
Craniospinal axis radiotherapy (CSI) plays a vital role in managing central nervous system (CNS) malignancies, especially those with a high propensity for leptomeningeal spread, such as medulloblastoma and primitive neuroectodermal tumors (PNET) (1,2,3). Traditionally, CSI has been administered using three-dimensional conformal radiotherapy (3D-CRT), which typically involves two opposing lateral cranial fields and one or two posterior spinal fields (4).
However, this conventional technique presents several challenges, particularly in field matching, dose uniformity, and the management of steep dose gradients. The junctions between the cranial and spinal fields are especially susceptible to hot spots (areas of overdose) and cold spots (areas of underdose) (4). Additionally, this method is associated with significant acute toxicity, with hematological side effects reported in approximately 25–30% of patients (5).
Recent advancements in radiotherapy techniques, particularly the widespread adoption and enhanced efficiency of Intensity-Modulated Radiation Therapy (IMRT) and Volumetric Modulated Arc Therapy (VMAT) have significantly improved the delivery of cranio-spinal irradiation (CSI). These advanced techniques offer unique capabilities that overcome many of the limitations associated with conventional conformal radiotherapy. Through dynamic beam modulation and continuous arc motion, IMRT and VMAT enable seamless target coverage, improved dose homogeneity, and better sparing of critical organs at risk. As a result, they have become increasingly popular for CSI due to their ability to deliver highly conformal and precise dose distributions (6,7).
Although existing studies have demonstrated the technical advantages of VMAT for cranio-spinal irradiation (CSI), there remains a significant gap in the literature regarding its real-world application in resource-constrained settings, particularly for pediatric patients in low- and middle-income countries (LMICs) (8). This study seeks to address this by evaluating the clinical and dosimetric performance of CSI-VMAT in a tertiary care center in Pakistan, providing context-specific evidence that contributes to a more globally inclusive understanding of advanced radiotherapy practices. Shaukat Khanum Memorial Cancer Hospital is one of the few centers in the country equipped with advanced infrastructure and state-of-the-art linear accelerator-based technologies, including Volumetric Modulated Arc Therapy (VMAT) and Intensity-Modulated Radiation Therapy (IMRT). The hospital also has the capability to provide anesthesia services for young pediatric patients, enabling the safe and effective delivery of complex radiotherapy treatments in this vulnerable population.
This study reports our experience with the CSI VMAT technique, including clinicopathological and dosimetric parameters. Evaluation parameters include conformity and homogeneity indices, planning target volume (PTV) coverage, and organ-at-risk (OAR) sparing. In addition, the study reports on acute toxicities and patient outcomes, including disease-free survival (DFS).
Following Institutional Review Board (IRB) approval, a retrospective analysis was conducted of the first 113 adult and pediatric patients treated with volumetric modulated arc therapy for craniospinal irradiation (VMAT-CSI) at Shaukat Khanum Memorial Cancer Hospital and Research Centre since the technology’s implementation in 2019.
Patients were positioned in the supine or prone position and immobilized using a five-point thermoplastic mask and a dedicated headrest. An indexed vacuum bag was used to immobilize the lower body, ensuring a reproducible pelvic tilt and minimizing anteroposterior curvature of the spine. Arms were positioned alongside the thighs in a relaxed, comfortable manner, with space between the body.
Computed tomography (CT) markers and tattoos were placed at the midline of the superior skull, upper spine, mid-spine, and lower spine to aid in reproducibility. Lateral CT markers were also positioned at the level of the mandible and pelvis.
All patients underwent simulation on a large-bore CT scanner, acquiring images with 3-mm slice thickness from the vertex to the sacrum. Planning CT scans were co-registered with diagnostic magnetic resonance imaging (MRI) for improved delineation of the primary tumor and adjacent structures.
