
Chromophobe renal cell carcinoma (ChRCC) ranks as the third most prevalent histological variant of renal cell carcinoma (RCC) [1,2]. Numerous studies have shown that the majority of ChRCC patients achieve a favorable prognosis following surgical removal, but a subset may progress to metastatic disease and succumb to RCC [3,4,5,6].
The utility of grading in chromophobe RCC is controversial. The Fuhrman grading system, which primarily assesses nucleolar characteristics, has been argued to lack prognostic significance in this context due to the inherent atypia in chromophobe RCC [3,7,8,9]. A novel grading system, called the chromophobe tumor grading (CTG) scheme and introduced by Paner et al [3], uses three tiers based on nuclear crowding (tight and irregular nuclear grouping), nuclear pleomorphism (variation in nuclear size and shape), and anaplasia (extreme loss of cellular differentiation). The World Health Organization (WHO) and the International Society of Urologic Pathology (ISUP) have recommended that, until a prognostically significant and validated grading system specific to chromophobe RCC is established, chromophobe RCC should not be graded [10].
To date, there is no consensus on the grading system and prognostic utility of tumor grade in chromophobe RCC, and further investigation is required in this regard. Therefore, we conducted a study to determine whether the novel grading system introduced by Paner et al. has prognostic significance and compared it with the Fuhrman grade.
Furthermore, we also compared the prognostic utility of tumor grade with other established independent prognostic factors like pT stage, sarcomatoid features, and tumor necrosis.
This Institutional Review Board (IRB)-approved retrospective analysis included 51 patients who underwent radical nephrectomy for ChRCC at the Department of Urology, Shaukat Khanum Memorial Cancer Hospital and Research Center, Lahore, between group III. All tumors exhibited necrosis; three had less than 10%, whereas one had necrosis ranging from 10% to 20%. All tumors were classified as chromophobe grade 3. Regarding nucleolar grade, one tumor was grade 1, another was grade 2, a third was grade 3, and the last was grade 4. Additionally, one tumor displayed sarcomatoid differentiation, while the remaining three did not. In this subset, TNM stage grouping (I vs. III), the presence of necrosis, and chromophobe tumor grade were significantly associated with CS survival. While Fuhrman nucleolar grade and sarcomatoid differentiation did not show a significant association with CS survival, other factors may influence patient outcomes. (Figures 5–7)
When comparing the chromophobe tumor grading system proposed by Paner et al. with independent prognostic factors, we observed that all grade 3 tumors and the majority of grade 2 tumors exhibited necrosis, whereas no necrosis was present in grade 1 tumors. A similar pattern was noted for sarcomatoid differentiation, which was absent in low-grade tumors (grades 1 2014 and 2019. Excluded from analysis were those patients with multiple tumor histologies and patients who underwent partial nephrectomy and core biopsies. Complete data and follow-up were available in the Hospital Pathology Archives.
Double-blinded slide review was done by two consultant Pathologists having significant experience in the relevant field. We assigned tumor grade according to Fuhrman’s four-tiered nucleolar grade categories and the three-tiered chromophobe tumor grading system proposed by Paner et al. [3]. The Fuhrman nucleolar grading system classifies tumors into four categories: Grade 1 features inconspicuous nucleoli at ×400 magnification with basophilic characteristics (low grade); Grade 2 has clearly visible eosinophilic nucleoli at ×400 magnification (low grade); Grade 3 shows clearly visible nucleoli at ×100 magnification (high grade); and Grade 4 is marked by extreme pleomorphism or rhabdoid morphology, indicating a high grade and the most aggressive form. The novel chromophobe tumor grades were defined as follows: Grade 1 indicated chromophobe RCC with a wide constitutive nuclear range but without nuclear crowding and anaplasia; Grade 2 included geographic nuclear crowding and the presence of nuclear pleomorphism; and Grade 3 involved frank anaplasia or sarcomatoid change [3]. Nuclear crowding was characterized by high nuclear/cytoplasmic density with some nuclei in contact with each other. Anaplasia was defined by a threefold variation in nuclear size and distinct chromatin irregularities. (Figure 1) Additionally, in our study, we excluded sarcomatoid differentiation from the novel chromophobe tumor grading system, treating it instead as a separate independent prognostic marker to prevent any bias when comparing the two grading systems. The assessment of the chromophobe tumor grade involved both low and high-power evaluations of the tumor. It required at least two distinct areas to exhibit features of a certain grade, with the highest grade assigned as the chromophobe tumor grade for the case.
