
Hodgkin lymphoma (HL) is characterized by diagnostic large Reed-Sternberg (RS) cells, which originate from germinal center B lymphocytes. It is categorized into classical Hodgkin lymphoma (cHL) and nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL). cHL is subclassified as nodular sclerosis, mixed cellularity, lymphocyte-rich, and lymphocyte-depleted subtypes (1).
The ABVD protocol, which includes doxorubicin, bleomycin, vinblastine, and dacarbazine, originated in the 1970s, but further discoveries led to the incorporation of novel agents in the treatment regimen (2). In mid-2011, brentuximab vedotin (BV) received approval from the United States Food and Drug Administration, which replaced bleomycin in ABVD to form BV-AVD (brentuximab vedotin, doxorubicin, vinblastine, and dacarbazine) (3). The 12th International Conference on Malignant Lymphoma, held in June 2013 at Lugano, Switzerland, led to the incorporation of positron emission tomography (PET) fused with computed tomography (CT) as standard staging for lymphomas (4). These advancements in the field are difficult to implement in low- and middle-income countries (LMIC), keeping in view the human development index of Pakistan (5). The recent Global Cancer Observatory (GLOBOCAN) 2022 research indicates a rising incidence of cHL (6). In view of this, ABVD chemotherapy remains an affordable choice with better outcomes (7, 8). Our study contributes to the limited national data on the outcome of ABVD and factors associated with it.
In this cohort, we have seen ABVD response using overall survival (OS) and progression-free survival (PFS), while also identifying different factors affecting the outcome.
In this single-center retrospective cohort study, 246 consecutive adult patients, 18 years or above at the time of diagnosis of cHL, who received treatment at Aga Khan University Hospital, Karachi, Pakistan, from January 2013 through December 2023, were included after their informed consent. All the patients were diagnosed with cHL on either excisional or Tru-cut tissue biopsy, according to either the 2008 or 2016 revised WHO classification of Hematopoietic and Lymphoid Tumors (9, 10). Exclusion criteria were age below 18 years, diagnosis of nodular lymphocyte predominant HL, receiving all or part of treatment outside our institution, and use of chemotherapy other than ABVD. This was granted by the Ethical Review Committee of AKUH (AKU-ERC #: 2024-10031-29840).
The electronic medical record system was used to collect patient demographics, histopathological findings, immunohistochemistry status of CD15 and CD30, Eastern Cooperative Oncology Group (ECOG), comorbid conditions, B-symptoms, albumin, erythrocyte sedimentation rate, hemoglobin concentration, white blood cell count, and its differentials.
Disease characteristics like bulky disease, defined as a nodal mass exceeding one-third of the maximum transverse diameter of the chest or measuring greater than 10 cm in any direction, extranodal or bone marrow involvement, and stage. For staging and response assessment, contrast-enhanced Computed Tomography (CT) of the neck, chest, abdomen, and pelvis was used until 2015, after which Positron Emission Tomography/ Computed Tomography (PET/CT) became the institutional standard following its availability. ABVD chemotherapy response was evaluated by means of either CT-CAP or PET/CT, upon availability, after 2 cycles and then with an end-of-treatment scan one month after chemotherapy completion. According to the revised response criteria for malignant lymphomas (Lugano 2014 classification), disease evaluation by PET/CT was according to the Deauville 5-point scale, in which a complete response (CR) was called when the Deauville score was 1–3, a partial response (PR) if the Deauville score was 4, and stable disease (SD) or progressive disease (PD) if the Deauville score was 5 (4). Early-stage cHL was stage I/II disease and subdivided into favorable/unfavorable categories according to the National Comprehensive Cancer Network (NCCN) guideline on Hodgkin lymphoma (11). The modified Ann Arbor system was used for staging, while further risk stratification of advanced stages was according to the International Prognostic Score (IPS). The IPS score contained seven variables: scores when age is above or equal to 45 years, male, stage IV disease, white blood count above or equal to 15,000 cells/mL, the absolute lymphocyte count below 600 cells/mL or lymphocytes less than 8% of total white cell count, albumin below 40 g/L, and hemoglobin less than 105 g/L. Patients with up to 1 risk factor were considered low-risk, while those with 2 or 3 risk factors were considered intermediate-risk, and those with 4 or more risk factors were labelled high-risk (12, 13). We followed previously reported thresholds; a low lymphocyte-to-monocyte ratio (LMR) was defined as <2.1, a high neutrophil-to-lymphocyte ratio (NLR) as >6.0, and the absolute monocyte count (AMC) cutoff value as 750 cells/mm3 (14, 15).
