated in Figure 1. Finally, seven studies[26,27,28,29,30,31,32] were selected for inclusion in this review.
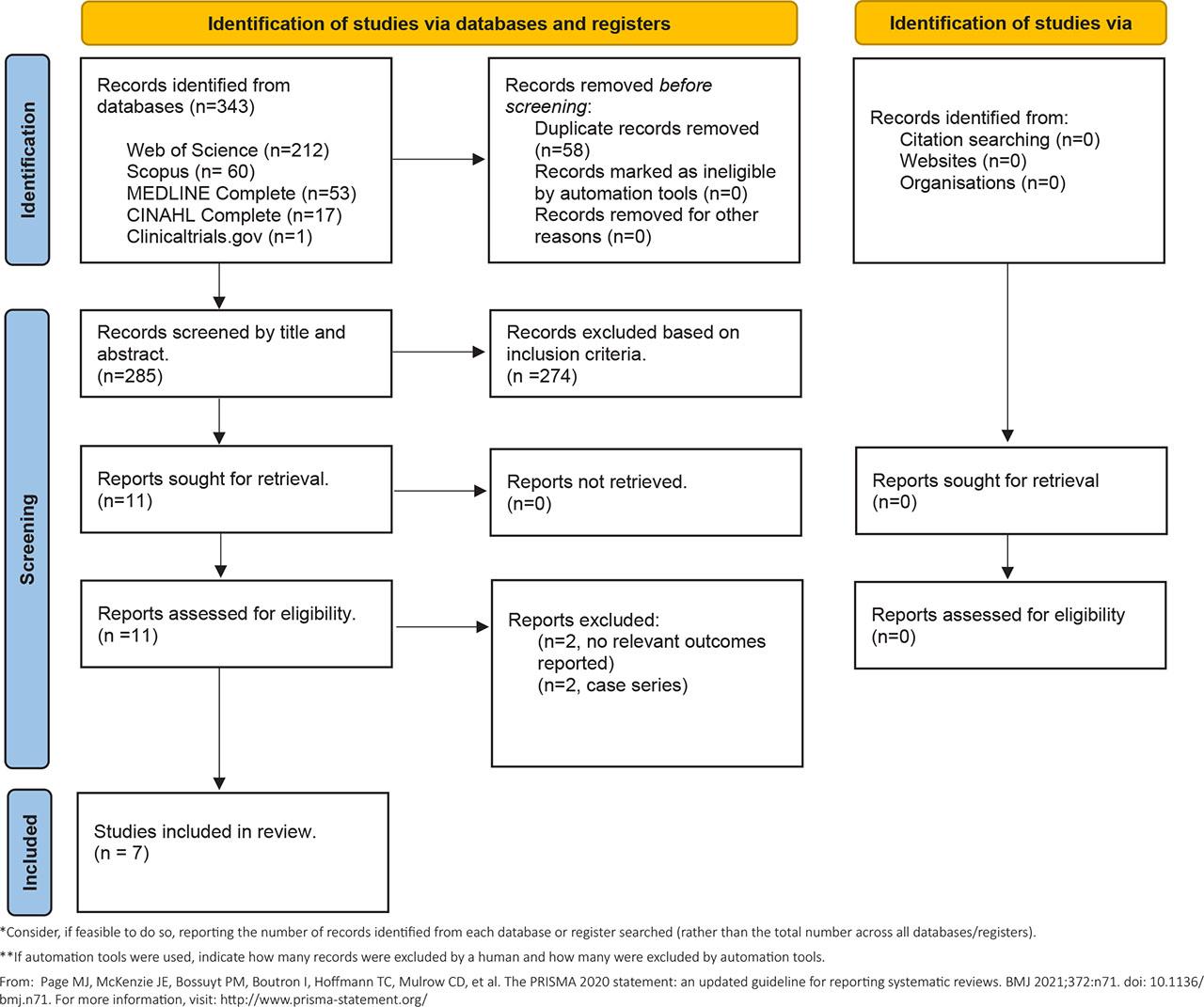
Preferred Items for Systematic Review and Meta-Analysis (PRISMA) screening process.
The definitions of clinical, microbiological outcomes and adverse events are shown in Table 1. The main characteristics and outcomes of the seven included trials are shown in Table 2 [26,27,28,29,30,31, 33]. One study was a retrospective cohort study [27], while two were retrospective case control studies [28, 33] and the remaining four were randomized controlled trials [26, 29,30,31]. Inhaled colistin was used in all six studies [27,28,29,30,31, 33]. while one study used inhaled amikacin [26]. The studies were from Ukraine, Iran, Turkey, Pakistan, India and Taiwan. None were sponsored by pharmaceutical companies. Four randomized controlled trials were included in meta-analysis [26, 29,30,31].