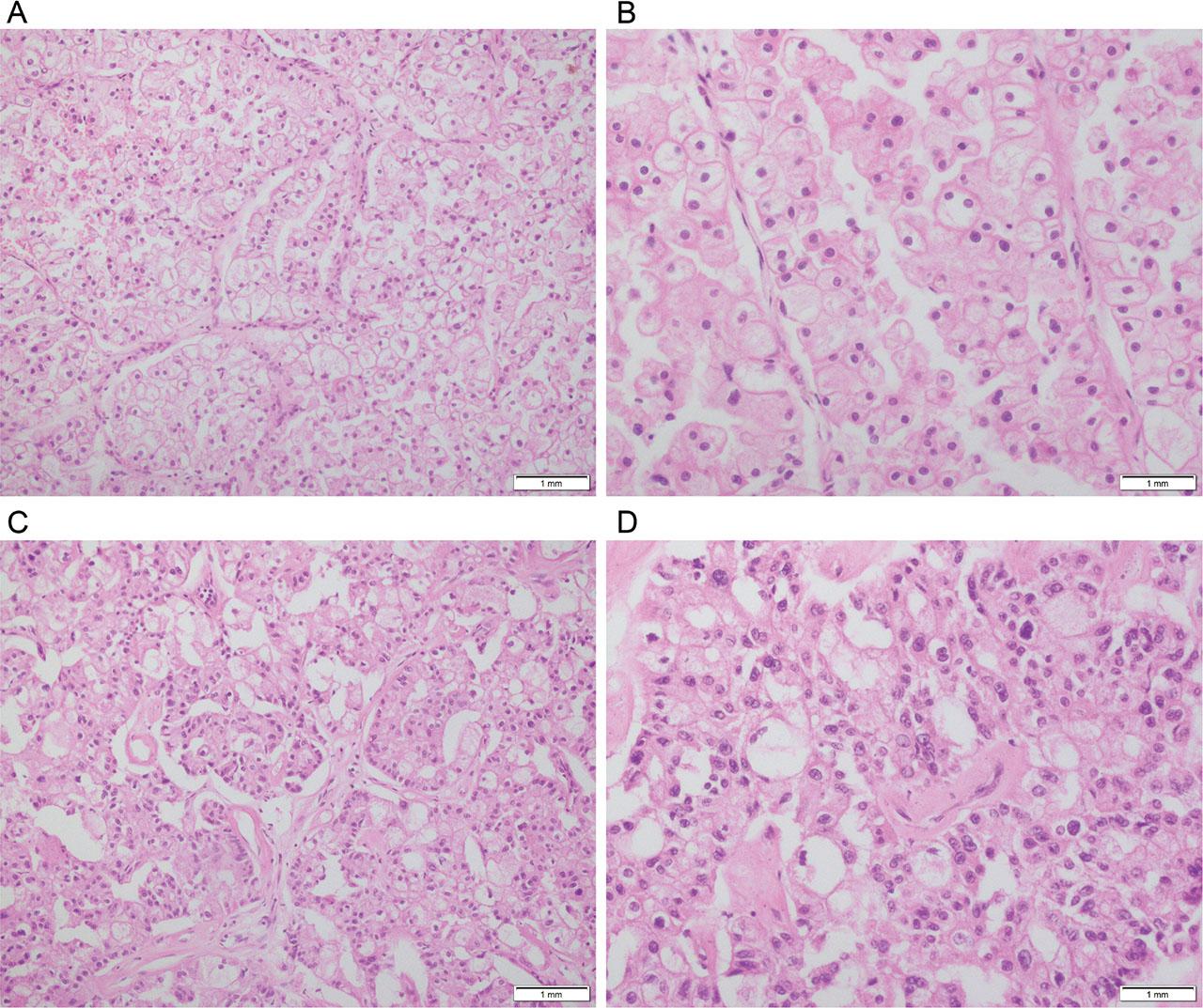
Chromophobe tumor grades. A, Chromophobe tumor grade 1 (H&E 20X). B, Chromophobe tumor grade 1 (H&E 40X). C, Chromophobe tumor grade 2 (H&E 20X). D, Chromophobe tumor grade 2 (H&E 40X). E, Chromophobe tumor grade 3 (H&E 20X). F, Chromophobe tumor grade 3 (H&E 40X).
The independent prognostic factors pT stage, tumor necrosis, and sarcomatoid change were also assessed. pT staging was assigned according to the AJCC 8th edition of 2017 TNM stage groupings. Sarcomatoid differentiation was defined as the presence of spindle-shaped, sarcoma-like cells showing high cellularity and atypia in at least one high-power field (Figure 2a). Coagulative tumor necrosis appeared as clusters and sheets of dead and degenerating tumor cells, ghost cells, and apoptotic debris merging into an amorphous coagulum (Figure 2b). Necrosis was quantified as a percentage of the total tumor area within histologic sections. The extent of necrosis was grouped as follows: group 1 (no necrosis), group 2 (1%–10% necrosis), and group 3 (more than 10% necrosis) [16]. Hyalinization, fibrosis, cholesterol clefts, edema, and infarction were excluded from the tumor-associated necrosis category.
