
Glomus tumors are rare, benign mesenchymal neoplasms that arise from the glomus bodies — specialized arteriovenous shunts located in the dermis responsible for thermoregulation. (1) They are commonly found in the distal extremities, particularly in the subungual area, accounting for approximately 2% of all soft tissue tumors. (2) Gastric glomus tumors, on the other hand, constitute less than 1% of all gastric neoplasms and are typically found in the gastric antrum. (3)
The preoperative diagnosis of gastric glomangioma remains a major challenge. The absence of unique clinical or radiological features makes it difficult to differentiate these tumors from gastrointestinal stromal tumors (GISTs), gastric neuroendocrine tumors (NETs), leiomyomas, or schwannomas.
Immunohistochemical staining of resected or biopsied tissue is therefore crucial for definitive diagnosis, as it enables the identification of glomus cell features. We report a case of gastric glomangioma, highlighting the diagnostic workup (clinical presentation, imaging, and histopathological assessment), surgical decision-making, and an updated framework for post-resection surveillance.
A 51-year-old female presented with two years of persistent epigastric burning, anorexia, and weight loss. Her history included hypertension, treated pituitary microprolactinoma, hypothyroidism, and major depressive disorder, the latter likely contributing to her symptoms.
Persistent symptoms and suspected gastric pathology led to OGD, revealing a smooth submucosal bulge in the distal gastric body and pyloric region. EUS showed a 1.8 × 2.4 cm hypoechoic lesion in the muscularis propria. EUS-guided FNB was performed.
The prepared cell block was adequate for cytologic evaluation and a limited immunohistochemical analysis. It revealed a cluster of epithelioid cells with round nuclei and moderate amounts of cytoplasm. However, it was not sufficient to establish a specific diagnosis. Immunohistochemical studies ruled out GIST (negative for CD117 and DOG1), leiomyoma (negative for desmin), and schwannoma (negative for S100). GGT-specific markers such as SMA, vimentin, and synaptophysin were not applied at this point due to tissue exhaustion and low preoperative suspicion of this diagnosis.
Contrast-enhanced CT of the abdomen with arterial and portal venous phase acquisition demonstrated a round, circumscribed mass along the greater curvature at the junction of the gastric body and antrum, measuring approximately 2 cm. The lesion showed avid arterial-phase enhancement with persistent venous-phase enhancement, suggestive of a hypervascular submucosal neoplasm. No lymphadenopathy or distant metastasis was identified [Figure 1]. CT of the thorax showed no pulmonary nodules, masses, or mediastinal lymphadenopathy to suggest metastatic spread.
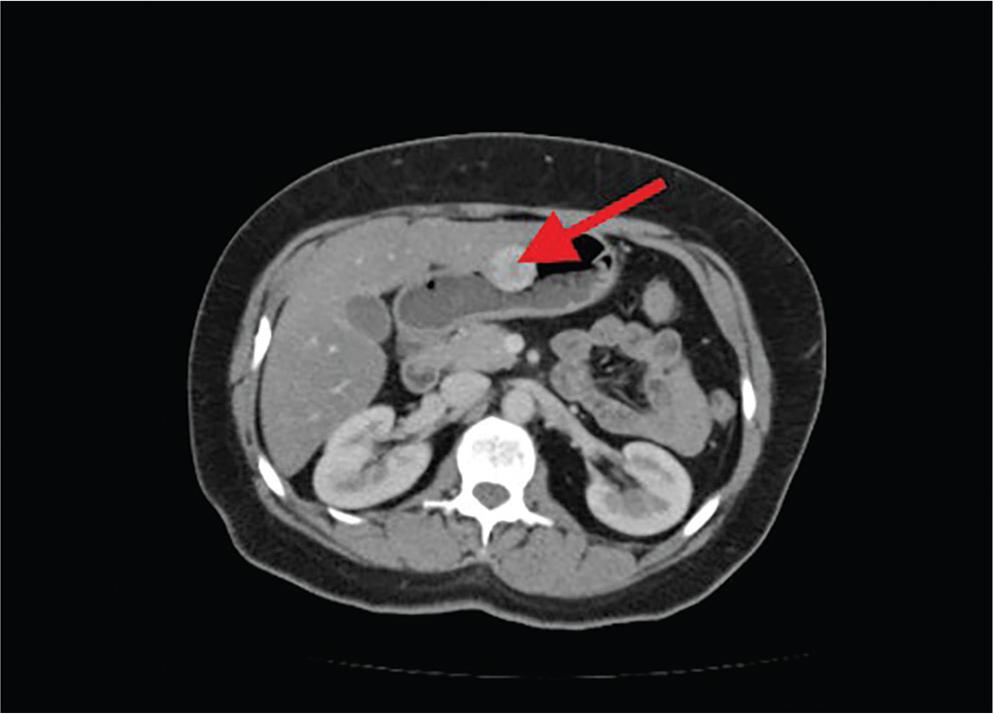
Contrast-enhanced CT abdomen (arterial phase) showing a round, circumscribed, avidly enhancing mass along the greater curvature of the stomach at the junction of the gastric body and antrum, suspicious for a hypervascular submucosal neoplasm.
