
Parathyroid glands play a pivotal role in calcium and phosphorus metabolism in the body. Parathyroid hormone regulates bone mineralization and resorption. Primary hyperparathyroidism is a disease caused by increased parathyroid hormone secretion. This hypersecretion leads to various consequences, such as increased calcium reabsorption from the kidneys, phosphaturia, excessive vitamin D synthesis, and bone resorption. Patients typically present with symptoms including depression, abdominal pain, renal stones, and declining functional status. However, in some cases, the condition is asymptomatic and is detected during routine workups. Parathyroid adenomas are considered the primary etiology in about 85% of primary hyperparathyroidism (PHPT) cases [1]. Brown tumors are reported in 1.5% to 4.5% of clinical cases with primary or secondary hyperparathyroidism [2]. A brown tumor is formed as a consequence of localized, rapid osteoclastic turnover of bone due to the direct effects of parathyroid hormone (PTH). These are the most pathognomonic signs of primary hyperparathyroidism [3]. They can develop in any bone of the body [4]. However, if a similar lesion is observed in patients without primary hyperparathyroidism, the differential diagnosis becomes challenging.
Parathyroid surgery is the only definitive treatment of symptomatic primary hyperparathyroidism. Parathyroidectomy is an effective treatment that cures the disease, improves bone mineral density (BMD), decreases fracture risk, and enhances quality of life.
Hypocalcemia is a common issue after parathyroidectomy. It is typically transient when bone disease is mild. However, postoperative hypocalcemia can be severe and prolonged, a phenomenon known as hungry bone syndrome. This syndrome is especially common among patients with bone disease associated with chronic increased bone resorption [5].
Careful monitoring is essential to prevent and treat symptomatic hypocalcemia, which can be catastrophic. It is advised to measure serum calcium levels two to four times a day during the first few postoperative days.
A 21-year-old girl, with no family history of any parathyroid disease, presented to the walk-in clinic of Shaukat Khanum Memorial Cancer Hospital and Research Center, with complaints of gastric problems. At the age of 16 years, she started complaining of stomach pain and vomiting. For a few years, she kept taking homeopathic medications. Her functional status declined to a point that she was wheelchair bound and used to mobilize with a Z-frame. She got her MRI done from a local facility, which showed large lytic lesions on the iliac blades, acetabulum, and sacrum. They were considered as a primary bone malignancy versus metastatic bone deposits. On further workup, she was advised to undergo biopsy of these lesions, which showed a simple bone cyst.
Evaluation through blood tests suggested raised calcium and parathyroid hormone levels, consistent with primary hyperparathyroidism (Table 1).
Summary of the blood analysis of the patient.
| Laboratory tests | Results | Reference range |
|---|---|---|
| Hemoglobin | 11.7 g/dl | 12–15 g/dl |
| Creatinine | 0.38 mg/dl | 0.50–0.90 mg/dl |
| eGFR | 212.49 mL/min/1.73 m2 | >60 mL/min/1.73 m2 |
| Calcium, corrected | 12.17 mg/dl | 8.5–10.5 mg/dl |
| 25 Hydroxy Vitamin D | 22.21 ng/ml | Insufficiency 20 - less than 30 ng/mL |
| PTH-Intact | 231.8 pg./mL | 18.5–88 pg./mL |
| Free T4 | 0.87 ng/dl | 0.89–1.76 ng/dl |
| TSH | 1.62 uIU/ml | 0.35–5.5 uIU/ml |
| GLUCOSE (FASTING) | 92 mg/dL | 70 – 99 mg/dl |
| Prolactin | 18 ng/ml | 1.90 – 25 ng/ml |
| Metanephrine, Normetanephrine | 54.71 pg/mL | Less than 90 pg/ml |
| 165.5 pg/mL | Less than 190 pg/ml | |
| CALCITONIN | 3.39 pg/mL | ND – 5.0 pg/ml |
| CEA | 0.643 ng/mL | 0.8–2.5 pg/ml |
Computed tomographic scanning of the chest, abdomen, and pelvis showed a “Hypodense mixed solid/cystic nodule in the right lobe of the thyroid gland. The left lobe is normal. A small, round nodule just below the left thyroid lobe could be a parathyroid nodule. The pancreas shows clumps of calcification noted within the pancreatic parenchyma. Tiny calcific foci are noted in the right kidney and left kidney lower pole without hydronephrosis. Multiple lytic expansile lesions are noted involving the ribs, left humerus, and pelvic bones” (Figure 1).
Magnetic resonance imaging of both lower limbs showed “Multiple expansile lesions with fluid levels seen in the right femur and tibia. Multiple expansile lesions with fluid levels seen in the left femur, tibia, and fibula” (Figure 2).