The data used in the analysis was anonymized, and those with insufficient data were excluded. OS and PFS were primary endpoints of this study. We censored patients at the last follow-up date, irrespective of outcomes. All the patients received standard doses of doxorubicin (25 mg/m2), bleomycin (10 units/ m2, not exceeding 15 units), vinblastine (6 mg/m2, not more than 10 mg), and dacarbazine (375 mg/m2) on days 1 and 15 of each cycle, and each cycle span was 28 days, as per the NCCN guideline on Hodgkin lymphoma (11). Primary prophylaxis with granulocyte colony-stimulating factor (G-CSF) was not routinely recommended with ABVD chemotherapy, hence was considered as secondary prophylaxis. Before the implementation of PET/CT, favorable early-stage disease was treated with either two cycles of ABVD followed by 20 Gy involved-field radiotherapy (IFRT) or an additional 3–4 cycles of ABVD upon achieving complete remission (CR). For unfavorable early-stage disease, treatment comprised either four cycles of ABVD followed by 30 Gy IFRT or six ABVD cycles. Advanced-stage disease was treated with either 6 or 8 cycles of ABVD, with incorporation of radiotherapy only if bulky disease was present on initial presentation or residual disease was ≥ 2.5 cm. The relapsed/refractory cases received salvage chemotherapy followed by high-dose therapy and autologous stem cell transplant. Primary refractory status was defined as progressive disease within three months of ABVD (16).
After the RATHL study findings and institutional availability of PET/CT scans in 2016, PET response-based management was followed. Every patient received 2 ABVD cycles followed by an interim PET/CT scan. Favorable early-stage patients received either 20 Gy IFRT or 2 additional ABVD cycles if iPET Deauville 1–2, whereas 4 cycles of AVD were given to patients with a Deauville 3 response. Unfavorable early-stage patients received either 1 additional ABVD with 30 Gy IFRT or 2 ABVD cycles if Deauville 1–2 on iPET, while 2 ABVD cycles with IFRT or 4 AVD cycles were for patients with Deauville 3 on iPET. Either early-stage risk category with Deauville 4 or 5 on iPET received 2 ABVD. In advanced-stage iPET Deauville 1–3 patients, bleomycin was omitted after 2 cycles of ABVD, and they received 4 cycles of ABD. Patients with a Deauville score of 4 underwent escalation to BEACOPP, while those with Deauville 5 (stable/progressive disease) underwent tissue biopsy before any further treatment. Patients with primary refractory or relapsed disease received salvage chemotherapy following a multidisciplinary tumor board review. Regimens included ICE (ifosfamide, carboplatin, 52 etoposide), IGEV (ifosfamide, gemcitabine, vinorelbine, prednisolone), DHAP (dexamethasone, cytarabine, cisplatin), or brentuximab-bendamustine. The relapsed/refractory cHL patients who received salvage chemotherapy and achieved CR were evaluated for transplant fitness before receiving high-dose chemotherapy (Benda-EAM) prior to autologous hematopoietic stem cell transplant (AHSCT) to ensure remission (11, 17). The decision of radiotherapy was dependent upon the anatomy of the disease or the treating physician’s or patient’s discretion. We calculated PFS as the duration between the date of disease diagnosis and death irrespective of cause, PD, or last visit, while OS was the time interval between diagnosis and death or the last contact date. For the lost patients, we used their last contact date as the endpoint. Descriptive statistics were used for the analysis of patient characteristics in which the mean and standard deviation were used for continuous variables that were normally distributed. For skewed data we used interquartile ranges and medians. The patients who survived without progression were censored at their last confirmed alive date. Survival for the entire cohort was estimated using Kaplan-Meier methodology. Survival outcomes were compared across different variables by using the log-rank test. Prognostic factors associated with survival were described with respect to their 95% confidence intervals (CIs) using univariate Cox regression analysis. Independent prognostic factors were determined using multivariate Cox regression, including only those variables with a p-value < 0.2 on univariate analysis. We deemed the result significant if the p-value was below 0.05. Statistical calculations were performed on SPSS v.26 (IBM, USA) and R version 4.5.2 for Windows.