Definition of clinical, bacteriological and safety outcomes in the SEVEN included studies
| Study/year/country | Clinical outcome | Microbiological outcome | Adverse events |
|---|---|---|---|
| Levchenko 2023/Ukraine | Clinical parameters (body temperature and changes in respiratory parameters while on ventilator, including C dyn, PEEP and PIP), laboratory indices (blood oxygen saturation, leukocyte count), instrumental methods (CXR) Average duration of MV Average duration of ICU stays | Microbial load in sputum from endotracheal tubes on Day 3 and Day 5 | NA |
| Polat 2015/Turkey | Favourable clinical response: | Bacterial eradication – no growth of the causative microorganisms in the final culture | Nephrotoxicity – 50% or greater increased in serum creatinine level from the baseline and/or elevation of serum creatinine values beyond the estimated normal rage for the patient’s age group at any time during the tx Neurotoxicity |
| Hussain 2020/Pakistan | Clinical success was defined as | Eradication of the causative organism – no growth of the pathogen in the final culture of specimens during the entire hospitalization | Acute kidney injury (AKI) – increment in serum creatinine levels of ≥0.3mg/dl within 48 hours or 150–200% increase from baseline trough value |
| Khanababee 2024/Iran | Days of hospital stay | No microbiological outcomes measured | Nephrotoxicity |
| Bharathi 2022/India | Favorable outcome: | Bacterial eradication – final culture of specimens demonstrating no growth of the pathogen during the entire hospitalization | Nephrotoxicity – Change in serum creatinine levels |
| Sachev 2019/India | Clinical cure was defined as complete resolution of all signs and symptoms of pneumonia, with normalization of total leucocyte count and temperature at the end of CS therapy. Clinical failure was defined as persistent or worsening of presenting signs and symptoms. | Bacterial eradication, if no growth of the same pathogen as in the last culture of a respiratory specimen; | Renal impairment was defined |
| Kang 2014/Taiwan | NA | Cure was defined as at least three separate sputum culture that had no A.baumannii growth and each at least 1 day apart | Renal compromise – presence of decreased urine output ≤1ml/kg/hr, plasma creatinine level ≥1.5mg/dl and elevated BUN (ml/kg/hr) |
Supplementary Table S1 presents the full risk of bias assessments
Outcome measures (See Table 2)
Ventilator-associated pneumonia - main characteristics, outcomes and results of the included studies
| Author/Year/Country | Study design | Patients | Type of Nebulizer | Intervention/Placebo | Duration & dosage | Results reported |
|---|---|---|---|---|---|---|
| Inhaled + IV Abx VS IV Abx only, n=4 | ||||||
| Levchenko 2023/Ukraine | Randomized controlled trial, single-blind (Pilot study) | 20 (10/10) infants with VAP in ICU | Not stated | TR1 (n=10): inhaled AMK + systemic IV Abx TR2 (n=10): systemic IV Abx only | TR1: Inhaled AMK 500mg BD for x1/52 + IV MER (5 pt), IV CPZ-SBT (3 pt), IV AZM (2 pt) | A 2-fold increase in resistance and a significant increase in PIP values (22–23 cm H20) were found in the control group. Prolongation of the purulent-inflammatory process in the lungs compared to the patients administered inhaled amikacin in the early period of VAP. |
| Polat 2015/Turkey | Retrospective Cohort study | 50 (18/32) aged 1 month to 18 years critically ill children with VAP due to COS GNB in PICU | Vibrating Mesh Nebulizer | TR1 (n=18): inhaled + IV CS. | TR1: Inhaled CS administered concurrently >1yo: 75mg BD ≤1yo: 4mg/kg/dose BD + IV CS median dose 3.4mg/kg for a median duration of 14 days | No significant differences in favorable clinical response (P=0.362) and bacterial eradication (P=0.362) |
| Hussain 2020/Pakistan | Retrospective case control study | 32 (16/16) neonate with MDR-assoc VAP in NICU | Not stated | TR1 (n=16): Inhaled + IV CS | TR1: Inhaled CS 4mg/kg/dose BD for median duration 7.5 days + IV CS 2.5–5.0mg/kg/day 2–4 daily doses for median duration 4.5 days | Clinical success: Clinical cure was significant in TR1 group compared to TR2 group (56.3% vs 31.3%, P<0.05) while clinical improvement was not significantly different (P>0.999). |
| Khanababee 2024/Iran | Randomized controlled trial study | 80 (40/40) children aged 2–18 yrs old with MDR-assoc VAP in PICU (excluded patients who died [n =2]) | Not stated | TR1 (n=40): Inhaled CS + IV Abx | TR1: Inhaled CS 3 to 5mg/kg every 6 hours for a duration of 2 to 3 weeks (maintained at least 2 weeks) + IV Abx | Fever occurrence was significantly higher in the control group than in the colistin group (7.5% vs. 2.5%, P = 0.04). |