As biochemical evidence of primary hyperparathyroidism was established with the presence of pancreatic and renal calcifications along with cystic bone lesions, it was planned in a multidisciplinary team meeting to proceed with parathyroidectomy.
To proceed with parathyroidectomy, further imaging was advised to locate the parathyroid adenoma, which included Magnetic resonance imaging neck and a Parathyroid scan with methoxy-isobutyl-isonitrile (Mibi) was conducted.
Parathyroid scan showed “A 0.8 cm soft tissue density appreciable at the inferoposterior aspect of left thyroid lobe without any sestamibi uptake, likely concerning for enlarged left parathyroid gland, multiple well-defined expansile lytic lesions with thinned out cortex in the visualized skeleton are typical for brown tumors.”
Magnetic resonance imaging showed “Prominent T2 hyperintense well-circumscribed nodular mass is noted adjacent/within the right thyroid lobe at its interpolar/upper pole region, measuring up to 13 × 11 mm. Another similar signal intensity nodule is noted along the inferior edge of the left thyroid lobe, which measures up to 8 × 7 mm. These could represent parathyroid masses” (Figure 3).
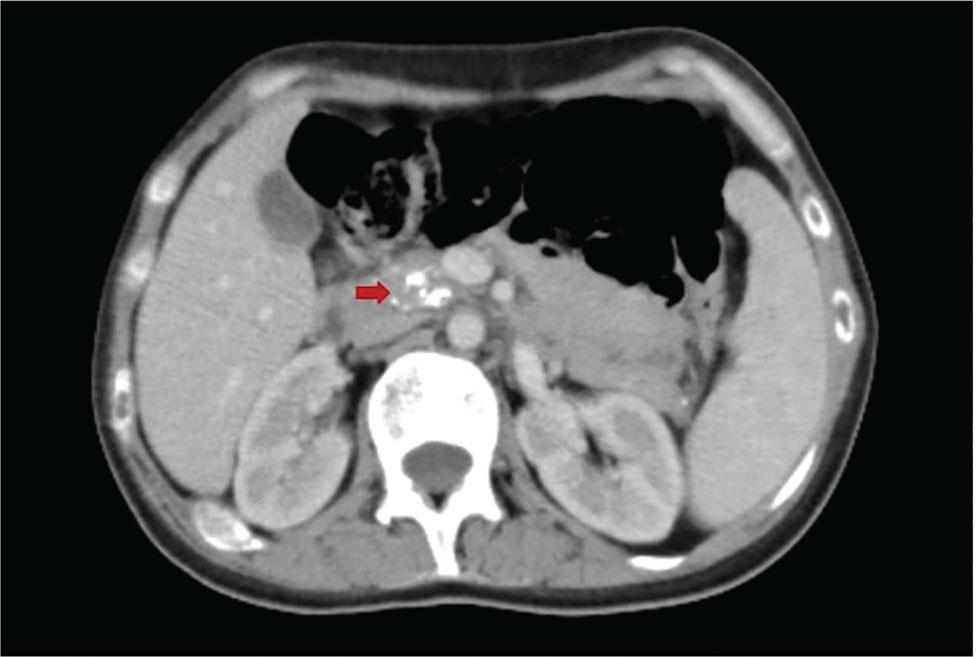
Computed tomography scanning chest, abdomen, and pelvis showing pancreatic calcification (red arrow).
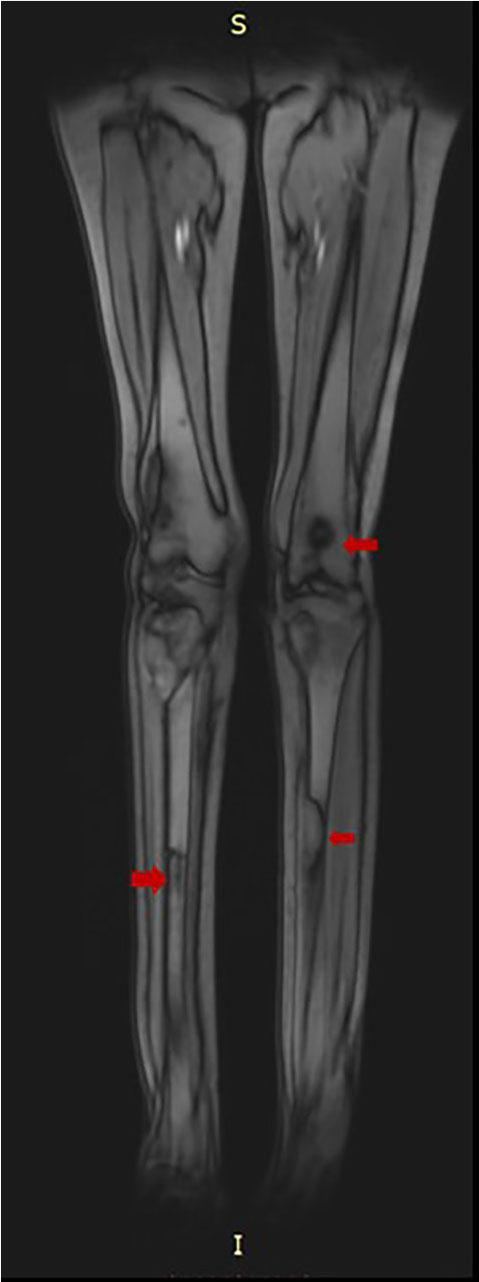
Magnetic resonance imaging lower limbs showing bilateral lytic lesions (red arrows).