Patients with standard-risk Medulloblastoma (1) were treated with a CSI dose of 23.4 Gy followed by a boost dose of 54–55.8Gy, at the physician’s discretion. Those with high-risk disease (1) received a dose of 36Gy to the craniospinal axis, followed by a boost of 54–55.8 Gy. Spinal mets were treated with a boost of 45 – 50.4Gy
A radiation oncologist delineated the clinical target volume (CTV), which included the whole brain, cribriform plate, temporal lobes, pituitary fossa, meninges, and the entire spinal cord as determined by the extent of Cerebrospinal fluid (CSF) on the MRI scan. The spinal CTV also included lateral extensions along the nerve roots.
An isotropic margin of 5 mm was added to the CTV to generate the planning target volume (PTV).
The organs-at-risk (OARs) for VMAT craniospinal irradiation (CSI) were contoured for treatment optimization and dose evaluation in accordance with established consensus guidelines (9). The contoured OARs included, but were not limited to, the eyes and lenses, parotid glands, lungs, kidneys, liver, heart, and gonads. All contours were reviewed and approved by the treating radiation oncologist to ensure consistency and adherence to institutional standards. Vertebral bodies in all pediatric patients received a homogenous dose of a minimum of 18Gy.
Volumetric modulated arc therapy (VMAT) plans were developed using a two- or three-isocenter technique, depending on the length of the planning volume. Each isocenter was treated with 360° arcs of 6 MV photon beams, with anterior lens avoidance, when the plan was optimized for the supine position; for the prone position, two partial arcs were used to create the plans.
A minimum overlap of 2 cm was maintained at the field junction between the isocenters to enable auto feathering and minimize hotspot formation.
To ensure reproducibility and reduce mechanical as well as patient setup uncertainties, the isocenters were aligned along the craniospinal axis, differing only in their superior-inferior (Y-axis) positioning.
Treatment planning and simultaneous optimization across both isocenters were performed using the Varian ARIA Eclipse treatment planning system, version 15.
The planning goal was to ensure that at least 95% of the planning target volume (PTV) received 100% of the prescribed dose for both CSI and the boost dose.
Plan quality was assessed using dose-volume metrics such as V95%, V107%, and V110% in both CSI PTV and Boost PTV, alongside conformity (CI) and homogeneity indices (HI) whore the formula is mentioned below:
TVPIV = Target volume covered by the prescription isodose
TV = Target volume
PIV = Prescription isodose volume
D2% = Dose received by 2% of the target volume (near-maximum dose)
D98% = Dose received by 98% of the target volume (near-minimum dose)
D50% = Median dose to the target
Patients were evaluated weekly during radiotherapy with focused clinical examinations and toxicity assessments using the Common Terminology Criteria for Adverse Events (CTCAE) v5.0. Particular attention was given to radiation-related toxicities, including dermatologic, gastrointestinal, hematologic, and neurological effects. A complete blood count (CBC) was performed weekly to monitor for treatment-related myelosuppression.
At 6 weeks post-radiotherapy, patients underwent a comprehensive assessment to evaluate acute radiation-induced toxicity. Long-term follow-up was subsequently conducted in collaboration with the pediatric medical oncology team, focusing on the detection and management of late effects of craniospinal irradiation, including endocrine, neurocognitive, and growth-related sequelae.
This retrospective study was approved by the Institutional Review Board (IRB) of Shaukat Khanum Memorial Cancer Hospital and Research Center, Lahore, Pakistan (IRB No. EX-24-06-21-01). The requirement for informed consent was waived owing to the retrospective design and use of anonymized data. All procedures performed in this study were conducted in accordance with the ethical standards of the institutional research committee and with the principles outlined in the Declaration of Helsinki (as revised in 2013).
A total of 113 patients diagnosed with medulloblastoma were included in this study, with treatment spanning from January 2018 to December 2024. The median age at diagnosis was 12 years, ranging from 4 to 37 years. Of the cohort, 76 patients (67.3%) were pediatric, while 37 (32.7%) were adults. The male-to-female ratio was 1.6:1. (Table 1).