| Inhaled + IV Abx vs Inhaled NS + IV Abx, n=2 | ||||||
| Bharathi 2022/India | Randomized double-blinded controlled study | 98 (51/47) children with VAP due to GNB in the postoperative period following cardiac surgery for congenital heart disease in SICU | Breath-actuated jet nebulizer | TR 1 (n=51): Inhaled CS + IV Abx | TR 1: Inhaled CS 4mg/kg BD reconstituted in 4ml of sterile NS + IV Abx | Favorable clinical response was not significant (mean 37 vs 31 days, P=0.696) |
| Sachdev 2019/India | Open-label, pilot randomized controlled trial | 35 (16/19) children with MDR-asstd VAP in PICU | Vibrating mesh nebulizer (Aerogen, Ireland) | TR1 (n-16): Inhaled CS + IV antibiotics | TR1: Inhaled CS 500,000 IU reconstituted in 4ml of NS (TDS) + IV antibiotics | Clinical cure was higher in TR1 compared to TR,2 however was not significant (93.7% vs 73.6%, p=0.12) |
| Inhaled Abx only vs IV Abx only, n-1 | ||||||
| Kang 2014/Taiwan | Retrospective case control | 31 (8/23) preterm infants with VAP due to A.baumannii infection in NICU | Neb-easy nebulizer kit | TR1 (n=8°): Inhaled CS | TR1: Inhaled CS 33.4mg BD with average 9.1 days (range 4-22 days) with 4 pts received IV antimicrobial concurrently | All pre-term infants in both treatment groups were reported to be cured with A.baumannii eradicated from airway secretions and discharged. |
TR1: Treatment regimen 1 (main); TR2: Treatment regimen 2 (control); VAP: Ventilator-associated pneumonia; COS GNB: Colistin-organism sensitive gram negative bacteria; MDR: Multi-drug resistant; SICU: Surgical Intensive Care Unit; NICU: Neonatal intensive care unit; OD: Once daily; BD: Twice daily; Abx: Antibiotic; IT Abx: Intrathecal Antibiotic; 1yo: 1 year old; ; MV: Mechanical ventilation; Pt: patient; Tx: treatment; Pa: pseudomonas aeruginosa; H.influenza: Haemophilus influenza; A.baumannii: Acinetobactor baumannii; BAL: Bronchoalveolar lavage; PO: Per oral; BBS: Blind bronchial sampling.
AMK: Amikacin; AZM: Aztreonam; CPZ: Cefoperazone; AMP: Ampicillin; SBT: Sulbactam; CAZ: Ceftazidime; CEF: Cefepime; CLI: Clindamycin; CS: Colistin; MER: Meropenam; VAN: Vancomycin; CIP: Ciprofloxacin; PIP-TAZ: Piperacillin-Tazobactam; LZD: Linezolid; TIG: Tigecyclin
Details obtained from personal communication with the authors.
Standard deviation not stated
Four studies looked at the combination of inhaled and intravenous antibiotics versus intravenous antibiotics only [26,27,28,29]. Two were retrospective [27, 28] while two were a randomized controlled study [26, 29]. Results are summarized in Table 2.
Two retrospective studies investigated the use of inhaled colistin in children with ventilator-associated pneumonia (VAP) in the NICU and ICU [27, 28]. Two studies included children under one-year-old, and inhaled colistin was administered at 4mg/kg BD [27, 28]. In the study that included children over one-year-old too, inhaled colistin was administered at 75mg BD [27]. Another study only included children aged 2–18 years old and administered inhaled colistin 3 to 5mg/kg every 6 hours for a duration of two to three weeks [29].
Polat et al. showed a significant reduction in time to bacterial eradication (TBE) in the study group compared to the control group (3 vs 6 median days, p<0.001) [27]. However, there were no significant differences in clinical response, bacterial eradication and mortality (VAP related mortality and other-cause mortality). Conversely, Hussain et al. showed that the use of inhaled and IV antibiotics resulted in significantly more cases with clinical cure (9 vs 5 cases, p<0.05) and eradication of infection (68.8% vs 43.8%, p<0.05) [28]. However, clinical improvement was similar (4 vs 4 cases, p>0.999). As for mortality, there was a trend towards reduced mortality in those with adjunct inhaled antibiotics: VAP (12.5% vs 31.3%, p =0.08), overall mortality (25% vs 73.8%, p=0.06).
A randomized controlled study recently published in 2024 investigated the use of inhaled colistin in ICU [29]. Khanababee et al. showed fever occurrence was higher in control group compared to study group (7.5% vs 2.5%, P =0.04). However, other outcomes measured (MV and hospital stay days, mortality, infective blood parameters, fever duration, were not significant). The types of co-administered intravenous antibiotics which were not described in the study. Microbiological outcomes were also not measured.