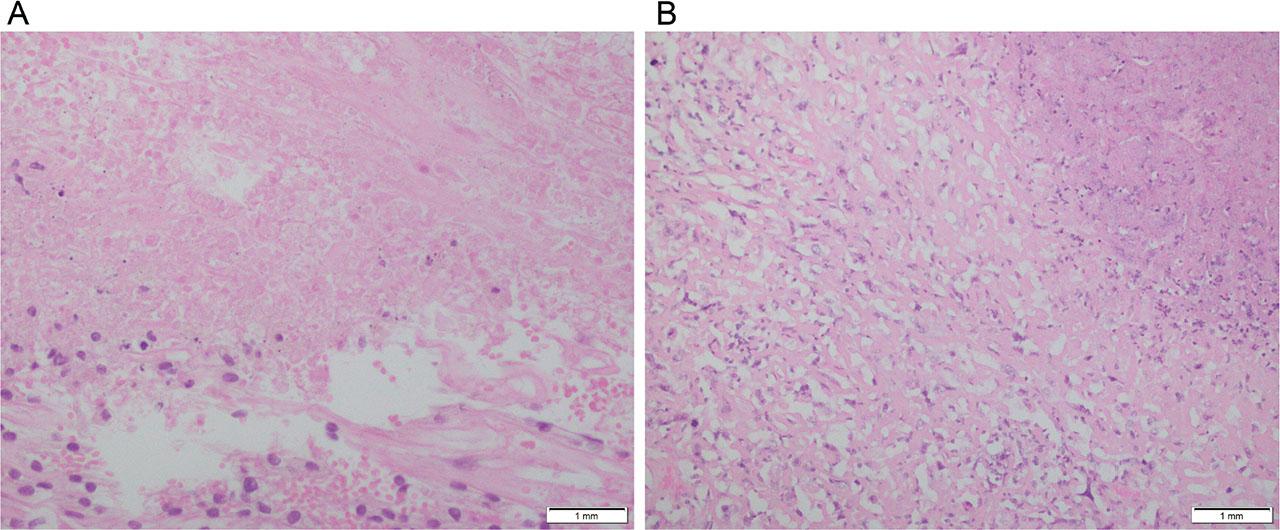
A, Sarcomatoid differentiation with area of necrosis (H&E 40X). B, Necrosis (H&E 40X).
Statistical analysis used Chi-square tests and independent sample t-tests. All tests were 2-sided. P values < 0.05 were considered statistically significant. Survival analysis was performed using the Kaplan-Meier method. The outcome was defined as the time from surgery to the first occurrence of local recurrence, metastasis, or disease-related death. Patients lost to follow-up or who died from unrelated causes were considered censored. Overall survival was calculated from the date of radical nephrectomy to the most recent follow-up. Distant metastasis-free survival (DMFS) was the time from surgery to the first occurrence of distant metastasis. Recurrence-free survival (RFS) was the time from surgery to the first occurrence of local recurrence. Cancer-specific survival (CSS) was the time from surgery to cancer-related death. A significant event was any recurrence (local or distant) or cancer-related death.
Clinical and pathological characteristics for all 51 patients with chromophobe RCC have been summarized in Table 1.
Summary of Clinical and Pathological Features for 51 Patients with Chromophobe RCC.
| Feature | Sub-category | Mean (Median; Range) |
|---|---|---|
| Age at surgery (years) | 46 (47; 25–70) | |
| Maximum tumor size (cm) | 9.6 (8.5; 4–17.5) | |
| Gender | Female | 31 (60.8%) |
| N (%) | Male | 20 (39.2%) |
| 2017 Primary tumor classification N (%) | pT1a | 2 (2%) |
| pT1b | 16 (31%) | |
| pT2a | 10 (19%) | |
| pT2b | 12 (23%) | |
| pT3a | 11 (21%) | |
| pT3b | 0 | |
| pT3c | 0 | |
| pT4 | 0 | |
| 2017 regional lymph node involvement N (%) | pNX and pN0 | 51 (100%) |
| pN1 | 0 | |
| Distant Metastasis N (%) | pMX | 51 (100%) |
| pM1 | 0 | |
| 2017 TNM stage groupings N (%) | I | 18 (35%) |
| II | 22 (43%) | |
| III | 11 (21%) | |
| IV | 0 | |
| Sarcomatoid Differentiation N (%) | Yes | 2 (4%) |
| No | 49 (96%) | |
| Coagulative tumor necrosis N (%) | 0% | 43 (84%) |
| 1% to 10% | 6 (11%) | |
| >10% | 2 (4%) | |
| Chromophobe RCC grade N (%) | 1 | 4 (7.8%) |
| 2 | 31 (60.8%) | |
| 3 | 16 (31.4%) | |
| Fuhrman Nucleolar Grade N (%) | 1 | 26 (51%) |
| 2 | 20 (39.2%) | |
| 3 | 2 (3.9%) | |
| 4 | 3 (5.9%) | |
N (Number of cases); RCC (Renal Cell Carcinoma).
Patients’ ages ranged from 25 to 70 years (mean 46 years). Of the 51 patients, 31 (60.8%) were female and 20 (39.2%) were male. Chromophobe RCC tumors varied in size from 4 to 17.5 cm (mean 9.6 cm), and 50 out of 51 (98%) were larger than 4.0 cm. Tumors were generally well-circumscribed, with appearances ranging from light tan to mahogany brown and yellow. Their architectural patterns included nested, alveolar, solid, cystic, and tubular structures. Cytoplasm ranged from granular and eosinophilic to vacuolated, often showing perinuclear clearing, which created a “plant-cell appearance.” Nuclei ranged from round and uniform to irregular and hyperchromatic, with or without prominent nucleoli. Binucleation was common. Renal sinus fat invasion was observed in 10 cases (19.6%). All ureteric and vascular resection margins were free of tumor.