Given the peri-pancreatic location of the mass and preoperative diagnostic uncertainty, and with a tumor size over 2 cm—a malignancy risk factor by Folpe criteria—a laparoscopic distal gastrectomy was performed. Wedge resection was suboptimal because of the tumor’s proximity to the pylorus. This posed a risk of inadequate margins or gastric outlet compromise. The frozen section was not obtained since the decision to resect the mass had been made preoperatively.
Histopathological examination of the resected specimen showed an epithelioid neoplasm with round cells and indistinct borders. The cells were arranged around branching capillary-sized vessels lined by endothelial cells, most compatible with a glomangioma [Figure 2]. Tumor cells stained positive for smooth muscle actin [Figure 3] and vimentin. They were negative for CD117, DOG1, S100 [Figure 4], desmin, and CD34. The Ki-67 proliferative index was about 1% [Figure 5].
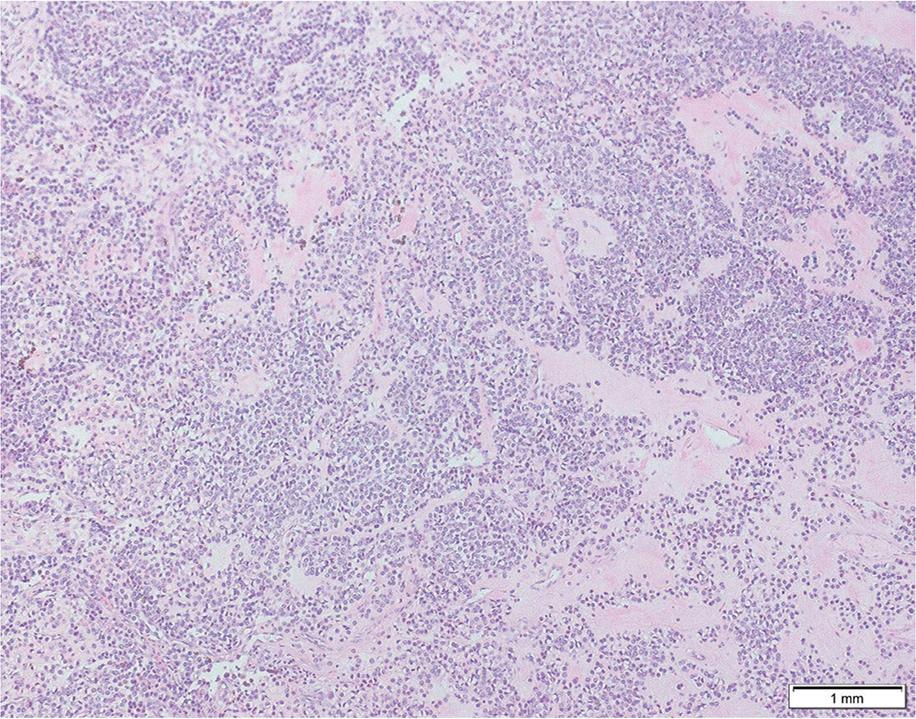
Hematoxylin and eosin (H&E) stained section (10×) demonstrating neoplastic epithelioid cells with round nuclei and indistinct borders arranged around branching capillary-sized vessels lined by endothelial cells, consistent with glomangioma.