Worth mentioning here is another randomized, controlled, single-blind (pilot) study which compared the administration of adjunctive inhaled antibiotics (amikacin 500mg BD) for one week combined with IV antibiotics versus IV antibiotics only, in mechanically ventilated infants with VAP [26]. This study investigated the respiratory parameters while on a ventilator, MV and ICU stay duration, and microbial load in the sputum pre-and post-treatment. A 2-fold increase in resistant organisms and a significant increase in peak inspiratory pressure (PIP) values was found in the control group. There was a significant reduction in early apoptotic and necrosis of circulating leukocytes in the study group compared to the control group. The average (range) duration of MV was also significantly reduced in the study group compared to the control group 6 (5–10) vs 7 (6–12) days, p<0.05, while the duration of stay in the ICU was not significant 7 (6–12) vs 8 (7–14) days, p=0.20 (personal communication in author) [26]. Levchenko et al. also found a significant reduction in microbial load in the endotracheal tube cultures of the study group on the third day of antibiotic therapy (log (3.59±0.32) CFU/ml) compared to the control group (log (5.49±0.27) CFU/ml) (p<0.001) and the results were reproduced on the fifth day as well. This study did not report on bacterial eradication nor adverse events [26].
There were two studies that used Inhaled NS in the control group [30]. A prospective, randomized, double-blind, controlled study compared the concomitant use of inhaled colistin (4mg/kg BD) with IV antibiotics (n=51) and Inhaled NS with IV antibiotics (n=47) in children with VAP in the postoperative period following cardiac surgery in a surgical ICU. The study group had a significant decrease in the duration of MV (11.2 vs 18.1 days, p=0.002), postoperative ICU stay (14.04 vs 22.3 days, p=0.004), and total hospital stay (17.6 vs 26.2 days, p=0.005) compared to the control group. However, there was no significant difference in favorable clinical response (37 vs 31, p=0.696), bacteriological outcome (80.4% vs 68.1%, p=0.16). There was a trend to reduced risk of VAP-related mortality (3.9% vs 14.7%, p=0.07) but not significant other-cause mortality (p=0.64). Adverse effects of inhaled colistin were not seen in both groups despite not using prophylactic B2 agonists. Regarding nephrotoxicity, differences in serum creatinine levels were insignificant between the two groups (mean 0.18 vs 0.12, p=0.081). In another study by Sachdev et al., who performed a randomized controlled trial in 35 children with inhaled colistin 500,000IU given 8hrly together with IV antibiotics, found no significant difference in outcomes (bacterial eradication, duration of MV and ICU stay, mortality, clinical cure).
Only one study used inhaled antibiotics only in the intervention group [33]. This retrospective case-control looked at the role of inhaled colistin monotherapy for VAP of Acinetobacter baumannii in premature infants. They recruited 31 preterm infants in which eight patients were given inhaled colistin 33.4mg BD (equivalent to 1 million IU), and 23 patients received IV antibiotics only. Four of the eight patients who received inhaled colistin initially received IV antibiotics but did not improve; hence, inhaled colistin was started. All preterm infants in both treatment groups were reported to be microbiologically cured with Acinetobacter baumannii eradicated (at least three negative sputum cultures and each at least one day apart) from airway secretions and discharged. This study found that inhaled colistin was safe to use in prematurity as no clinical or renal function abnormalities were noted. None of the patients had adverse events from the inhaled colistin therapy despite not using bronchodilators.
Hussain et al. showed acute kidney injury (AKI) was more prevalent in the control group compared to the study group (31.3% vs 6.25%, p<0.05); this could be due to the longer duration of IV colistin given in the control group compared to study group (12.5 vs 7.5 days) [28]. Polat et al. showed that one child developed nephrotoxicity in the control group [27]. However, this patient also received concomitant vancomycin and radiocontrast agents before IV colistin. Bharathi et al found no significant differences in serum creatinine levels between the two groups (mean 0.18 vs 0.12, p=0.081)[30]. Khanababee et al. found no significant difference in nephrotoxicity or serum creatinine levels between two groups despite the high dose (3–5 mg/kg inhaled every 6 hrs) and prolonged use (2–3 weeks) of inhaled colistin [29]. Sachdev et al found no significance difference in renal impairment [31]. The study in premature infants also found no clinical or renal function abnormalities [33].