Follow-up data were available for all 51 patients, with a mean follow-up duration of 50 ±10 months, a median of 50 months, and a range of 13 to 101 months. During this follow-up period, a total of four patients experienced adverse events. One patient developed metastasis, experienced disease recurrence, and subsequently died. Another patient developed metastasis and succumbed to renal cell carcinoma (RCC). The remaining two patients developed metastases without further complications. In total, there were four cases of metastases, two deaths, and one recurrence.
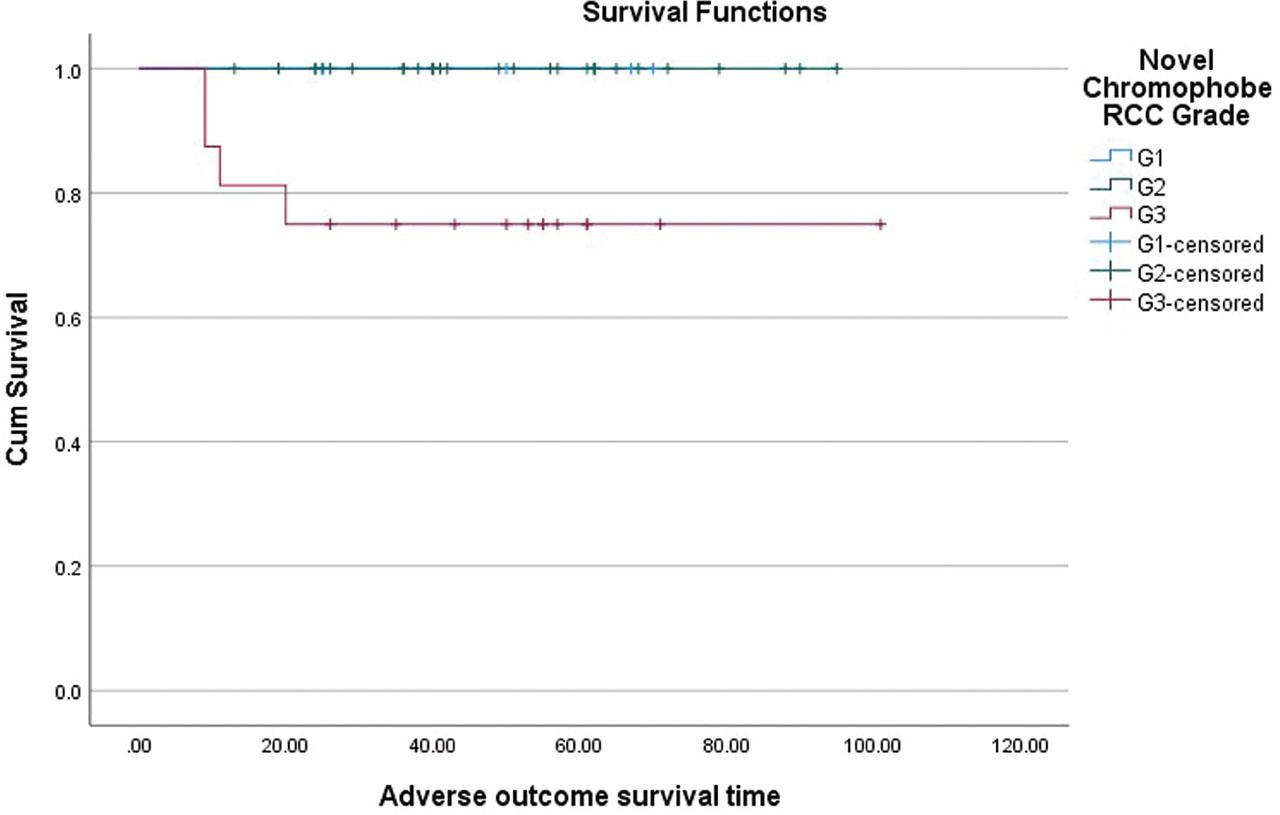
The distributions of chromophobe RCC based on Novel chromophobe tumor grade by Paner et al were as follows: (n = 51): grade 1, 4/51 (7.8%); grade 2, 31/51 (60.8%); and grade 3, 16/51 (31.4%). In grades 1 and 2 tumors, none experienced any significant events, including death, metastasis, or recurrence.
