
According to the global cancer statistics 2022, Esophagus is the 11th most prevalent cancer type around the globe, accounting for 2.6% of all new cancer cases, and is ranked 7th in cancer-related mortality with a frequency of 4.6% [1]. The most common type of esophageal cancer (EC) globally is Esophageal Squamous Cell Carcinoma (ESCC), which accounts for above 90% of all cases in Eastern Asia [2]. It is more prevalent in developing countries and is often related to micronutrient deficiencies, like vitamin C, E, and folate, and lifestyle habits like smoking, alcohol, hot beverages, and nitrosamines consumption [3]. However Esophageal Adenocarcinoma (EAC) is more common in developed countries [4] and is associated with tobacco consumption, obesity, and gastroesophageal reflux disease. [3]. This type is more common in men, with a male-to-female ratio of 9:1, potentially influenced by hormonal factors [5].
In Pakistan literature from different parts of the country exhibits regional variation. In Karachi, this cancer ranked as 7th most frequent in males (6.2/100,000) and 5th in females (7.0/100,000). In contrast, in Quetta, a significantly higher prevalence was reported in males (25.5/100,000) than in females (23.4/100,000) making it the highly prevalent region for this cancer type with most patients diagnosed in the advanced stage [6]. In Punjab and Khyber Pakhtunkhwa ESCC is predominant (account for 92.5% of cases) and is more prevalent in male gender [7,8].
Chemo-radiotherapy is commonly used to shrink the tumor pre-operatively, however, it is related to increased risk of esophageal perforation in 5.6% to 33% of the cases, especially in advanced stage cancer [9]. Old patients (age <60–65 years) and those with ESCC are more prone to esophageal perforation, and develop complications like empyema, mediastinitis, and sepsis, which is associated with mortality in 9% to 26% of the cases [10,11].
Surgical repair involves direct closure and drainage is the conventional treatment option for esophageal perforation, [12] however, it is less feasible in advanced stages due to disease progression and patient frailty, making less invasive approaches preferable [11]. The preferred minimally invasive option for sealing perforation and correcting oral intake involves esophageal stenting (ES) with self-expandable metal stents (SEMS) [13]. Studies demonstrate a high technical success of self-expandable metal stents SEMS with median stent patency of 38.5 days and a median survival of 40 days. Initial placement success is considered the only predictor of better survival. However, the procedure is not very successful in advance stage cancer patients. Overall the esophageal SEMS help in symptoms relief and improve quality of life [14].
Esophageal stenting offers a less invasive, more feasible, and cost-effective alternative to other treatment modalities. This study seeks to assess the long-term outcomes of this procedure in patients with esophageal tumor perforation.
This retrospective cohort study was conducted at Shaukat Khanum Memorial Cancer Hospital and Research Center, Peshawar, after obtaining approval from the ethical committee under reference number EX-31-10-24-01, dated 29-11-2024. The record of patients who presented with esophageal tumor perforation from 1st January 2016 to 31st December 2021 was consecutively reviewed through the hospital electronic medical record system from October to December 2024. The inclusion criteria were patients of either gender and age, who perform esophageal stenting for tumor perforation, and those whose date of death is either available in Hospital Electronic System or was traced via the available demographics. Patients who were managed either conservatively or with another procedure for tumor perforation and wrong alert of tumor perforation were excluded. A total of 600 patients had presented with esophageal among which 80 patients were presented with tumor related esophageal verified by imaging (CT, MRI, or PET) and manage with esophageal stenting was included in the study.
The esophageal tumor perforation or rupture is defined as a hole or tear through the wall of the esophagus that is confirmed with CT, MRI, and/or PET scans [15]. The data regarding the patient’s body mass index (BMI), date of CT/MRI/PET confirming perforation, stage of esophageal cancer, date of stenting, BMI at the time of stenting, visit after stenting and live status after the last visit. The self-expandable metallic stents, specifically the HANARO stents manufactured by MI Tech Korea, were utilized in this procedure in all patients. The stents used were fully covered, with diameters 18 mm and lengths between 130 mm and 170 mm. All the data was recorded in a predesigned proforma. The collected data was entered into an Excel sheet.
The data was analyzed using SPSS-25. Mean ± standard deviation or Median(IQR) was calculated for numerical/quantitative variables after checking normality through the Shapiro-Wilk test. Frequencies and percentages were calculated for categorical/qualitative variables. Chi-square test was applied keeping the p-value ≤ 0.05 as statistically significant.