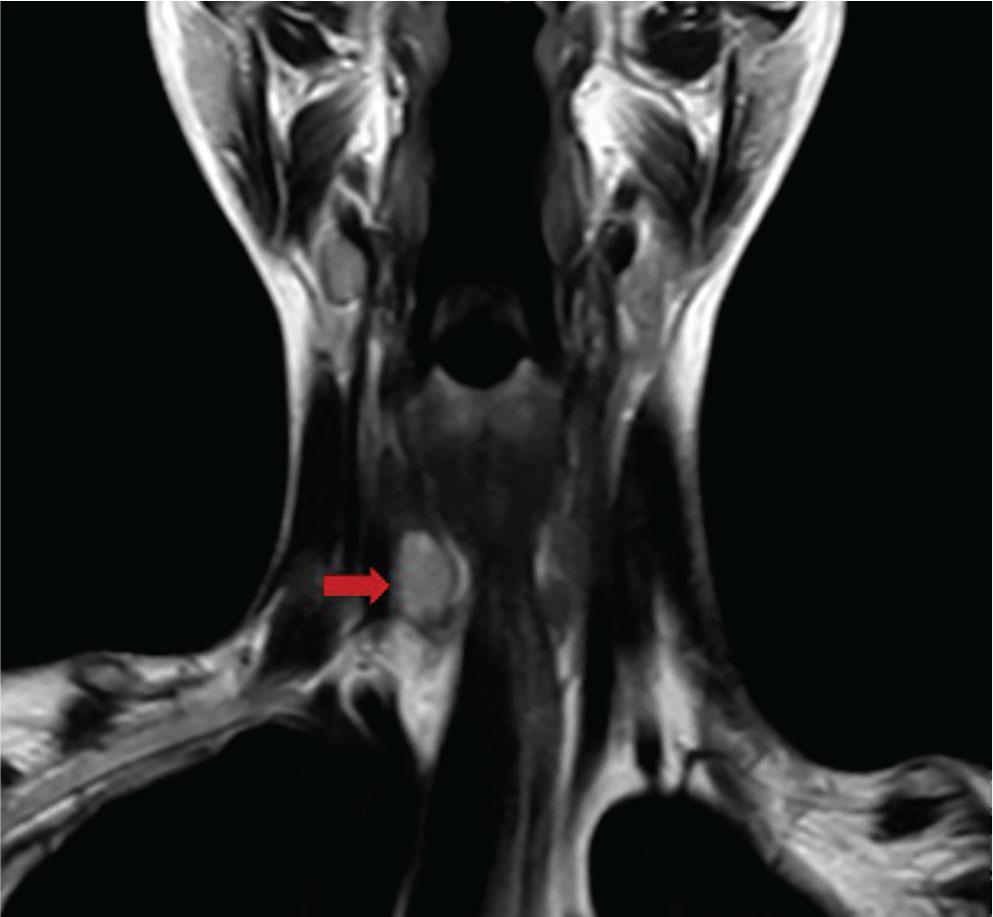
Magnetic resonance imaging neck showing a mass adjacent to the right lobe of the thyroid at its inferior pole (red arrow).
Further workup was conducted to rule out multiple endocrine neoplasia and concomitant thyroid disease. This turned out to be negative for multiple endocrine neoplasia, and fine needle aspiration of the thyroid nodule showed a Bethesda category III lesion.
Bone densitometry with Dual Energy X-Ray Absorptiometry (DXA) results were below the expected range for age. Left radius 33%, Z-score was −4.4.