In this retrospective cohort, the median age was 35 years (18 to 77 years), with 62% male (male-to-female ratio 1.6:1), and 80.9% (199/246) had an ECOG PS of 0. More than one comorbidity was reported in 8.5% (21/246) of patients. Nodular sclerosis was identified in 86 patients (35.0%), followed by mixed cellularity (59 patients, 24.0%), lymphocyte-depleted (5 patients, 2.0%), and 96 patients (39.0%) were classified as unspecified classical Hodgkin lymphoma. Excisional biopsy was done in 54.5% (134/246), while 45.5% (112/246) underwent Tru-Cut biopsy. All biopsy samples were CD30-positive on immunohistochemistry. Clinical presentation included B-symptoms in 87.0% (214/246) of patients. Bulky disease (>33% of the transthoracic diameter or more than ten centimeters elsewhere) was observed in 8.9% (22/246) of cases. Bone marrow involvement was confirmed in 20.7% (51/246) of cases. Seventy-eight (31.7%) patients were early-stage, out of which 7.3% (18/78) were stratified as favorable, while the remaining 24.7% (60/78) had unfavorable early-stage disease. Advanced-stage disease (stage III–IV) was found in 68.3% (168/246) of patients. The advanced-stage disease was risk-stratified according to the International Prognostic Score (IPS) as 12.2% (30/168) low risk (score 0–1), 32.5% (80/168) intermediate risk (score 2–3), and 23.6% (58/168) high risk (score ≥ 4) patients. The median number of ABVD cycles administered was six, with a range of two to eight cycles. Thirty patients (12.2%) received involved-field radiotherapy (IFRT) at a dose of 2 Gy per fraction per day, which included four early favorable-stage patients (20–30 Gy in 10–15 fractions), 17 early unfavorable-stage patients (20–36 Gy in 10–18 fractions), and nine advanced-stage patients (20–44 Gy in 10–22 fractions). Median delay in treatment initiation from diagnosis was 25 (0–202) days. In this cohort, 14.6% (36/246) of patients had relapsed/refractory cHL, out of which 6.5% (16/246) received high-dose chemotherapy (HDC) followed by autologous hematopoietic stem cell transplant (AHSCT). Patients who underwent HDC/AHSCT received salvage therapy as Brentuximab-Bendamustine (n=6), DHAP (dexamethasone, cytarabine, and cisplatin; n=4), ICE (ifosfamide, carboplatin, and etoposide; n=4), or IGEV (ifosfamide, gemcitabine, vinorelbine, and prednisolone; n=2). The remaining patient characteristics are given in Table 1.
Patients demographics and treatment characteristics.
| Characteristics | Number (n) | Percentage (%) |
|---|---|---|
| Total number of patients | 246 | |
| Median Age (years) | 35 (18–77) | |
| Male | 153 | 62.2% |
| Female | 93 | 37.8% |
| ESR (≥50 mm/h) | 92 | 37.4% |
| Age at diagnosis (Years) | ||
| ≤45 | 145 | 58.9% |
| 46–64 | 81 | 32.9% |
| >64 | 20 | 8.1% |
| Ann Arbor stage | ||
| I | 23 | 9.3 % |
| II | 57 | 23.2% |
| III | 68 | 27.6% |
| IV | 100 | 40.7% |
| Bulky Disease | 22 | 8.9% |
| Extranodal Disease | 46 | 18.7% |
| Bone Marrow Involvement | 51 | 20.7% |
| Combined Modality (Chemo-radiotherapy) | ||
| Early favourable | 4 | 1.6% |
| Early unfavourable | 17 | 6.9% |
| Advanced stage (III/IV) | 9 | 3.7% |
| Interim PET/CT Response | ||
| Deauville 1–3 | 174 | 70.7% |
| Deauville 4 | 63 | 25.6% |
| Deauville 5 | 9 | 3.7% |
| End of Treatment PET/CT Response | ||
| Deauville 1–3 | 176 | 71.5% |
| Deauville 4 | 4 | 1.6% |
| Deauville 5 | 39 | 15.9% |
| Relapse/Refractory | ||
| Primary refractory | 16 | 6.5% |
| Relapse after 3 months | 20 | 8.1% |
| Salvage therapy | ||
| Brentuximab-Bendamustine | 16 | 6.5% |
| DHAP | 9 | 3.7% |
| ICE | 6 | 2.4% |
| IGEV | 5 | 2.0% |
Abbreviation key: DHAP (dexamethasone, cytarabine, and cisplatin); ICE (Ifosfamide, Carboplatin, and Etoposide); IGEV (ifosfamide, gemcitabine, vinorelbine, and prednisolone); ESR Erythrocyte Sedimentation Rate; PET positron emission tomography; CT computerized tomography.
