
Intussusception occurs when one segment of the bowel (the intussusceptum) telescopes into an adjacent segment (the intussuscipiens). It is a rare clinical entity due to the retroperitoneal fixation of the duodenum, which restricts its mobility and reduces the risk of intussusception [1,2]. In adults, it accounts for only 5% of all reported cases and is usually associated with an underlying lesion. Reported causes include benign and malignant tumors such as adenomas, gastrointestinal stromal tumors (GISTs), Brunner’s gland hamartomas, and duodenal duplication cysts; less common etiologies include carcinoid tumors and peptic ulcer disease [3].
In a recent review of 54 cases, adult duodenojejunal intussusception (DJI) was present in 32 (59.3%) cases, and tubovillous adenoma was the underlying cause in only 6/32 (18.8%) patients. Most patients were symptomatic with abdominal pain and vomiting, emphasizing the importance of timely diagnosis [4].
We present a rare case of adult DJI secondary to a periampullary tubulovillous adenoma. This case report discusses the diagnostic evaluation and imaging findings. It also discusses the challenges in the surgical management of adult DJI. Informed consent was taken from the patient regarding the information and pictures.
A 30-year-old woman presented with an 18-month history of dull, non-radiating right hypochondrial pain, episodic non-bilious vomiting, and 10 kg unintentional weight loss. Physical examination was unremarkable. Laboratory tests showed a hemoglobin of 10.3 g/dL, white blood count of 6,290/μL, and platelets of 356,000/μL. The alkaline phosphatase was 905 U/L, and total bilirubin was 0.45 mg/dL. Serum albumin was 3.7 g/dL, and CA 19-9 was mildly elevated (46.5 U/mL). Hepatitis C serology was positive. A prior CT scan of the abdomen demonstrated a long segment DJI with intrahepatic and extrahepatic biliary dilatation secondary to an enhancing periampullary lesion. Endoscopic biopsy revealed a tubulovillous adenoma without high-grade dysplasia.
A repeat contrast-enhanced CT scan revealed a 9 cm duodenojejunal intussusception (DJI) with a 55 × 45 mm enhancing ampullary lesion, causing traction and biliary dilatation without evidence of malrotation (Figures 1A,B). After multidisciplinary team review, surgical resection was recommended based on the lesion’s size, location, and imaging features.

(A) xial CT view demonstrating target sign for intussusception (B) Coronal view with common bile duct traversing the midline (white arrow) towards the left hypochondrium with intussuscepted adenoma (asterisk).
At laparotomy, a mobile periampullary mass was identified. The intussusception was manually reduced, and a duodenotomy was performed, confirming a large, cauliflower-shaped ampullary polyp with a broad base and redundant mucosa (Figure 2). Due to concerns about achieving complete resection, the procedure was converted to a pancreaticoduodenectomy. The postoperative course was uneventful, and the patient was discharged on postoperative day 7.
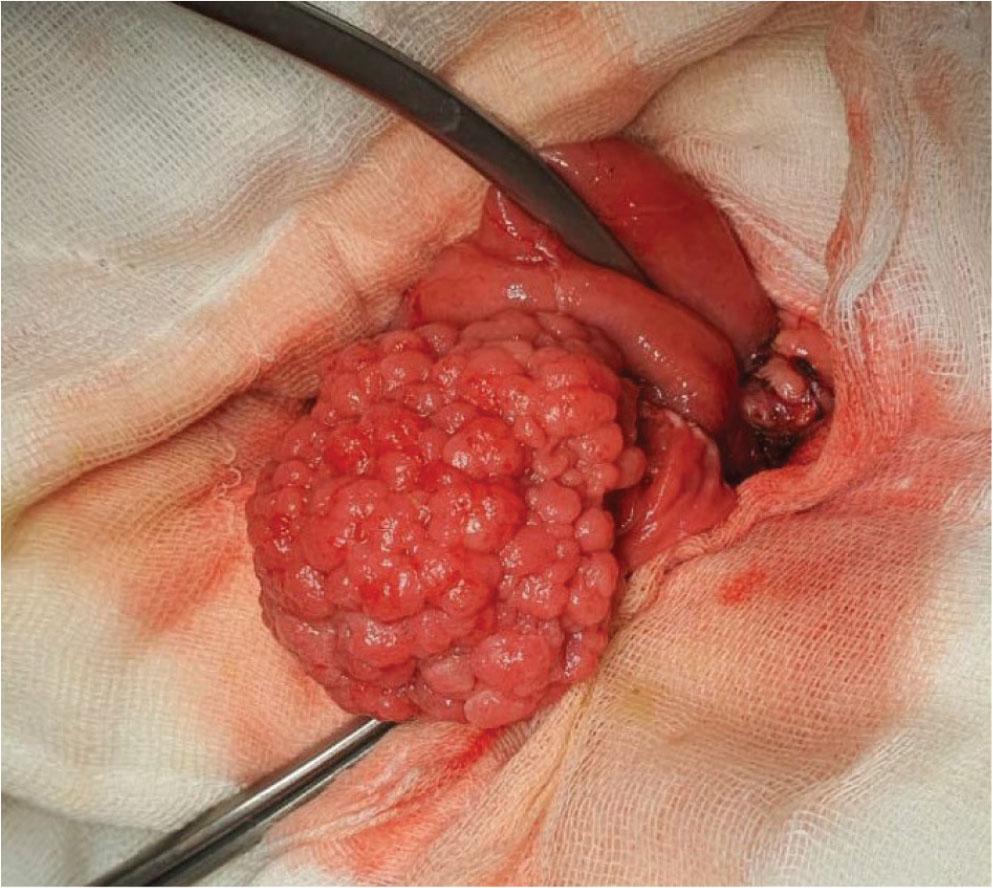
Intra-operative picture of cauliflower shaped large adenoma after duodenotomy.