Consequently, the overall survival, distant-metastasis-free survival, and recurrence-free survival for grade 1 tumors were all 100%. In contrast, all of the adverse events (including four metastases, one recurrence, and two deaths) happened amongst the 16 patients with grade 3 tumors. The distant metastases free survival (DMFS), local recurrence free survival (RFS), and cancer-specific survival rate (CSS) for grade 3 tumors after a mean follow-up of 50.3 months were 75% (71–79%), 93.8% and 87.5% respectively. (Figure 3)
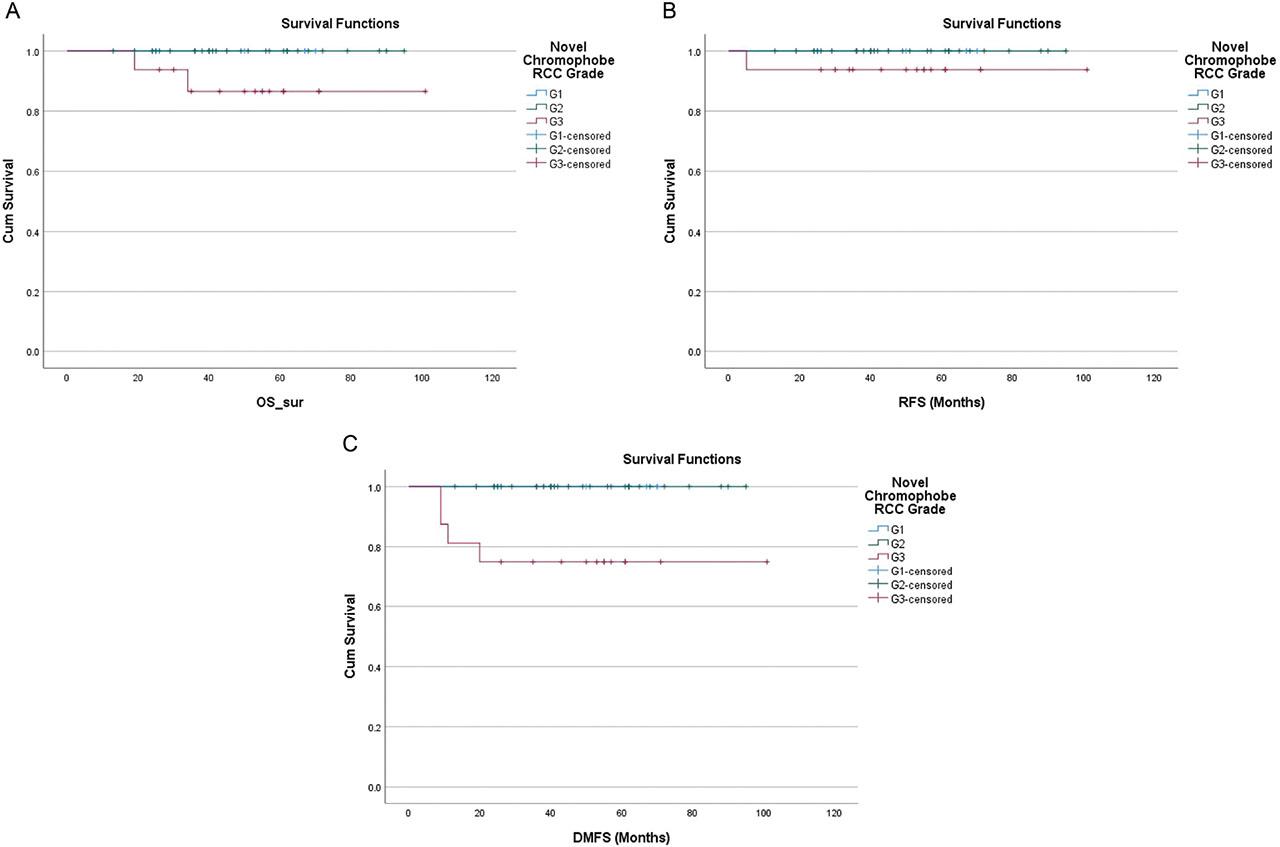
Chromophobe tumor grade. A, Overall survival (months). B, Recurrence-free survival (months). C, Distant metastasis-free survival (months).
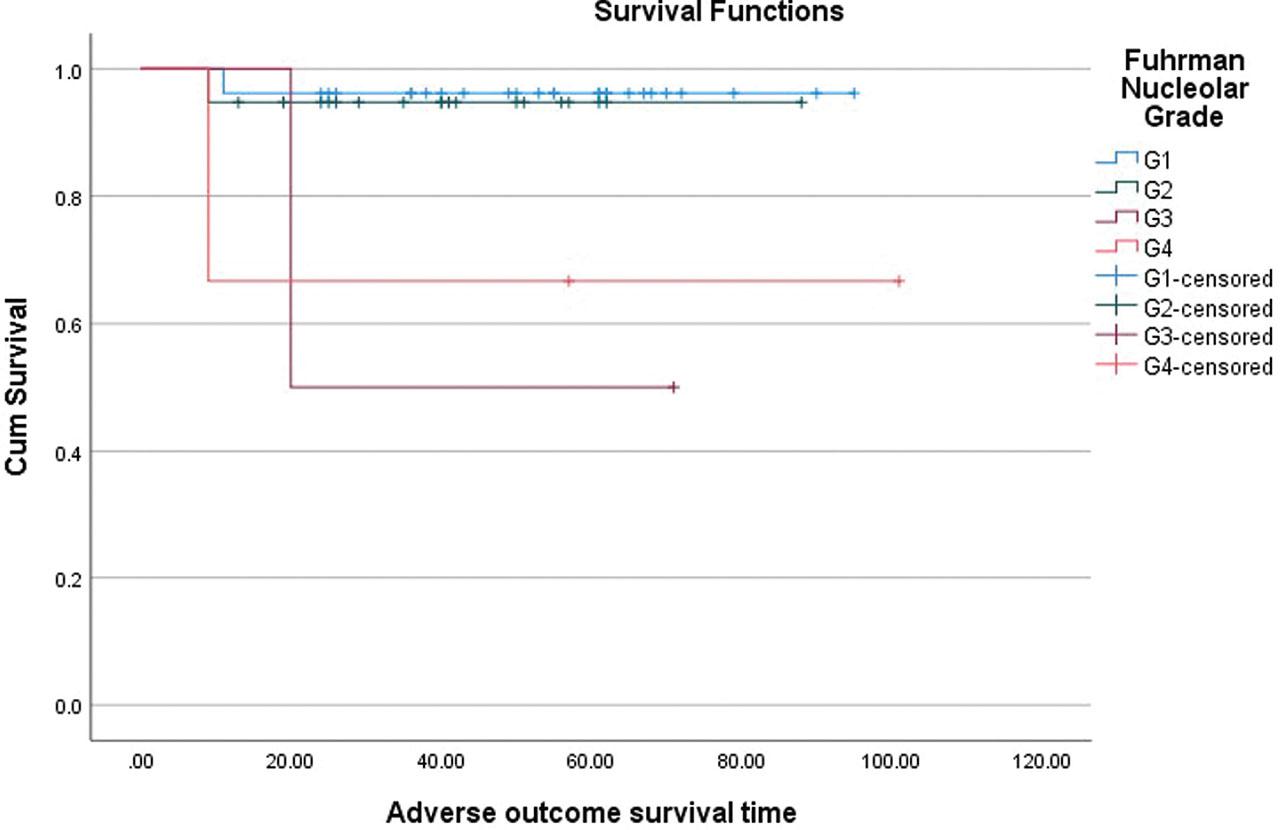
The distribution of chromophobe RCC by Fuhrman nucleolar grade was as follows: (n = 51): grade 1, 26/51 (51%); grade 2, 20/51 (39.2%); grade 3, 2/51 (3.9%), and grade 4, 3/51 (5.9%). Among the 26 patients with grade 1 tumors, one patient developed distant metastases, but no recurrences or deaths occurred. Thus, the distant-metastasis-free survival