Biodemographic and tumor characteristics of the study population
| Median Age years (range) | 12 (4 –37) |
| Pediatric (below 18 years) | 76 (67.3%) |
| Adult (above 18 years) | 37 (32.7%) |
| Male: Female | 70:43 |
| Risk Stratification | |
| High Risk | 78 (69.4%) |
| Standard Risk | 35 (30.6%) |
| Extent of surgery | |
| GTR/NTR | 43 (38.1%) |
| STR | 70 (61.9%) |
| CSF | |
| positive | 16 (14.2%) |
| negative | 97 (85.8%) |
| Time between surgery and RT | |
| <6 weeks | 69 (61.1%) |
| >6 weeks | 44 (38.9%) |
| Concurrent chemotherapy | |
| yes | 76 (67.3%) |
| no | 37 (32.7%) |
| Toxicity (Grade 2 and Above) | |
| Bone Marrow Suppression | 13 (11.5%) |
| Esophagitis | 12 (10.6%) |
| Nausea/vomiting | 12 (10.6%) |
| Weight loss | 10 (8.8%) |
| Diarrhea | 5 (4.4%) |
| Vision changes | 2 (1.8%) |
GTR = Gross total resection, NTR= near total resection, STR= subtotal resection, RT= radiotherapy, CSF = cerebrospinal fluid.
Surgical resection was categorized based on residual tumor volume, with gross total or near-total resection (GTR/NTR), defined as less than 1.5 cc of residual disease, achieved in 43 patients (38.1%). The remaining patients underwent subtotal resection (STR). Cerebrospinal fluid (CSF) cytology was positive in 16 patients (14.2%) and negative in 97 patients (85.8%). Patients were stratified into risk groups: 78 (69.4%) were high-risk, and 35 (30.6%) were standard-risk.
The interval between surgery and initiation of radiotherapy was less than six weeks in 69 cases (61.1%). Concurrent chemotherapy during radiotherapy was administered to 66.7% of patients, while 33.3% received radiotherapy alone.
The mean planning target volume (PTV) length, that is, the length of volume from the cranial-most slice of the PTV to the last spinal PTV slice on CT scan, was 62.4 ± 9.78 cm, with a range of 46.8 to 81.4 cm. The mean PTV coverage was 96% ± 1.23%, with a mean PTV D99% of 93.8% +/− 2.34 and a mean PTV D1% of 106% +/− 1.45. The majority of patients (90.3%) required more than two isocenters for adequate craniospinal coverage; only 9.7% were treated with two isocenters. The median conformity index (CI) was 1.02 (range: 0.98–1.08), and the homogeneity index (HI) was 0.10 (range: 0.09–0.14). The median number of arcs per treatment plan was five (range: 3–7). Regarding patient positioning, 78.7% were treated in the supine position, and 21.2% in the prone position. Organs-at-risk doses are detailed in Table 2. The median follow-up duration was 15 months, ranging from 5 to 56 months. The two-year disease-free survival (DFS) rate was 76% (Figure 1).
Dosimetric characteristics of the study population
| CSI dose (Gy) | 23.4/36 |
| Boost spine (Gy) | 14.4–30.6 |
| Boost to primary (Gy) | 54–55.4 |
| Mean PTV coverage | 96% +/− 1.23 |
| PTV D99 | 93.8% +/− 2.34 |
| PTV D1 | 106% +/− 1.45 |
| Number of isocenters | |
| 2 | 11 (9.7%) |
| >2 | 102 (90.3%) |
| Conformity index (CI) | 1.02(0.98–1.08) |
| Homogeneity index (HI) | 0.1 (0.14–0.09) |
| Mean Length (PTV) | 62.4 +/− 9.78 |
| Median ARC | 5 (3–7) |
| Left Kidney Mean | 6.5Gy +/− 2.32 |
| Right Kidney Mean | 6.5Gy +/− 2.32 |
| V19 Liver mean | 0.47cc +/− 1.02 |
| Heart Mean | 6.5Gy +/−2.61 |
| Bowel Mean | 6.1Gy +/− 3.56 |
| Lung mean | 7.2Gy +/− 1.83 |
| Setup Position | |
| Prone | 24 (21.2%) |
| Supine | 89 (78.7%) |
| Median ARC | 5 (3–7) |
CSI = craniospinal irradiation, PTV = planning target volume.