A total of 80 patients were analyzed in our study who presented with esophageal perforation and treated with esophageal stenting. The mean age of the patients was 46.98±11.615 years, ranging from 23 to 75 years, predominantly male 45 (56.3%) and 35 (43.8%) was female. The median BMI is 18.25(IQR=5.21) kg/m2, ranges from 11.68 to 32.47 kg/m2. Most of the patients in our study is from Afghanistan 38(47.5%), followed by Punjab 19(23.8%), Khyber Pakhtunkhwa 13(16.3%), Baluchistan 6(7.5%), Sindh 3(3.8%) and Azad Kashmir 1(1.3%). Squamous cell carcinoma was the predominant histological type 74(92.5%), followed by adenocarcinoma 4(5%) and other rare types 2(2.5%). Most patients had advanced disease, with 48(60%) classified as T3 and 15(18.8%) as T4. Nodal involvement N1 and N2 was present in 34(42.5%) each. Majority of patients had no distant metastasis (M0) 57(71.3%). Nearly half 37(46.3%) received both chemotherapy and radiotherapy, while 32(40%) had only chemotherapy. The median stent insertion to the end of study was 83 days, ranging from 1 day to over 7 years. Survival outcomes were poor, with 76 (95%) deceased and only 4(5%) alive Table 1.
Patients Characteristics, histology, staging, treatment and outcome.
| Histology | n (%) | Total | |
|---|---|---|---|
| Squamous Cell Carcinoma | Squamous Cell Carcinoma | 67 (83.8%) | 74 (92.5%) |
| Moderately Differentiated Squamous Cell Carcinoma | 5 (6.3%) | ||
| Well-Differentiated Squamous Cell Carcinoma | 2 (2.5%) | ||
| Adenocarcinoma | Adenocarcinoma | 3 (3.8%) | 4 (5%) |
| Poorly Differentiated Adenocarcinoma | 1 (1.3%) | ||
| Other Types | High-Grade Neuroendocrine Carcinoma | 1 (1.3%) | 2 (2.5%) |
| Mucoepidermoid Carcinoma and Gastroesophageal Junction (GOJ) Tumor | 1 (1.3%) | ||
| Staging | |||
| T | Tumor invades lamina propria, muscularis mucosae, or submucosa (T1) | 1 (1.3%) | |
| Tumor invades muscularis propria (T2) | 16 (20%) | ||
| Tumor invades adventitia (T3) | 48 (60%) | ||
| Tumor invades adjacent structures (T4) | 15 (18.8%) | ||
| N | No regional lymph node metastasis (N0) | 12 (15%) | |
| Metastasis in 1–2 regional lymph nodes (N1) | 34 (42.5%) | ||
| Metastasis in 3–6 regional lymph nodes (N2) | 34 (42.5%) | ||
| M | No distant metastasis (M0) | 57 (71.3%) | |
| Distant metastasis present (M1) | 23 (28.7%) | ||
| Chemotherapy and Radiotherapy | |||
| No Chemotherapy or Radiotherapy | 11 (13.8%) | ||
| Combined Chemotherapy and Radiotherapy | 37 (46.3%) | ||
| Only Chemotherapy | 32 (40%) | ||
| Median duration of stent insertion to end date of the study | 83 days (min=1 day, max=7.24 yeras) | ||
| Survival status | |||
| Alive | 4 (5%) | ||
| Dead | 76 (95%) | ||
The comparative analysis of patients who survived versus those who did not following esophageal tumor perforation showed no statistically significant associations between survival and key tumor characteristics. The T stage distribution, nodal involvement, presence of metastasis, and histological type did not differ significantly between the two groups (p > 0.05 for all variables). Although most decedents occurred in patients with advanced T3 stage (60.5%), nodal involvement (N1/N2), and metastasis (28.9%), these trends were not statistically significant, suggesting that these factors alone may not independently predict mortality in these patients Table 2.