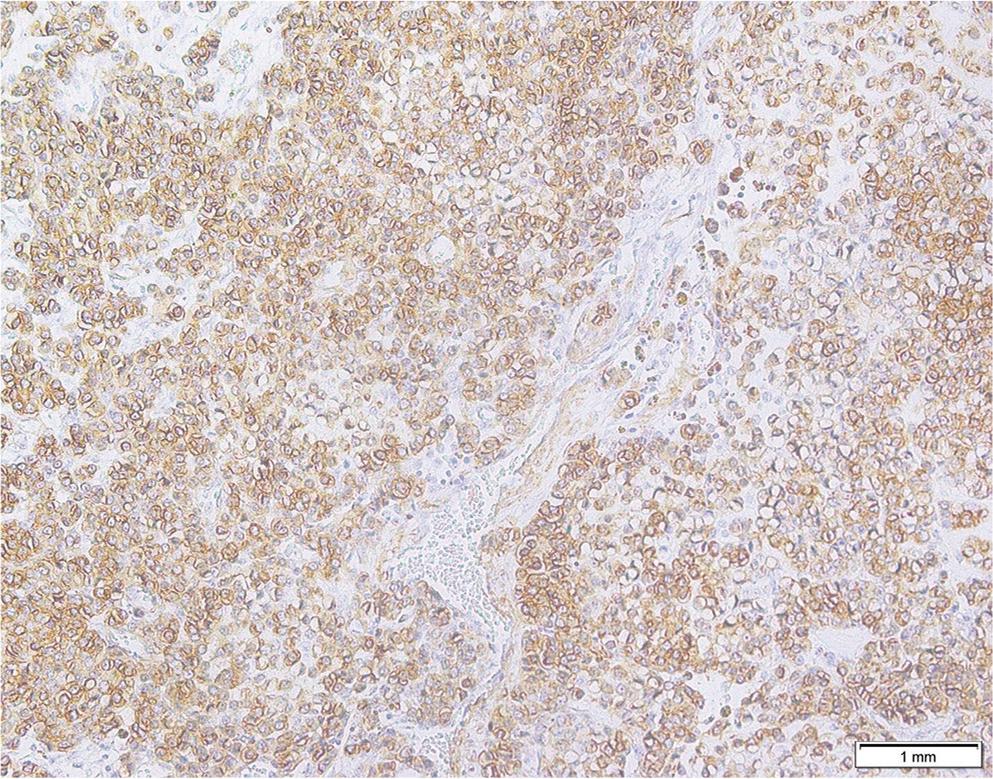
Immunohistochemical staining showing diffuse cytoplasmic positivity for smooth muscle actin (SMA) in tumor cells.
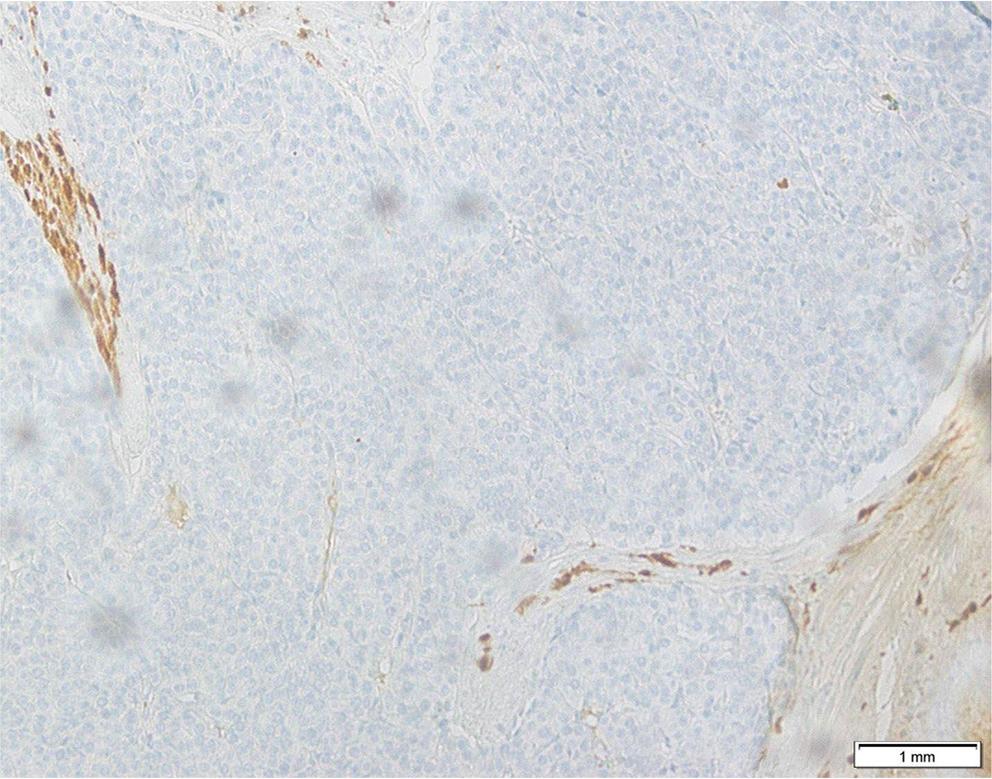
S100 immunostaining negative in tumor cells, excluding neural differentiation (schwannoma).