Bronchoconstriction was an adverse effect of inhaled colistin therapy, as observed in Polat et al., where three patients experienced bronchoconstriction and desaturation after receiving the first dose. However, this problem was alleviated with B2-agonist and well tolerated after that [27]. In contrast, Hussain et al, Bharati et al and Khanababee et al did not report any bronchoconstriction, although it was not evident in the study whether all patients were routinely prescribed B2-agonists before inhaled antibiotics [28,29,30]. Sachdev et al pre-treated patients with hyper-reactive airways with inhaled salbutamol. They found no increased risk of bronchospasm in the treatment group [31]. The study by Levchenko did not comment on side-effects [26]. In premature infants, no bronchospasm was noted despite not using bronchodilators [33].
Polat et al. and Khanababee et al. did not report any cases of neurotoxicity. In contrast, Hussain et al. reported three cases when comparing both treatment arms (one in the study group versus two in the control group, p<0.782).
Finally, in the study that used inhaled colistin in premature infants, no clinical or renal function abnormalities were noted. None of the patients had adverse events from the inhaled colistin therapy despite not using bronchodilators [33].
We included four randomized controlled studies [27,28,29, 31] in the meta-analysis. However, not all of the outcomes could be included into the meta-analysis due to differential reporting or lack of reporting standard deviation or range. Levchenko et al did not report on clinical success, bacterial eradication, nor mortality, while Khanababee et al did not report on clinical success or bacterial eradication. Bharathi et al, did not provide standard deviation for analysis of MV, ICU stay, and lacked details regarding adverse events. We finally decided to combine the control arms of IV antibiotics with and without inhaled NS when analyzing MV, ICU stay, mortality, and nephrotoxicity, as inhaled NS was considered a placebo.
We examined the following clinical outcomes: clinical success (cure or improvement), eradication of bacteria, duration of MV, nephrotoxicity, and other-cause mortality, as shown in Figure 2A–E.
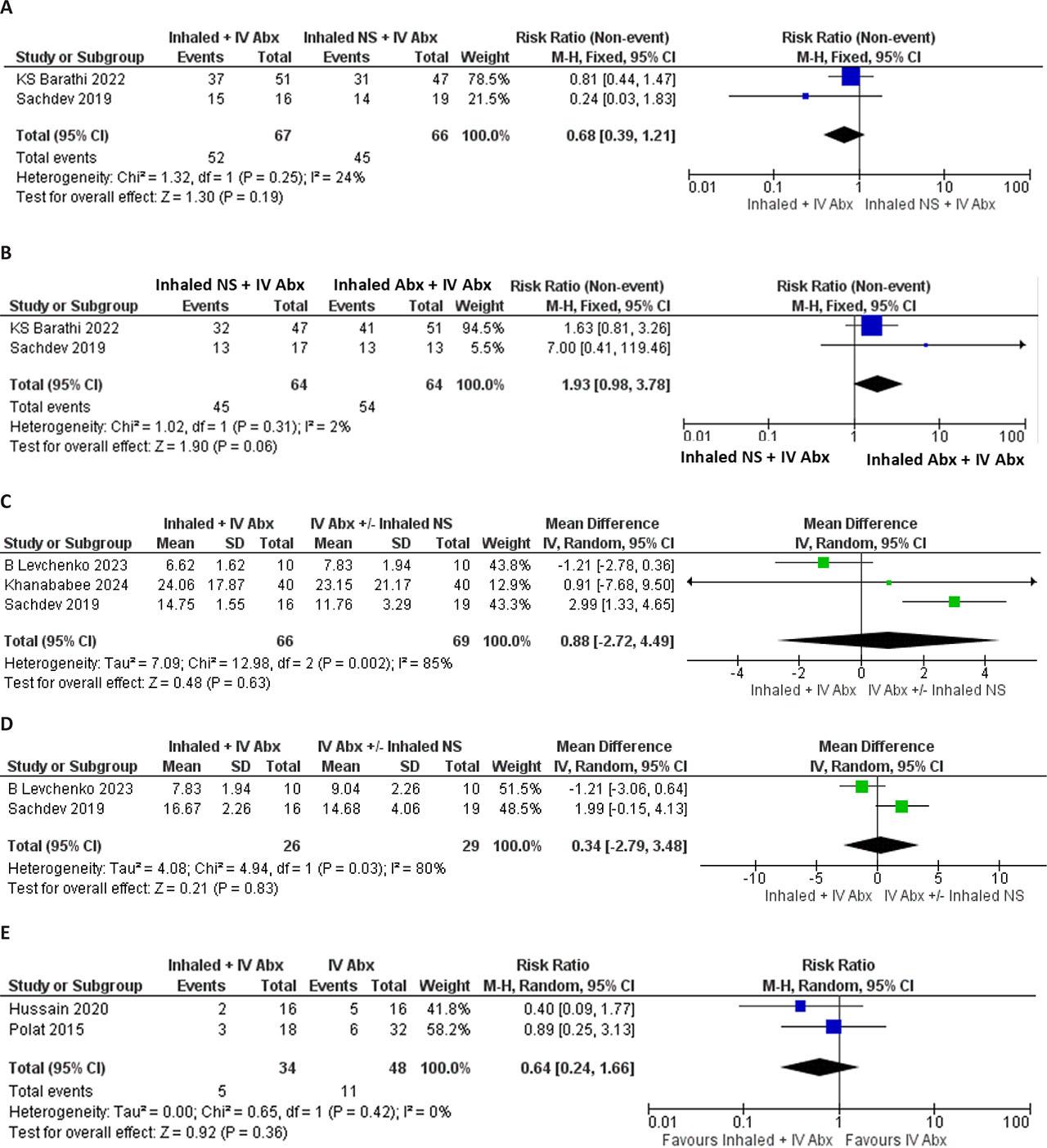
Forest plot for clinical outcomes. (A) Clinical success, (B) Bacterial Eradication (C) Duration of Mechanical Ventilation (D) Duration of intensive care unit (ICU) stay (E) Mortality
Analyses of studies from Bharati et al. and Sachev et al. found no significant improvement in clinical success (RR 0.68, 95% CI 0.39–1.21; p = 0.19; I2 = 24%) in the groups with inhaled + IV antibiotics (Figure 2A).