The reverse Kaplan-Meier demonstrated a median follow-up of 35.0 months (95% CI: 29–41). The median OS and PFS were not reached. At the time of the last encounter, 83.3% (205/246) of patients remained alive, while 16.7% (41/246) had deceased. Two-year OS and PFS in our cohort were 85.6% (95% CI: 80.8% - 90.7%) and 74.7% (95% CI: 68.8% - 81.1%), respectively. Five-year OS and PFS in our cohort were 79.5% (95% CI: 73.4% - 86.2%) and 66.0% (95% CI: 58.7% - 74.2%), respectively (Figure 1).
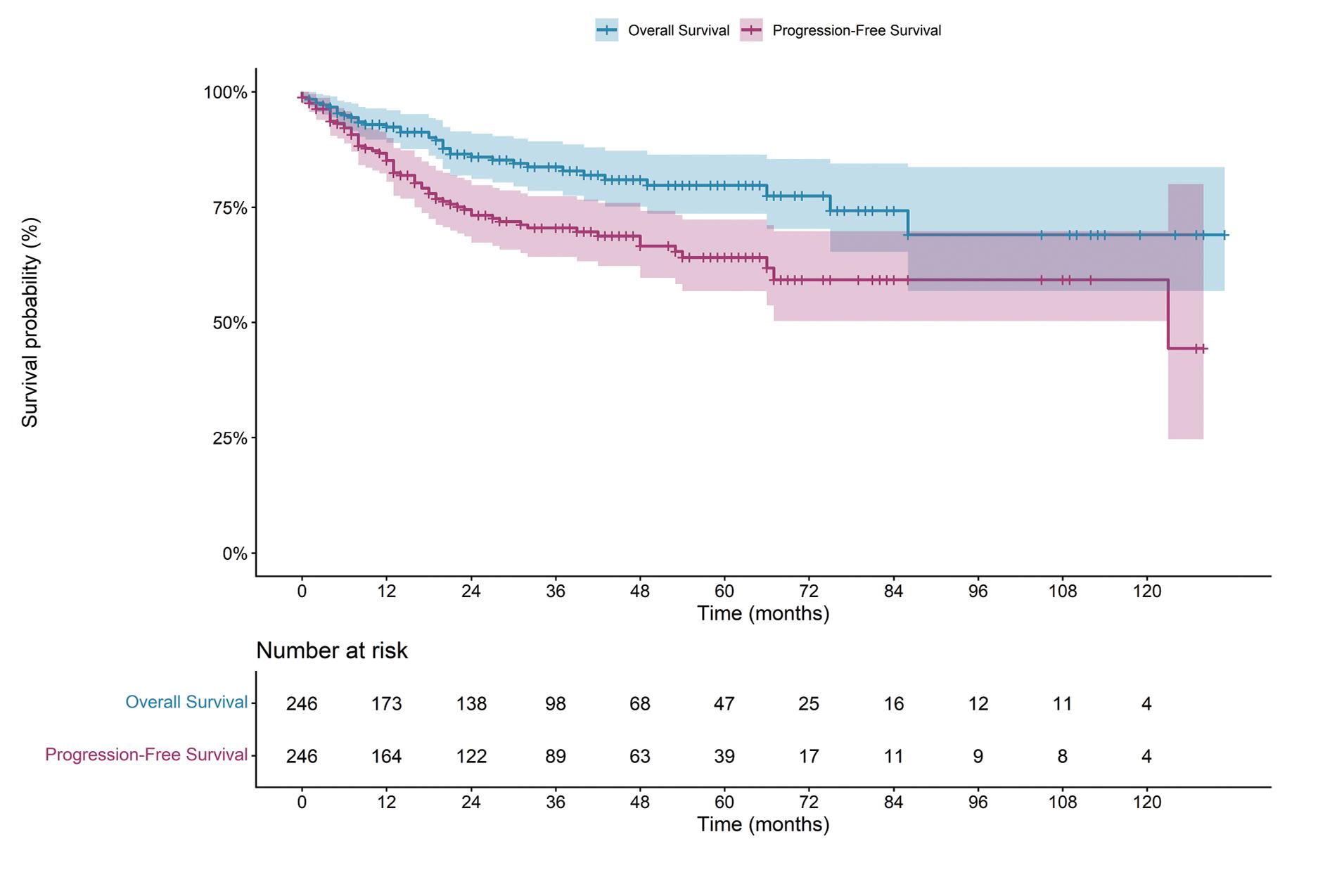
Kaplan–Meier estimates of two-year and five-year overall survival and progression-free survival.