After reviewing all imaging and reports, it was decided to get a complete thyroidectomy and parathyroidectomy, as images were unable to locate hyper hyperfunctioning parathyroid adenoma.
The patient underwent total thyroidectomy and subtotal parathyroidectomy (Partial left superior parathyroid gland was preserved). Operative findings showed subtle nodularity along the thyroid gland, but no discrete mass was seen. She remained stable throughout the admission and was discharged on the 3rd postoperative day. Her calcium levels were within normal ranges on discharge.
Histopathology of the surgical specimen turned out to be “parathyroid adenoma/hyperplasia with normal thyroid parenchyma.”
On follow-up after 3 weeks to the endocrinology clinic, her calcium levels were checked, which turned out to be 5.36 mg/dL (Normal range: 8.5 – 10.5 mg/dl). Her phosphorus was also on the lower side, 1.91 mg/dL (Normal range: 2.5 – 4.5 mg/dl). Magnesium, potassium, and renal functions were normal. PTH-Intact was < 4.6 pg/mL (18.5 – 88 pg/dl). She was admitted through the emergency, and calcium infusion was started. She had a prolonged inpatient stay due to hypocalcemia, which was managed with calcium infusion, vitamin D supplements, and thiazide diuretics.
The patient was discharged when calcium levels were in acceptable ranges; however, later she revisited the emergency multiple times due to low calcium levels because of non-compliance with calcium supplements.
She is currently on a high dose of calcium supplements, on endocrine follow-up, and living a normal life with good functional status.
Incidence of primary hyperparathyroidism varies among different populations [5, 6, and 7]. There is a rising trend in the incidence of primary hyperparathyroidism, more in countries outside North America and Europe, due to increasing serum calcium level measurements.
Brown Tumors are rare manifestations, reported in 3% patients in primary hyperparathyroidism and 2% in secondary hyperparathyroidism [8]. Prolonged undiagnosed hyperparathyroidism can lead to increased osteoclastic turnover of bones, which causes the formation of brown tumors. Due to rapid bone loss, there is hemorrhage and deposition of hemosiderin within the fibrous tissue of bone, which gives it a reddish-brown color [9].
Radiologically, they appear as osteolytic lesions. Their differential diagnosis includes bone metastasis, amyloid cysts, chondroma, aneurysmal bone cyst, osteosarcoma, and Giant cell tumors.
Primary hyperparathyroidism is the third most common endocrine disease after diabetes and thyroid disease [9]. There are a few guidelines that help us navigate through the management of primary hyperparathyroidism [10]. Only definitive management of primary hyperparathyroidism is surgery. Before surgery, it is recommended to establish biochemical evidence of primary hyperparathyroidism. Workup is advised if someone has symptoms of hypercalcemia, such as thirst, polyuria or constipation, renal stones, osteoporosis, or a previous fragility fracture. Albumin-adjusted calcium levels are measured, and if they are raised, parathormone levels, creatinine, and 25-hydroxyvitamin D levels are measured. 24-hour urinary calcium levels should also be measured in patients undergoing workup for primary hyperparathyroidism to rule out Familial hypocalciuric hypocalcemia. Once biochemical evidence is at hand, it is recommended to get abdominal imaging to rule out nephrocalcinosis and pancreatic calcification, a DXA (dual-energy X-ray absorptiometry) scan of the lumbar spine, distal radius, and hip, and assess other symptoms and comorbidities. Parathyroid imaging is only advised to locate an abnormal parathyroid gland once the decision of surgery is made. Symptomatic patients are expected to derive clear benefits from curative parathyroidectomy. Observation and pharmacologic therapy are less effective and less cost-effective than surgery, even when the patient is considered asymptomatic [11]. Primary hyperparathyroidism causes a decrease in BMD, most pronounced at cortical bone sites, such as the distal third of the radius. Parathyroidectomy improves BMD and appears to reduce fracture rate, even for normal or osteopenic bone [12].
There are no clear guidelines for the management of the Hungry Bone Syndrome, but treatment is aimed at replacing the severe calcium deficit and at restoring normal bone turnover with high doses of calcium and active metabolites or vitamin D analogues. Proper correction of magnesium deficiency and normalization of bone turnover are required for the correction of hypocalcemia, which can last for several months after successful surgery [13]. Primary hyperparathyroidism is essentially a benign condition that can be managed completely if diagnosed at the right time. It should be considered as a differential diagnosis in all patients presented with cystic bone lesions to avoid missing a completely treatable cause. Severe hypocalcemia, post-subtotal parathyroidectomy, is a life-threatening condition. Clinical and biochemical features of hungry bone syndrome should be kept in mind post-operatively to avoid any sinister outcome.