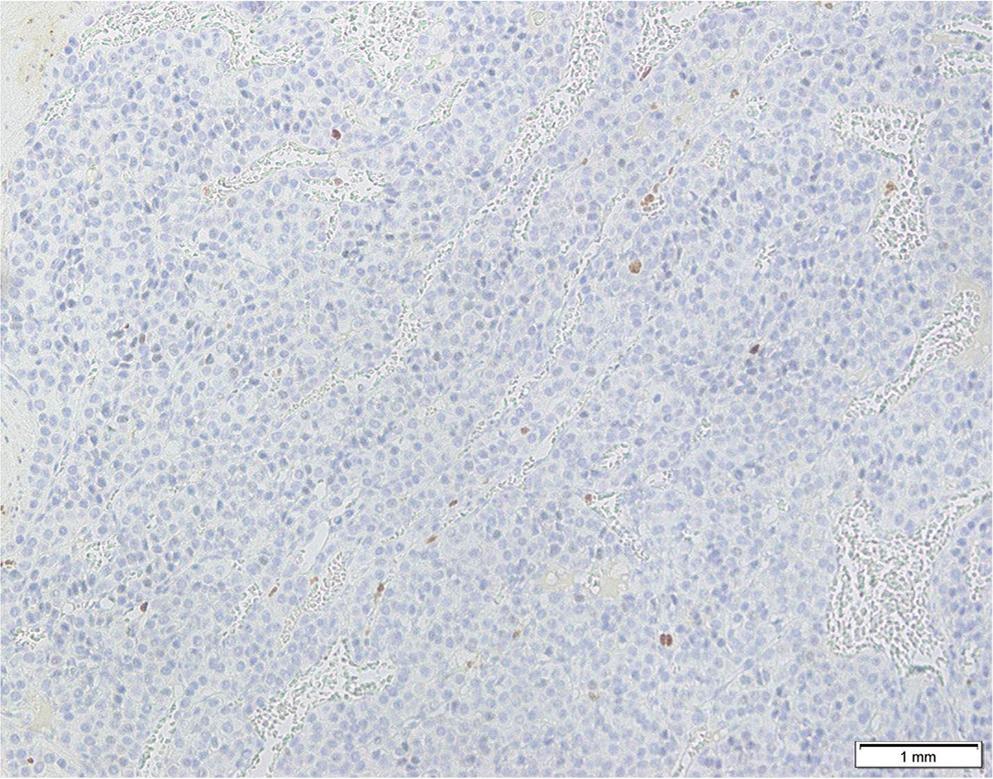
Ki-67 immunostain demonstrating very low proliferative activity (~1%), consistent with benign behavior.
No mitotic figures were seen in 50 HPF. There was no cytologic atypia, tumor necrosis, capsular or lymphovascular invasion. All margins were tumor-free. Fourteen incidental, reactive perigastric lymph nodes were identified in the specimen, all free of malignancy.
The postoperative course was uneventful. The patient’s epigastric burning and anorexia resolved completely after surgery. The residual weight loss was linked to the pre-existing major depressive disorder. The patient regained bout 4 kgt over six months after surgery and has maintained a stable weight since. No adjuvant therapy was indicated.
Follow-up CTs at 6 and 12 months showed no recurrence or metastasis. At 18 months, the patient is well and asymptomatic.
Glomus tumors of the gastrointestinal tract are rare benign mesenchymal neoplasms first described by Kay et al. in 1951. (5) These tumors are difficult to differentiate preoperatively from other submucosal tumors, primarily GISTs, carcinoid tumors, schwannomas, and hemangiomas, due to their submucosal location. (4,6) The gastric antrum is the most common intra-abdominal site, and GGTs show a female predominance with a peak incidence observed in the fifth and sixth decades of life. (1,7)
These tumors are often asymptomatic and may be detected incidentally during routine endoscopy. When symptomatic, patients may present with epigastric pain, dyspepsia, upper gastrointestinal bleeding, or constitutional symptoms. (8,9)
On contrast-enhanced CT, GGTs may exhibit a characteristic pattern of avid arterial-phase enhancement with persistent venous-phase enhancement, reflecting their highly vascular histology. This pattern was observed in our case and, while not pathognomonic, may serve as a supportive preoperative radiological clue. CT and MRI have limited specificity, as their features frequently mix with those of GISTs and other neuroendocrine neoplasms. (10,11)
EUS-guided FNB may improve preoperative diagnostic accuracy for submucosal gastric lesions. (12) However, obtaining an adequate amount of tissue from a lesion that is deeply located in the muscularis propria is difficult. (12,13) Larger-caliber core biopsy needles, such as Franseen or fork-tip designs, may provide better tissue architecture and improve diagnostic yield.