Survival differences using the Kaplan–Meier log-rank test demonstrated that several factors affected both OS and PFS, including age, stage, bone marrow involvement, IPS, hemoglobin, albumin level, ECOG performance status, histologic subtype, and neutrophil-to-lymphocyte ratio. Additionally, hemoglobin level, leukocytosis, and absolute lymphocyte count were identified as significant predictors for PFS (Table 2).
Log-rank analysis for overall-survival (OS) and progression-free survival (PFS) predictors
| Variable | OS Log-rank | p-value | PFS Log-rank | p-value |
|---|---|---|---|---|
| Age | 22.00 | <0.001*** | 6.04 | 0.049* |
| B symptoms | 1.89 | 0.169 | 2.06 | 0.152 |
| Bulky disease | 3.35 | 0.067 | 1.11 | 0.292 |
| Extra-nodal disease | 0.91 | 0.340 | 2.92 | 0.088 |
| Bone marrow involvement | 4.41 | 0.036* | 5.28 | 0.022* |
| IPS | 25.19 | <0.001*** | 25.12 | <0.001*** |
| Stage (Advance vs early) | 12.00 | 0.003** | 10.47 | 0.005** |
| Comorbidity (>1 vs ≤1) | 0.01 | 0.937 | 0.23 | 0.635 |
| WBC (≥15 vs <15 × 109/L) | 3.67 | 0.056 | 8.99 | 0.003** |
| ALC (<0.6 vs ≥0.6 × 109/L) | 3.63 | 0.057 | 0.42 | 0.515 |
| Hemoglobin (<105 vs ≥105 g/L) | 17.53 | <0.001*** | 7.01 | 0.008** |
| Albumin (<40 vs ≥40 g/L) | 25.26 | <0.001*** | 19.49 | <0.001*** |
| ECOG (≥2 vs <2) | 32.57 | <0.001*** | 24.81 | <0.001*** |
| Histology | 1.86 | 0.603 | 5.78 | 0.123 |
| LMR (≤ 2.1 vs > 2.1) | 3.11 | 0.078 | 1.78 | 0.182 |
| AMC (> 750 vs ≤ 750 cells/mm3) | 1.11 | 0.293 | 0.52 | 0.471 |
| NLR (> 6 vs ≤ 6) | 5.51 | 0.019* | 12.50 | <0.001*** |
Abbreviation key: CI Confidence interval; HR Hazard ratio; AMC: Absolute monocyte count; LMR: Lymphocyte-to-monocyte ratio; NLR, Neutrophil-to-lymphocyte ratio; WBC, White blood cell; ECOG: Eastern Cooperative Oncology Group; IPS: International Prognostic Score.
p<0.05;
p<0.01;
p<0.001.
On univariate analysis, factors that were significantly associated with inferior overall survival were increasing age (hazard ratio 2.26, 95% CI 1.48–3.45; p<0.001), bone marrow involvement (HR 2.29, 95% CI 1.21–4.32; p=0.011), advanced-stage disease (HR 7.23, 95% CI 1.84–28.39; p=0.005), ECOG ≥2 (HR 7.64, 95% CI 3.29–17.75; p<0.001), hemoglobin <105 g/L (HR 2.65, 95% CI 1.43–4.91; p=0.002), and albumin <40 g/L (HR 2.69, 95% CI 1.60–4.53; p<0.001). Factors associated with inferior progression-free survival were poor ECOG status (HR 5.23, 95% CI 2.47–11.11; p<0.001), leukocytosis (HR 2.70, 95% CI 1.56–4.66; p<0.001), an elevated neutrophil-to-lymphocyte ratio (HR 2.48, 95% CI 1.51–4.06; p<0.001), hypoalbuminemia (HR 2.28, 95% CI 1.54–3.38; p<0.001), anemia (HR 2.22, 95% 53 CI 1.36–3.63; p=0.001), bone marrow involvement (HR 1.85, 95% CI 1.09–3.13; p=0.023), extranodal disease (HR 1.81, 95% CI 1.06–3.10; p=0.031), and histological subtype (HR 1.19, 95% CI 1.03–1.38; p=0.021), along with advanced-stage disease (HR 4.05, 95% CI 1.85–8.85; p=0.001) (Table 3).