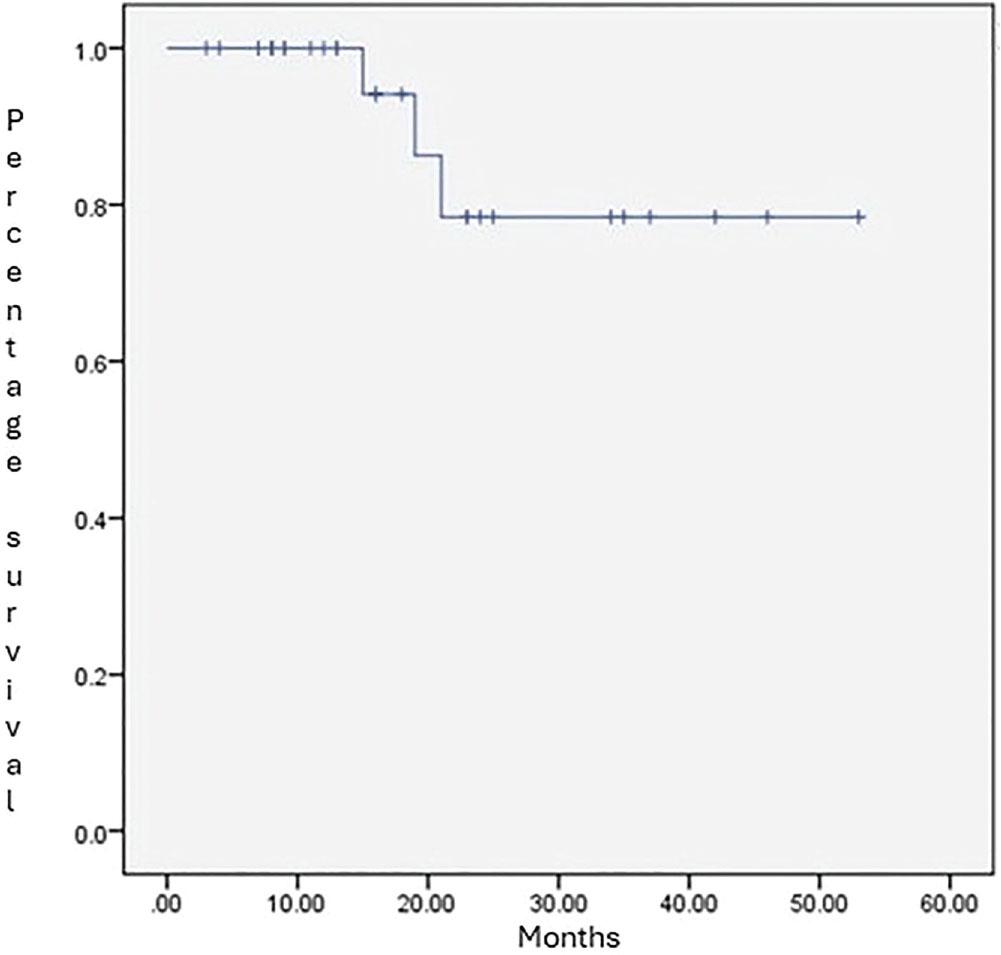
The two-year disease-free survival (DFS) rate of the study population.
Acute radiotherapy-related toxicities occurring during and after 6 weeks post-treatment were generally limited to grade 1. Grade 2 or above Esophagitis occurred in only 11% of patients, bone marrow suppression in 12%, nausea and vomiting in 10%, and weight loss in 9%. Less frequent side effects included grade 2 diarrhea (5%) and vision changes (2%).