Similarly, studies by Bharati et al. and Sachev et al. found that the likelihood of eradicating bacteria in the combined inhaled + IV antibiotics group (RR 1.93, 95%CI 0.97,3.78; p=0.06, I2 = 2%) was possibly higher than with IV antibiotics +Inhaled NS alone; however, the difference did not achieve statistical significance. Figure 2B
However, the combination of inhaled + intravenous antibiotics compared to intravenous antibiotics +/− inhaled NS had no significant reduction in the duration of MV (MD 0.88 days, 95% CI −2.72, 4.49; p=0.63, I2 = 85%) and ICU stay (MD 0.34[−2.79,3.40]; p=0.83, I2 = 80%) (Figure 2C and 2D respectively).
As for VAP-related mortality (RR 0.64, 95% CI 0.24, 1.66; p=0.36, I2=0%) and other-cause mortality (RR 0.91, 95% CI 0.36, 2.33; p=0.85, I2=40%), both outcomes were not significantly different between the two treatment groups (Figure 2E).
Inhaled + IV antibiotics therapy was associated with a non-significant reduced risk of nephrotoxicity (RR 0.20, 95% CI 0.08, 1.14; p=0.08, I2=0%) (Figure 3).

Forest plot for nephrotoxicity
This systematic review aimed to determine the efficacy of inhaled antibiotics in children with VAP, associated with gram-negative bacteria (GNB) in children. We found seven studies involving neonates and children and the commonest antibiotic used was inhaled colistin, which was included in six trials [27,28,29,30,31, 33], while one trial [26] used inhaled amikacin. Four studies used Inhaled and IV antibiotics versus IV antibiotics alone while the other two used IV antibiotics with inhaled normal saline (NS) as a placebo. The meta-analysis included four randomized controlled studies, however due to difference in reporting outcomes, majority of the analysis was on two studies. We found no significant improvement in clinical success and no reduction in bacterial eradication, mechanical ventilation, ICU stay nor mortality. Importantly, there was no significant increase in adverse effects.
In the meta-analyses, adjunctive inhaled antibiotics did not significantly shorten the duration of MV nor ICU stay. Others have shown a reduction in MV and ICU stay, by about 4 days each, albeit both of these studies were retrospective [27, 28]. Bharathi et al. also demonstrated significant reduction in duration of MV by 7 days, postoperative ICU days by 8 days and total hospitalization by 9 days, in the group receiving inhaled and intravenous antibiotics compared to the control group [30]. However, we could not include Bharathi’s study into the meta-analyses as standard deviations were not reported in the paper. Considering that Bharathi et al had 98 patients in their study, exclusion of this may have affected our finding. Also to note was high heterogeneity in both these analyses. This may have resulted in our negative outcome. Reducing duration of invasive ventilation and ICU stay has both clinical and financial implications [34]. There may be other factors that influence duration of ICU stay like central line infections, renal failure, tracheostomy, need for external ventricular shunts and surgical procedures [35, 36]. Only half of the studies compared the underlying illness of patients, which ultimately may be a confounding factor associated with the duration of ICU stay and/or mechanical ventilation [27, 28, 31, 32]. In adults, two systematic reviews by Qin et al (13 studies involving 1733 patients, looking at adjunctive use of Amikacin) and Zampieri et al (12 studies involving 885 patients, looking at both adjunctive and substitutive use of amikacin, colistin and tobramycin) showed no significant effect on duration of MV and ICU stay, although there was high heterogeneity in both these outcomes [11, 37]. Adults have significant co-morbidities like diabetes and poor cardiac function that may affect both the duration of MV and ICU stay too [38, 39].