Results of univariate analysis for overall survival and progression-free survival predictors
| Variable | OS HR (95% CI) | p-value | PFS HR (95% CI) | p-value |
|---|---|---|---|---|
| Age | 2.26 (1.48 - 3.45) | <0.001*** | 1.42 (0.99 - 2.03) | 0.054 |
| B symptoms | 1.30 (0.46 - 3.66) | 0.616 | 1.67 (0.67 – 4.18) | 0.269 |
| Bulky disease | 1.87 (0.82 - 4.26) | 0.139 | 1.41 (0.67 - 2.96) | 0.367 |
| Extra-nodal disease | 1.38 (0.68 - 2.83) | 0.373 | 1.81 (1.06 - 3.10) | 0.031* |
| Bone marrow involvement | 2.29 (1.21 - 4.32) | 0.011** | 1.85 (1.09 - 3.13) | 0.023* |
| IPS | 1.18 (0.88 - 1.58) | 0.276 | 1.21 (0.96 - 1.53) | 0.109 |
| Stage (Advance vs early) | 7.23 (1.84 - 28.39) | 0.005** | 4.05 (1.85 - 8.85) | 0.001** |
| Comorbidity (>1 vs ≤1) | 1.01 (0.36 - 2.86) | 0.978 | 1.33 (0.53 - 3.32) | 0.543 |
| WBC (≥15 vs <15 × 109/L) | 1.85 (0.91 - 3.77) | 0.091 | 2.70 (1.56 - 4.66) | <0.001*** |
| ALC (<0.6 vs ≥0.6 × 109/L) | 2.03 (0.85 – 4.84) | 0.113 | 1.21 (0.52 - 2.80) | 0.663 |
| Hemoglobin (<105 vs ≥105 g/L) | 2.65 (1.43 - 4.91) | 0.002** | 2.22 (1.36 - 3.63) | 0.001** |
| Albumin (<40 vs ≥40 g/L) | 2.69 (1.60 - 4.53) | <0.001*** | 2.28 (1.54 - 3.38) | <0.001*** |
| ECOG (≥2 vs <2) | 7.64 (3.29 - 17.75) | <0.001*** | 5.23 (2.47 - 11.11) | <0.001*** |
| Histology | 1.15 (0.96 - 1.38) | 0.126 | 1.19 (1.03 - 1.38) | 0.021* |
| LMR (≤ 2.1 vs > 2.1) | 1.44 (0.77 - 2.70) | 0.254 | 1.48 (0.89 - 2.45) | 0.128 |
| AMC (> 750 vs ≤ 750 cells/mm3) | 1.26 (0.68 - 2.33) | 0.459 | 1.10 (0.67 - 1.80) | 0.697 |
| NLR (> 6 vs ≤ 6) | 1.80 (0.97 - 3.37) | 0.064 | 2.48 (1.51 - 4.06) | <0.001*** |
Abbreviation key: CI Confidence interval; HR Hazard ratio; ALC: Absolute lymphocyte count; AMC: Absolute monocyte count; LMR: Lymphocyte-to-monocyte ratio; NLR, Neutrophil-to-lymphocyte ratio; WBC, White blood cell; ECOG: Eastern Cooperative Oncology Group; IPS: International Prognostic Score.
p<0.05;
p<0.01;
p<0.001.
Independent prognostic factors were identified using multivariate analysis, including only variables with p-values < 0.20 on univariate analysis. In the multivariate analysis, advanced-stage disease was the strongest independent predictor of overall survival (OS) (HR 6.80, 95% CI 1.07–43.28; p=0.043), followed by ECOG PS ≥2 (HR 3.81, 95% CI 1.22–11.97; p=0.022), bulky disease (HR 2.94, 95% CI 1.09–7.94; p=0.034), and increasing age (HR 2.00, 95% CI 1.15–3.47; p=0.014). Regarding progression-free survival (PFS), ECOG performance status remained the sole independent predictor (HR 3.99, 95% CI 1.47–10.86; p=0.007) (Table 4).