T-Stage and Nodal Involvement association with survival.
| Variable | Category | Alive | Death | p value |
|---|---|---|---|---|
| T Stage | Tumor invades lamina propria, muscularis mucosae, or submucosa (T1) | 0 (0.0%) | 1 (1.3%) | 0.967 |
| Tumor invades muscularis propria (T2) | 1 (25.0%) | 15 (19.7%) | ||
| Tumor invades adventitia (T3) | 2 (50.0%) | 46 (60.5%) | ||
| Tumor invades adjacent structures (T4) | 1 (25.0%) | 14 (18.4%) | ||
| Total | 4 (100.0%) | 76 (100.0%) | ||
| Nodal Involvement | No regional lymph node metastasis (N0) | 1 (25.0%) | 11 (14.5%) | 0.726 |
| Metastasis in 1–2 regional lymph nodes (N1) | 2 (50.0%) | 32 (42.1%) | ||
| Metastasis in 3–6 regional lymph nodes (N2) | 1 (25.0%) | 33 (43.4%) | ||
| Total | 4 (100.0%) | 76 (100.0%) | ||
| Metastasis | No distant metastasis (M0) | 3 (75.0%) | 54 (71.1%) | 0.675 |
| Distant metastasis present (M1) | 1 (25.0%) | 22 (28.9%) | ||
| Total | 4 (100.0%) | 76 (100.0%) | ||
| Histology | Adenocarcinoma | 0 (0.0%) | 4 (5.3%) | 0.843 |
| Squamous Cell Carcinoma | 4 (100.0%) | 70 (92.1%) | ||
| Other types | 0 (0.0%) | 2 (2.6%) | ||
| Total | 4 (100.0%) | 76 (100.0%) | ||
P value is calculated through chi-square test/Fisher Exact test based on cell count, p value <0.05 is considered significant.
The Kaplan-Meier survival analysis of 80 patients (Fig. 1) who underwent esophageal stenting for tumor perforation shows a rapid decline in survival probability, with approximately 40% of patients surviving by around 100 days. The median survival time, estimated visually from the curve where the cumulative survival drops to 0.5, is approximately 200 days. By roughly 500 days, the survival probability decreases further to about 20%. Beyond this point, the decline in survival becomes more gradual, with approximately 10% of patients surviving to around 1000 days. While some patients survived beyond this timeframe, the survival probability continues to decrease, reaching approximately 5% by 2000 days. The curve plateaus at around 5% survival after approximately 2500 days, indicating that a small proportion of patients survived for a considerable duration within the study period. The median survival of approximately 200 days was observed, although a small subset of patients experienced longer-term survival.
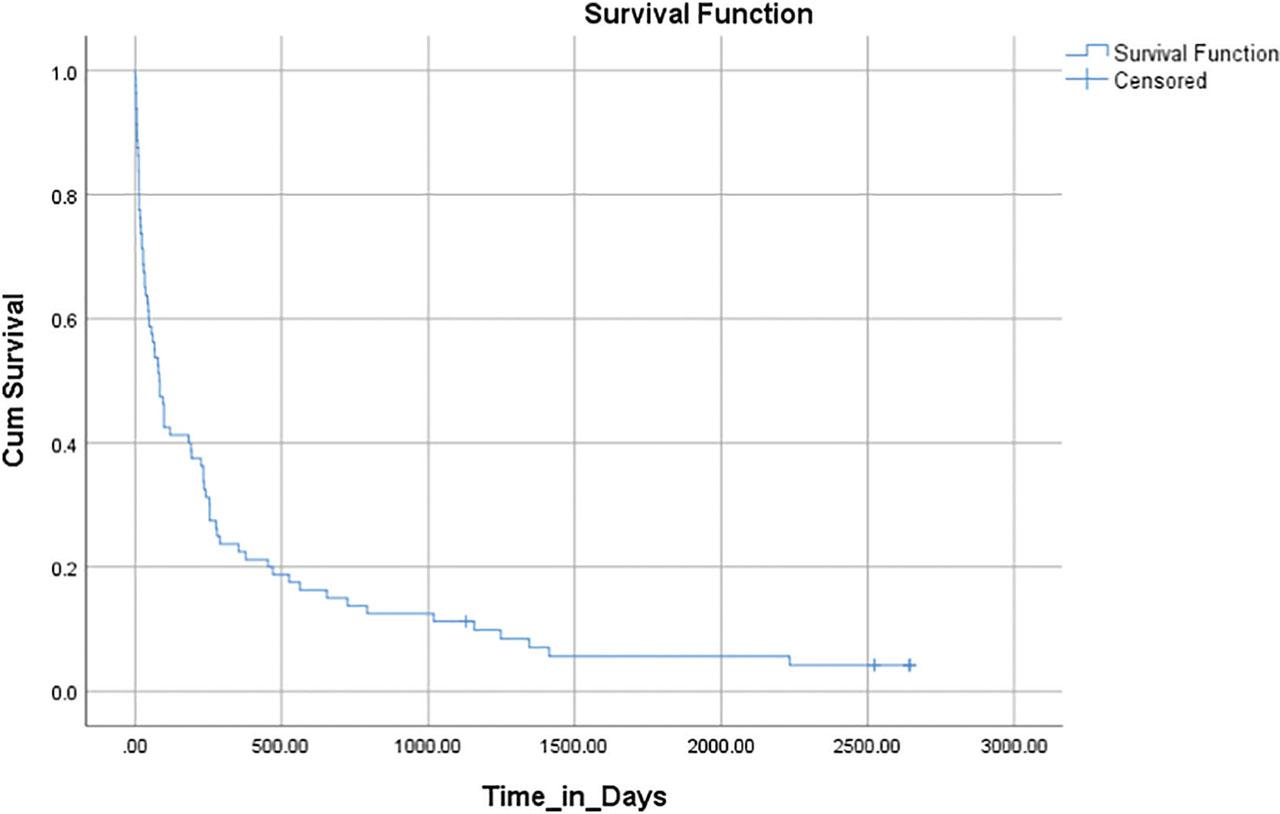
Kaplan-Meier survival analysis of esophageal stenting patients for tumor perforation.
The findings highlight the efficacy of esophageal stenting (ES) in managing esophageal tumor perforation by analyzing clinical outcomes, survival rates, and factors influencing prognosis among patients undergoing stent placement for tumor-related esophageal perforations.
The results indicate that ES is a viable palliative approach for managing tumor perforations, particularly in cases where surgical intervention is not feasible. The median duration of stent insertion to the end of study of patients was 83 days, ranging from 1 day to over 7 years, which is higher from the previous studies that report a median stent patency of approximately 38.5 days [13].