was 96.2%, while recurrence-free survival and overall survival were 100% in grade 1 tumors. Among the 20 patients with grade 2 tumors, one patient developed distant metastasis, experienced local recurrence, and succumbed to RCC. This resulted in a 95% cancer-specific survival rate, 95% local recurrence-free survival (RFS), and 95% distant metastasis-free survival for grade 2 tumors. For the two patients with grade 3 tumors, one developed distant metastasis, but no recurrences or deaths occurred, resulting in a 50% distant metastasis-free survival (DMFS), 100% local recurrence-free survival (RFS), and overall survival (OS). Among the three patients with grade 4 tumors, one developed distant metastasis and died of RCC, but there were no recurrences. The distant metastasis-free survival (DMFS) and cancer-specific survival were 66.7%, with a 100% local recurrence-free (RFS) survival rate. (Figure 4)
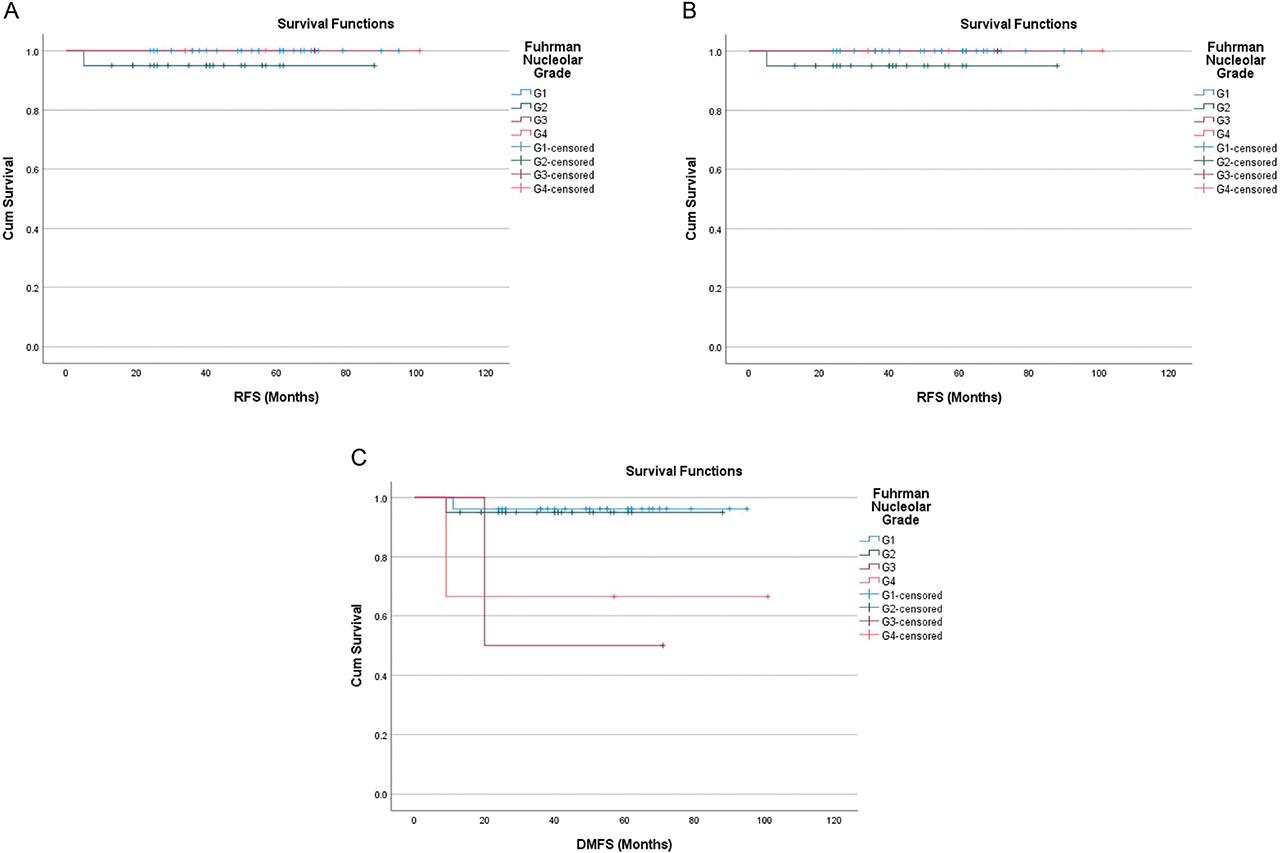
Fuhrman nucleolar grade. A, Overall survival (months). B, Recurrence-free survival (months). C, Distant metastasis-free survival (months).