Multivariable Cox proportional hazards regression analysis for overall survival and progression-free survival predictors
| Variable | OS HR (95% CI) | p-value | PFS HR (95% CI) | p-value |
|---|---|---|---|---|
| Age | 2.00 (1.15 - 3.47) | 0.014* | 1.24 (0.77 - 1.97) | 0.374 |
| B symptoms | 1.49 (0.40 - 5.53) | 0.548 | 1.59 (0.58 – 4.38) | 0.367 |
| Bulky disease | 2.94 (1.09 – 7.94) | 0.034* | 1.68 (0.75 – 3.79) | 0.211 |
| Extra-nodal disease | 1.26 (0.55 - 2.89) | 0.586 | 1.04 (0.56 - 1.95) | 0.894 |
| Bone marrow involvement | 1.15 (0.55 – 2.40) | 0.715 | 1.01 (0.56 – 1.83) | 0.973 |
| IPS | 1.41 (0.73 – 2.74) | 0.305 | 1.23 (0.74 - 2.05) | 0.432 |
| Stage (Advance vs early) | 6.80 (1.07 - 43.28) | 0.043* | 3.24 (0.93 - 11.35) | 0.066 |
| WBC (≥15 vs <15 × 109/L) | 1.42 (0.54 - 3.74) | 0.475 | 1.77 (0.89 – 3.55) | 0.107 |
| ALC (<0.6 vs ≥0.6 × 109/L) | 1.67 (0.55 – 5.02) | 0.363 | 1.04 (0.39 - 2.77) | 0.946 |
| Hemoglobin (<105 vs ≥105 g/L) | 1.50 (0.66 – 3.39) | 0.331 | 1.38 (0.72 – 2.64) | 0.332 |
| Albumin (<40 vs ≥40 g/L) | 1.62 (0.81 – 3.25) | 0.175 | 1.44 (0.84 - 2.45) | 0.185 |
| ECOG (≥2 vs <2) | 3.81 (1.22 - 11.97) | 0.022* | 3.99 (1.47 - 10.86) | 0.007** |
| Histology | 1.22 (0.99 - 1.50) | 0.059 | 1.17 (1.00 - 1.38) | 0.051 |
| LMR (≤ 2.1 vs > 2.1) | 1.46 (0.65 - 3.27) | 0.361 | 1.44 (0.75 - 2.76) | 0.273 |
| NLR (> 6 vs ≤ 6) | 1.08 (0.49 - 2.44) | 0.828 | 1.72 (0.91 – 3.28) | 0.097 |
Abbreviation key: CI Confidence interval; HR Hazard ratio; ALC: Absolute lymphocyte count; LMR: Lymphocyte-to-monocyte ratio; NLR, Neutrophil-to-lymphocyte ratio; WBC, White blood cell; ECOG: Eastern Cooperative Oncology Group; IPS: International Prognostic Score.
p<0.05;
p<0.01;
p<0.001.
Overall, the ABVD chemotherapy was well tolerated. Short-term toxicities were addressed through a dedicated hotline or day-care unit, leading to an under-reporting of such events; hence, we could not retrieve that data. While in long-term toxicities, 3 patients experienced second malignancies, which included 1 anaplastic large cell lymphoma, 1 neuroendocrine tumor, and 1 adenocarcinoma of the lungs. All of these 3 had advanced-stage cHL and received 6 cycles of ABVD. Bleomycin was skipped in 3 patients due to reported restrictive lung disease on pulmonary function tests prior to the initiation of ABVD. Two (0.8%) patients developed bleomycin-induced restrictive lung disease, and 1 (0.4%) developed cardiotoxicity. Out of 41 deceased patients, 6 had sepsis, and 12 had progressive disease, while in 23 of the patients, the cause of death remained unspecified.
In this retrospective cohort of 246 patients, the median age of diagnosis with cHL was 35 years with male predominance (1.6:1), which is comparable to the pattern seen in resource-constrained settings (18–21). Nodular sclerosis (35%) and mixed cellularity (24%) were the dominant subtypes, consistent with the WHO classification (1, 22). In 87 out of 112 true-cut biopsies, subtyping could not be done, and they were reported as classic Hodgkin lymphoma. In our cohort, histological subtyping was not associated with overall survival, as in the Rose et al. study (21). Biasoli et al. (23), found ECOG PS of more than or equal to 2 as an independent predictor of poor OS, while across log-rank, univariate, and multivariate analyses we similarly found ECOG performance an independent predictor of both PFS and OS. The median time from tissue diagnosis to treatment initiation was 29 (0–202) days, which is similar to other developing countries (23, 24).