Ullah et al. (2023) [16] analyzed 11 cases of esophageal perforation managed with emergency esophagectomy (EE) at the same center from 2009 to 2019, reporting a 90-day mortality of 27.3% and a median overall survival (OS) of 6.37 months, emphasizing the importance of early surgical intervention (<24 hours) in improving survival. In contrast, our findings indicate that esophageal stenting (ES) provides temporary symptom relief, with a median stent insertion duration to the end of the study was 83 days, but survival outcomes remain poor (mortality: 95%, overall survival: 5%). Their studies identified tumor stage and nodal involvement as key prognostic factors, however no such relation was identified in our data. Also histological subtype was not significantly linked to survival in our study (p=0.843), whereas Ullah et al. suggested tumor differentiation (moderate to poor) influenced prognosis [16].
The findings of this study align with existing literature regarding esophageal stenting as a palliative intervention for advanced esophageal cancer, particularly in cases of inoperable stage III and IV cancer. In alignment with Chaiyakul et al. (2024), [14] who reported stent utilization in 62.8% of stage IV and 37.2% of stage III cases, our research confirms that nodal involvement and tumor stage serve as significant prognostic indicators, with T3 tumors exhibiting a death rate of 65.5%. Nodal status significantly influenced prognosis, with decreased survival rate for N1 and N2. This underscores that tumor burden and metastatic dissemination are critical predictors of survival in patients receiving palliative stenting.
Complications related to stenting, including migration, tumor overgrowth, and fistula formation, have been thoroughly documented in the literature [17,18] The reported re-intervention rate of 19.4% per stent placement [17] and the increased risk of perforation following radiotherapy doses exceeding 40 Gy [18] highlight the necessity for careful patient selection and monitoring. Post-stenting chemoradiotherapy has been associated with an increased risk of esophagorespiratory fistulas, [19] however, these factors were not analyzed in our cohort.
A limitation includes the retrospective study design and small sample size. Although esophageal stenting provides symptom relief and improves oral intake, its long-term advantages remain limited due to the progressive characteristics of esophageal cancer. Furthermore, tumour site and treatment modality may influence survival outcomes; however, subgroup analysis by site was not feasible due to small numbers. Future studies can focus on prospective study design with long-term follow-up.
Esophageal stenting serves as a minimally invasive palliative option for esophageal tumor perforation, offering symptomatic relief with limited impact on survival. Outcomes are notably better in early stages of cancer, while advanced stages yield less favorable results. It also prolongs survival, and improves quality of life in cases where surgical intervention is unfeasible.