Overall survival of adverse outcome with regard to Chromophobe tumor grade.
Overall survival in relation to adverse outcomes concerning Fuhrman nucleolar grade.
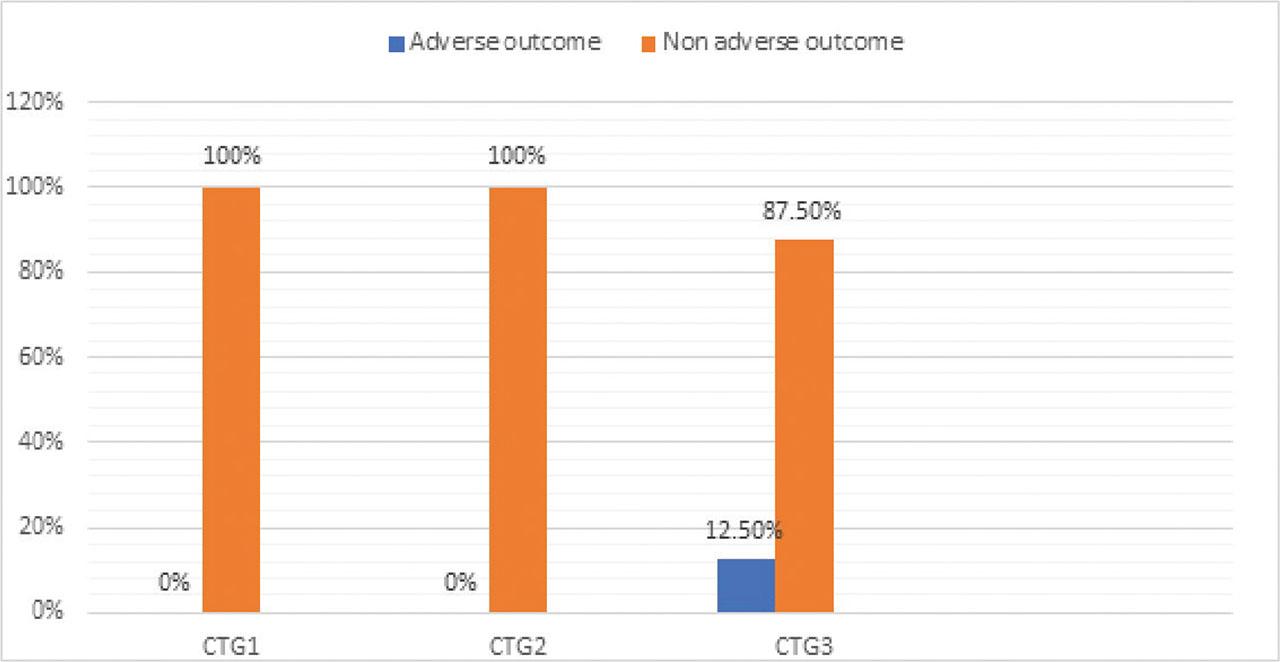
Association of the novel chromophobe tumor grade (CTG) with chromophobe renal cell carcinoma with adverse outcome (local recurrence, metastasis, and/or death owing to disease).
Correlation of Grading systems with established independent prognostic factors, i.e., coagulative tumor necrosis, sarcomatoid differentiation, TNM stage, and their effect on survival. The distribution of the TNM stage groupings (I, II, and III), presence or absence of sarcomatoid differentiation, and percentage of coagulative tumor necrosis in association with the three groups in Chromophobe tumor grading and with the four groups of Fuhrman nucleolar grade are listed in Tables 2 and 3, respectively.