Histopathological examination confirmed an intestinal-type adenoma with negative resection margins and no evidence of high-grade dysplasia or malignancy. All thirty-three excised lymph nodes were negative for metastasis. After full recovery, the patient began hepatitis C virus (HCV) treatment, one month postoperatively. Over the next 8 weeks, the patient regained weight, had normal laboratory results, and remained clinically well at 15 months of follow-up.
Adult DJI is an uncommon clinical entity that presents unique diagnostic and therapeutic challenges. Although more frequently reported in females, its epidemiological characteristics remain poorly defined due to limited published data. Management is typically individualized, ranging from endoscopic to surgical approaches [4,5].
Contrast-enhanced CT is the diagnostic modality of choice, characteristically demonstrating “target,” “doughnut,” or “sausage-shaped” configurations consistent with telescoping bowel segments [1,2,3]. The pathophysiology of DJI is incompletely understood; in adults, it is most often associated with a structural lead point, including benign or malignant tumors, or less commonly, congenital malrotation or mucosal redundancy [5,6]. In this case, a duodenal adenoma served as the lead point. Prior studies suggest that chronic peristaltic traction, mucosal prolapse, and limited duodenal mobility promote invagination, while retroperitoneal fixation and pancreatic attachments exacerbate it [7,8].
Biliary obstruction in DJI typically results from extrinsic compression rather than direct tumor invasion [6]. In this patient, intermittent compression of the biliary and pancreatic ducts led to ductal dilatation without hyperbilirubinemia, likely due to incomplete obstruction, underscoring the value of radiologic assessment in cases of biochemical cholestasis.
Definitive management usually involves surgical resection, given the risk of obstruction or ischemia and the frequent presence of a pathological lead point [9,10]. While endoscopic resection may be appropriate for mucosal lesions <2 cm, larger or transmural lesions generally warrant surgical excision [3,4]. Among surgical options, ampullectomy is less commonly performed due to diagnostic uncertainty, as intraoperative frozen sections are often superficial and may not reliably exclude malignancy. Pancreaticoduodenectomy (Whipple’s procedure) is preferred when histologic certainty is lacking, offering both oncologic safety and durable outcomes [11,12].
In this case, endoscopic resection was not feasible due to the tumor’s size and significant intussusception. An initial transduodenal ampullectomy was converted to a pancreaticoduodenectomy because of the lesion’s broad base and redundant mucosa, raising concerns of incomplete excision. Given our center’s expertise in hepatopancreatobiliary surgery, Whipple’s procedure was selected as the most definitive option. This approach is consistent with outcomes from high-volume tertiary centers, which report low morbidity and excellent long-term results in similar scenarios [13]. To the best of our knowledge, there are only six reported cases of adult DJI with underlying adenoma as the pathological diagnosis (Table 1).
Summary of published cases reports on DJI.
| Authors | Age/Gender | Chief complaints | Treatment |
|---|---|---|---|
| Chawla et al. [3] | 34/F | vomiting | Segmental duodenal resection preserving the ampulla |
| Hirata et al. [7] | 66/F | whole-body edema and malaise | Pylorus preserving Pancreaticoduodenectomy |
| Kaw et al. [10] | 41/M | abdominal pain | Duodenectomy with polypectomy |
| Huda et al. [14] | 25/F | vomiting and weight loss | Segmental resection and end to end anastomosis |
| Neogi et al. [15] | 37/F | abdominal pain,vomiting | Segmental resection and end to end anastomosis |
| Mangal et al. [16] | 31/F | abdominal pain | Duodenectomy with polypectomy |
Adult DJI is a rare condition usually driven by a structural lead point and best diagnosed with contrast-enhanced CT. Management should be tailored, and pancreaticoduodenectomy provides a definitive option for large or uncertain periampullary lesions, ensuring complete excision and durable outcomes.