Our meta-analyses involving studies from Bharati et al [30] and Sachdev et al [31] found no significant increase in clinical success. Clinical success was similarly defined in the study by Polat et al and Hussain et al [27, 28], of whom only Hussain et al found a significant improvement in clinical cure. Hussain differed from the others as he studied neonates in the NICU, while the others studies patients post cardiac surgery or in the PICU with various illnesses. This is probably the reason for the difference in findings. As mentioned earlier, underlying disease may potentially influence clinical outcomes. In adults, the reviews by Qin and Zhang found differing results in clinical responses: RR 1.23 (95% CI 1.13–1.34) and OR 1.39 (95% CI 0.87–2.20) [11, 16].
As for bacterial eradication, the meta-analyses showed a trend to increased microbiological clearance (RR 1.93, p=0.06), although it did not achieve statistical significance. In the retrospective studies not included in this meta-analysis, both Polat el al and Hussain et al found bacterial eradication was increased when inhaled colistin was used [27, 28]. Similarly, Levchenko et al. found a significant decrease of microbial load in sputum from the endotracheal tubes on the third and fifth day in the inhaled amikacin + IV antibiotics group compared to IV antibiotics only group [26]. The lack of significance in bacterial clearance across most studies could be due to the variation in duration of therapy, as most of the studies continued inhaled antibiotics as long as IV antibiotics were on board [27, 30]. However, Hussain et al., who continued inhaled antibiotic treatment alone for at least 3 days after the cessation of IV antibiotics, found significant bacterial eradication [28]. Results on bacterial eradication could also be affected by when the culture was taken or analyzed e.g. early in the course of treatment versus later after treatment, whereby recrudescence of bacteria is more likely to occur. Interestingly, inhaled colistin monotherapy was used for VAP of Acinetobacter baumannii in premature infants, and all preterm infants reported to be microbiologically cured (at least three negative sputum cultures and each at least one day apart) [33]. In children, there are no head-to-head studies between colistin and amikacin. In adults, the review by Sella et al (11 studies involving 1472 patients, looking at the adjunctive use various inhaled antibiotics (amikacin, polymyxin B, colistin and tobramycin), found increased bacterial eradication, with OR 2.63(95% CI 1.36–5.09) [40]. They also found that the effect size on bacterial clearance was higher with colistin compared to amikacin (OR 2.21 [95%CI 1.25–3.92] vs RR 1.51[95%CI 1.35–1.69]) respectively [40].
As for VAP-related mortality and other-cause mortality, we decided to combine the results of studies which included inhaled NS as this is a placebo, and there was low heterogeneity. Three studies were analyzed and there were no significant differences between the treatment and control groups. This is probably due to the small numbers of children with mortality in these studies. In adults, effect sizes for pneumonia-cause of mortality by Qin et al (for amikacin) and Valachis et al (both adjunctive and substitutive use of colistin) were RR 1.12 (95% CI 0.82–1.52) and OR 0.58 (95% CI 0.34–0.96) respectively [11, 41]. As for all-cause mortality, the effect size for amikacin by Qin et al and colistin by Vardakas et al (13 studies involving 1135 patients, adjunctive use of colistin) were not significant at RR 1.17 (0.98–1.50) and RR 0.94 (0.81–1.08) respectively [11, 42].
Our negative meta-analysis suggests that studies should focus on the use of inhaled antibiotics on specific populations, such as premature infants alone, solid organ transplant recipients, or post-cardiac surgery, who have an increased risk for prolonged IMV, hence at risk of developing MDR strains, which may result in more positive findings. Furthermore, the use of inhaled antibiotics for prevention rather than for treatment may be a more effective strategy [25, 43].
Expert opinion recommends that inhaled colistin + systemic colistin may be considered for VAP caused by XDR GNB especially when the pathogen is only sensitive to colistin and if there is treatment failure with systemic colistin alone [44]. We recommend that the dose for adjunctive inhaled colistin in infants and children is 4mg/kg BD, as observed in the two studies in infants [27, 28] and one study in children [30]. In preterm infants with VAP due to A. baumannii, inhaled colistin was administered at 1.0 M IU BD (33.33mg) [33]. This is also in line with the recommendation of the Children’s Antimicrobial Management Program (ChAMP) Monograph by Perth Children Hospital [45].
The duration of inhaled colistin observed among the four studies on VAP varied greatly [27, 28, 30, 33]. We found that cessation of combination treatment following resolution of clinical signs and symptoms did not achieve significant bacterial clearance based on three studies[27, 30, 31]. , while continuing inhaled antibiotics alone after combination therapy for a minimum of three days resulted in bacterial clearance, as shown in Hussain et al. [28]. Hence, we recommend that duration of inhaled antibiotics should be continued longer than systemic antibiotics to achieve bacterial clearance.