The median number of ABVD cycles was 6 (range, 2–8), and involved-field radiation (IFRT) was used in 21 of 78 early-stage patients; institutional availability of PET/CT enabled a response-guided treatment approach. The PET/CT-based approach avoided over- or under-treatment and has decreased treatment-related toxicities (4). At the end of therapy, 177 patients (72%) achieved complete remission, as defined by an end-of-treatment PET/CT scan Deauville score of 1–3. The observed relapse rate of 14.6% (36/246) was similar to those reported in cohorts from neighboring countries, such as India (25) and China (22). The survival outcomes of our study (2- and 5-year OS of 85.6% and 79.5%, respectively) were comparable to those of developing countries but modestly lower than what we see in high-resource settings (OS 90–95%), attributable to advanced-stage presentation and poor risk factors like unfavorable early stage and high IPS (21, 26).
Increasing age, bulky disease, and advanced-stage disease were independent predictors of OS. Hemoglobin and albumin were significant for OS on univariate analysis; similarly, NLR was significant for PFS. The advanced stage disease (stage III–IV) was seen in 68.3% (168/246) of patients, which is a common scenario in developing countries due to lack of awareness, unaffordability, poor health care facilities, empiric tuberculosis treatment, delay in diagnosis due to fine-needle aspiration, and seeking alternative medicine (25, 27). Disease staging showed a significant association with overall survival (OS)—hazard ratio (HR) 6.80 (1.07–43.28); p=0.043. On log-rank analysis, early favorable disease was found to have better OS and PFS than early unfavorable disease, and both had better outcomes than advanced-stage disease (p < 0.05). Similarly, the International Prognostic Score (IPS)-based risk stratification of advanced-stage disease into low, intermediate, and high risk showed statistical significance: the higher the risk, the lower the OS and PFS (p<0.05). These results were concomitant with other studies (12, 19, 21, 28). Cellini et al. (29) reported an association between high NLR and poor PFS, and between low LMR and poor OS and PFS, but in our study, we found only a high neutrophil-to-lymphocyte ratio associated with worse PFS on univariate analysis. Marcheselli et al. (15), and Tadmor et al. (14), reported AMC more than 750 cells/mm3 as an independent predictor of poor OS and PFS, but their data included patients with only nodular sclerosis who received different chemotherapies, unlike our study, in which the majority of the cases were unspecified cHL and found no association of AMC with either PFS or OS.
Yang Liang Boo et al. (27), reported 5.4% patients with febrile neutropenia, while 3.2% experienced pulmonary toxicity due to bleomycin. Jacob et al. (19), found 9.5% patients with febrile neutropenia and 3.5% developed pulmonary toxicity attributable to bleomycin. Although bleomycin was better tolerated in our patients, as only two patients (0.8%) developed bleomycin-induced restrictive lung disease, 1 (0.4%) developed cardiotoxicity, and 6 (2.43%) died of sepsis. Sixteen (6.5%) patients underwent high-dose chemotherapy followed by autologous HSCT.
Retrospective analysis inherently has selection bias, which is one of the limitations of our study. Another limitation was the inability to retrieve data on short-term toxicities, as these events were typically managed and recorded by a dedicated hotline or day-care team. Additional study limitations include the unavailability of PET/CT facilities until 2015, which likely influenced patient outcomes. Furthermore, the COVID-19 pandemic caused significant treatment delays; the median time from diagnosis to treatment initiation rose to 23 months (IQR 17.75–40.75) in 2019–2020, compared to 19.50 months (IQR 11.75–31.2) during 2013–2018. Three patients were lost to follow-up during this pandemic. The use of Tru-Cut biopsies posed a diagnostic challenge, as they often failed to identify the precise histopathological subtype of classical Hodgkin lymphoma (cHL).
In conclusion, our data provide evidence that age, stage, bulky disease, and ECOG are significant factors affecting OS, but log-rank analysis underscores the importance of disease risk stratification. Early disease recognition and prompt treatment with PET/CT response assessment can improve outcomes. Keeping in view the introduction of novel therapeutic agents, ABVD remains an effective and accessible treatment option in LMIC settings, where the availability of novel agents and hematopoietic stem cell transplants remains uncertain.