Furthermore, inclusion of GGT-specific markers, particularly SMA, vimentin, and synaptophysin, in the initial IHC panel would be advisable when an indeterminate epithelioid neoplasm is encountered at this anatomical site. In our case, if SMA positivity had been checked preoperatively, a more conservative surgical option, such as wedge resection, could have been considered.
The differential diagnosis of a hypoechoic muscularis propria lesion in the gastric antrum is broad. Table 1 summarizes the key immunohistochemical markers distinguishing GGT from the major clinical mimics.
Comparative immunohistochemical profile of gastric submucosal neoplasms
| Marker | GGT | GIST | Gastric NET | Schwannoma | Leiomyoma | Hemangioma |
|---|---|---|---|---|---|---|
| CD117 (KIT) | Negative | Positive | Negative | Negative | Negative | Negative |
| DOG1 | Negative | Positive | Negative | Negative | Negative | Negative |
| SMA | Positive | Variable | Negative | Negative | Positive | Variable |
| Vimentin | Positive | Variable | Variable | Positive | Positive | Variable |
| S100 | Negative | Negative | Negative | Positive | Negative | Negative |
| Desmin | Negative | Negative | Negative | Negative | Positive | Negative |
| CD34 | Negative* | Variable | Negative | Negative | Negative | Positive |
| CD31 | Negative | Negative | Negative | Negative | Negative | Positive |
| Chromogranin | Negative | Negative | Positive | Negative | Negative | Negative |
| Synaptophysin | Variable** | Negative | Positive | Negative | Negative | Negative |
| Ki-67 | Very low (<2%) | Variable | Stratifies grade | Low | Low | Low |
CD34 expression in glomus tumors is variable; focal positivity has been reported in a subset of cases and does not exclude the diagnosis.
Synaptophysin expression in GGT is occasionally focal and should not be used as a primary diagnostic marker. GGT = gastric glomus tumor; GIST = gastrointestinal stromal tumor; NET = neuroendocrine tumor.
GIST is the most important and common differential. It is reliably distinguished by co-expression of CD117 and DOG1, both of which were negative here. Gastric NETs should be considered in any epithelioid gastric wall lesion. Chromogranin and synaptophysin positivity, with Ki-67 stratifying tumor grade, are the hallmarks.
We did not apply these markers preoperatively, which represents a recognized limitation. Schwannoma (S100+) and leiomyoma (desmin+, SMA+) are readily excluded by their respective IHC profiles.
In the majority of cases, wedge resection with negative margins is the first-line surgical approach for GGTs and is generally curative. However, distal gastrectomy with reconstruction may be required for tumors located near the pylorus to avoid gastric outlet obstruction. (14)
The malignant potential of GGTs is very low, with fewer than 1% of cases reported to behave aggressively. According to the Folpe classification, features associated with malignant risk include: tumor size >2 cm, deep location, mitotic activity ≥5 figures per 50 HPF, and moderate-to-high nuclear grade. (2)
Tumors satisfying any one of these criteria are classified as having “uncertain malignant potential,” while frank malignancy typically requires size >2 cm combined with deep location, or mitotic activity ≥5/50 HPF, or moderate-to-high nuclear atypia.
In the present case, the tumor measured 2.4 cm, slightly above the 2 cm threshold, placing it in the uncertain malignant potential category on size alone. However, no other high-risk features were present, including mitoses, cytologic atypia, or necrosis, and the Ki-67 index was low. These findings indicate a very low risk of malignant behavior and highlight that tumor size alone should not be used to classify a glomus tumor as high risk. No standardized surveillance guidelines exist for gastric glomus tumors after complete resection. Because recurrence is uncommon with negative margins, follow-up practices vary in the literature. In our case, given the tumor size exceeding 2 cm, we took a cautious approach with contrast-enhanced CT of the abdomen at 6, 12, and 24 months, followed by an annual clinical assessment for up to 5 years. At 18 months of follow-up, there has been no evidence of recurrence or metastasis. Clinical follow-up alone may be sufficient in tumors that fully meet low-risk criteria.
Gastric glomangioma should be part of the differential diagnosis for any submucosal gastric tumor. Accurate preoperative diagnosis can be made using EUS with core biopsy and an IHC panel that includes GGT-specific markers. The surgical approach should be individualized for each patient: wedge resection should be the preferred approach, while distal gastrectomy may be required for peri-pancreatic tumors or cases with diagnostic uncertainty. The prognosis following complete resection is excellent.