Bronchospasm has been reported to occur in patients with and without asthma [46]. However, our review showed that this can be prevented by using a B2-agonist, without the need to discontinue the drug [27]. This review also did not find consistent reporting of bronchospasm as an adverse event. Even in children with CF, adverse events from the use of inhaled antibiotics are rarely reported [47]. This shows that bronchospasm from the use of inhaled antibiotics is not common in young children. This is different in adults, whereby bronchospasm seems to be more common with risks of RR 2.55 (95%CI 1.40–4.66) and OR 5.19 (95% CI 1.05–25.52) [11, 16]. Use of preservative free antibiotics do have a lower risk for bronchospasm [48].
The common adverse reactions described with intravenous colistin treatment are nephrotoxicity and neurotoxicity due to its narrow therapeutic index [49]. As for nephrotoxicity, this meta-analysis and the other studies [27, 28, 30, 33], which were not included in the quantitative analysis, observed that this risk was not significantly different between the study and control groups. Even in premature infants, the use of colistin has been reported to be effective [50, 51] and safe [51,52,53]. Given that colistin is negatively charged at human physiological pH, the negative charge of the alveolar basement membrane likely contributes to the slow systemic passage of colistin into the systemic circulation [54]. Colistin-associated nephrotoxicity can still occur in up to 10% of the cases, as shown in a review involving 104 critically ill children with normal renal function and colistin dosage administered at 5mg/kg per day in three divided doses [55]. Conversely, studies in adults have found reduced nephrotoxicity with the use of inhaled antibiotics[56]. Nephrotoxicity and neurotoxicity associated with intravenous colistin are related to the amount of daily maintenance dose and not to the loading or cumulative dose and are usually reversible [57]. Higher or excessive doses of colistin (>5mg/kg ideal body weight/day) are associated with an increased risk of nephrotoxicity and often result from the use of actual body weight in obese patients [58]. Nonetheless, careful surveillance and the use of preventative strategies for antibiotic related toxicity (such as nephrotoxicity and ototoxicity) are still essential to avoid possible toxicity [59].
With the use of nebulized antibiotics, antibiotic resistance is a significant concern. This was not reported in any of our included studies. In a small study involving children with tracheostomy, one out of six developed microbial resistance, after a median duration of 74 days of inhaled antibiotics. [60]. In adults with VAP, the systematic review showed reduced emergence of resistant bacteria strains (RR 0.18, 95% CI 0.05–0.64) [15]. A systematic review (19 studies) on adults with stable NCFB revealed a higher risk of isolating resistant organisms with inhaled antibiotic treatment [61]. The pooled risk ratio was 1.86 (95% CI, 1.51–2.30; p<0.001, I2:6%), and resistance increased regardless of which inhaled antibiotic was used (p=0.20, I2: 35%) [61]. However, a review that explored the use of inhaled tobramycin, colistin and gentamicin in adults with NCFB did not demonstrate any significant emergence of antimicrobial isolates in sputum, and any increase in minimum inhibitory concentrations (MIC) was transient with a return to baseline after discontinuation of treatment [55]. Although antibiotic resistance is a concern, evidence shows that inhaled antibiotics could eradicate existing multidrug-resistant organisms (MDRO) in intubated patients and reduce the pressure for the selection of new resistant organisms whilst reducing the use of systemic antibiotics [62].
One should be wary of other essential aspects of nebulized therapy e.g. type of device used and administration techniques, to improve drug deposition balanced with safety and patient comfort [8, 63]. An ultrasonic mesh nebulizer, placed in the inspiratory limb 15-40 cm before the Y-piece and removing the heat and moisture exchange during therapy, is important. Use of a smooth inner surface tubing will also improve drug deposition [8]. Placing a filter in the expiratory limb, between the ventilator during nebulization, which should be changed after treatment, will prevent expiratory limb obstruction.
The limited number of studies with small sample sizes and few randomized controlled trials in children with VAP will impact the generalizability and reliability of the findings. Furthermore, the use of inhaled antibiotics in various diseases and populations would have impacted the outcome. Our meta-analysis on the four RCTs still only included a maximum of three studies, with some analyses showing significant heterogeneity between these studies.
Using inhaled antibiotics with systemic antibiotics in children with ventilator-associated pneumonia did not result in statistically significant outcomes. We observed a minor, non-significant decrease in days on bacterial eradication, but no notable changes in clinical outcomes like MV, ICU stay, clinical success, or mortality. There was no increase in side effects, such as bronchospasm or nephrotoxicity, however close monitoring of each individual patient is still required.
Larger randomized studies on specific populations are needed to confirm that inhaled antibiotics improve outcomes for children with VAP. Studies directly comparing amikacin and colistin are also important to determine if colistin is the best choice.