In this series of 113 patients with medulloblastoma treated between January 2019 and December 2024, we observed a 2-year disease-free survival (DFS) rate of 76% with a median follow-up of 15 months. While direct comparisons with historical data of longer follow-up are limited, these early results are consistent with previously reported 5-year progression-free survival (PFS) rates of approximately 79–83% in pediatric trials combining reduced-dose craniospinal irradiation (CSI) with chemotherapy (10,11). The extent of resection and metastatic status at diagnosis remain critical prognostic factors; gross total or near-total resection (GTR/NTR) was achieved in about half of our cohort, with 13.3% presenting with metastases. Though other studies have reported local control rates exceeding 90%, largely independent of risk group or resection extent (12), our cohort comprised a predominance of high-risk patients (69.4%), highlighting the generally more challenging prognostic context.
Only 30% of patients started radiotherapy within 6 weeks post-surgery, despite evidence that early initiation of radiotherapy (within 6–7 weeks) is associated with improved outcomes, whereas delays beyond 7 weeks correlate with poorer prognosis (10). This is was mainly due to delayed referrals to our center post-surgery. Concurrent chemotherapy during radiotherapy was administered to two-thirds of patients, while adjuvant systemic therapy was given to approximately 40%. Previous trials have demonstrated that combining radiotherapy with chemotherapy, particularly with concurrent administration, significantly improves event-free and overall survival, especially in high-risk medulloblastoma (11,12). The observed 2-year DFS of 76% in our cohort, despite delayed radiotherapy initiation in most cases, is encouraging but suggests room for optimizing treatment timing and coordination.
The dosimetric analysis of our study demonstrated high-quality treatment planning, as reflected in our coverage, conformity, and homogeneity indices. The technical complexity was underscored by the fact that the majority of patients required more than 2 isocenters for adequate craniospinal coverage. These findings align with other reports demonstrating that advanced radiotherapy techniques such as volumetric modulated arc therapy (VMAT) or helical tomotherapy offer precise target conformity and effective sparing of organs at risk (OARs), including the heart, lungs, kidneys, and liver, with mean doses of approximately 6–7 Gy to these structures (12,13,14). Our results further support VMAT as a viable treatment technique for CSI.
Acute radiotherapy-related toxicities in our cohort were generally limited to Grade 1 on the CTCAE scale, and they were consistent with manageable side effect profiles in contemporary CSI protocols (15,11). The low frequency of diarrhea and rare occurrence of vision changes further support the acceptable safety profile of treatment in this cohort. These findings suggest that CSI using the VMAT technique can achieve effective disease control while maintaining manageable acute toxicity, allowing most patients to complete treatment without significant interruption.
Although our median follow-up of 15 months limits the assessment of late toxicities, existing long-term data from pediatric and adult medulloblastoma cohorts emphasize the importance of monitoring for neurocognitive decline, endocrine dysfunction, cardiomyopathy, and secondary malignancies (10,17,16). Adult studies with longer follow-up report 5-year PFS upwards of 85–95%, albeit with significant late effects including cognitive dysfunction, anxiety, depression, and ototoxicity (10). Higher boost doses to the posterior fossa have also been associated with increased neuropathy, endocrine sequelae, and cognitive decline (11).
Several limitations of this study must be acknowledged. Its retrospective, single-institution design introduces potential biases, including selection bias and incomplete data capture, limiting the generalizability of findings. The relatively short median follow-up restricts the evaluation of late toxicities and secondary malignancies, which often manifest years after treatment (16). Variability in systemic therapy administration and radiotherapy initiation timing may have influenced outcomes.
VMAT-based CSI is a feasible and effective treatment modality for medulloblastoma in a resource-constrained setting, providing superior dosimetric outcomes with manageable toxicity. These findings support the broader adoption of advanced radiotherapy techniques, such as VMAT, in similar clinical environments.