Correlation of Chromophobe grading system with coagulative tumor necrosis, sarcomatoid differentiation and TNM stage.
| Novel ChRCC Grade | TNM stage groupings | Sarcomatoid Differentiation | Tumor necrosis (%age) | |||||
|---|---|---|---|---|---|---|---|---|
| N (%) | Stage I N (%) | Stage II N (%) | Stage III N (%) | Present N (%) | Absent N (%) | Group 1 (0%) | Group 2 (1%–10%) | Group 3 (>10%) |
| Grade 1 | 1 (25%) | 2 (50%) | 1 (25%) | 0 (0%) | 4 (100%) | 4 (100%) | 0 (0%) | 0 (0%) |
| Grade 2 | 11 (33%) | 15 (45%) | 5 (15%) | 0 (0%) | 31 (100%) | 27 (87%) | 2 (6%) | 2 (6%) |
| Grade 3 | 6 (37%) | 5 (31%) | 5 (31%) | 2 (12%) | 14 (88%) | 0 (0%) | 14 (87.5%) | 2 (12.5%) |
N (Number of cases)
Correlation of the Fuhrman nucleolar grading system with coagulative tumor necrosis, sarcomatoid differentiation and TNM stage.
| Fuhrman Nucleolar Grade | TNM stage groupings | Sarcomatoid Differentiation | Tumor necrosis (%age) | |||||
|---|---|---|---|---|---|---|---|---|
| N (%) | Stage I N (%) | Stage II N (%) | Stage III N (%) | Present N (%) | Absent N (%) | Group 1 (0%) | Group 2 (1%–10%) | Group 3 (>10%) |
| Grade 1 | 9 (34%) | 13 (50%) | 4 (15%) | 0 (0%) | 26 (100%) | 22 (77%) | 2 (8%) | 4 (15%) |
| Grade 2 | 7 (35%) | 8 (40%) | 5 (25%) | 0 (0%) | 20 (100%) | 17 (85%) | 0 (0%) | 3 (15%) |
| Grade 3 | 1 (50%) | 0 (0%) | 1 (50%) | 1 (50%) | 1 (50%) | 2 (100%) | 0 (0%) | 0 (0%) |
| Grade 4 | 1 (33%) | 1 (33%) | 1 (33%) | 1 (33%) | 2 (67%) | 2 (67%) | 0 (0%) | 1 (33%) |
N (Number of cases).
Among the four tumors that developed significant events due to ChRCC, one belonged to stage group I, while three were in stage and 2) but present in grade 3 tumors. However, TNM stage grouping did not demonstrate a specific association within our cohort.
Comparison of independent prognostic factors with Fuhrman nucleolar grade did not reveal any specific associations, except for the presence of sarcomatoid differentiation in higher grades. TNM stage groupings and tumor necrosis exhibited variability and lacked a consistent pattern.
Chromophobe renal cell carcinoma (ChRCC) is generally associated with an excellent prognosis, with only a small subset of cases exhibiting aggressive behavior [3,10,15]. In our study, only 4 out of 51 patients experienced adverse events, reinforcing the notion that ChRCC typically follows an indolent course.
Our findings suggest that the novel three-tiered ChRCC grading system proposed by Paner et al., which incorporates geographical crowding, nuclear size, anaplasia, and sarcomatoid differentiation, effectively stratifies tumors with an increased risk of progression following surgical intervention. The majority of ChRCC cases were categorized as low grade (chromophobe tumor grades 1 and 2), with a decreasing frequency as tumor grade increased—an inverse relationship that aligns with the generally favorable biologic behavior of this tumor type. Furthermore, we observed a consistent trend linking higher chromophobe tumor grades to an increased proportion of adverse outcomes, further supporting the prognostic utility of this grading system.
Various histological parameters have previously been explored as components of a potential ChRCC grading system [1,3,10]. The Fuhrman grading system, which primarily relies on the presence of prominent nucleoli, has limited applicability to ChRCC due to the inherent rarity of prominent nucleoli in this subtype [3,4,11,12]. In contrast, nuclear pleomorphism is a defining feature of ChRCC. To date, no study has demonstrated the prognostic utility of Fuhrman nuclear grading in ChRCC, and some experts discourage its use in this context. Delahunt et al. recently investigated the prognostic value of Fuhrman nuclear grade in a cohort of 87 ChRCC cases and found no significant association between any of the grading components—including whole tumor or focal nucleolar grade, nuclear shape, and nuclear size—and survival outcomes [3,13]. Additionally, their study revealed that the trend between Fuhrman nuclear grade and adverse outcomes was inconsistent across different levels, and Fuhrman nuclear grade was not an independent predictor of prognosis in ChRCC. Our findings further corroborate these observations, providing additional objective data that highlight the limited clinical utility of Fuhrman nuclear grading for this tumor type. Similarly, Lohse et al. reported significant overlap among Fuhrman grades 1, 2, and 3 in ChRCC, suggesting that nuclear features alone may be insufficient to accurately stratify non-grade 4 ChRCC cases [3,14]. This limitation likely stems from the intrinsic nuclear atypia observed even in lower-grade ChRCC tumors. Finley et al. also conducted a study comparing the Fuhrman nuclear grading system with the chromophobe RCC grading system in 84 cases of chromophobe renal cell carcinoma, utilizing ROC curve analysis and area under the curve (AUC) values [17]. Among the patients, 20 (24%) experienced or later developed metastatic disease, while 11 (13%) exhibited sarcomatoid differentiation.
The ROC analysis revealed that the chromophobe RCC grade achieved a marginally higher AUC for recurrence-free survival compared to the Fuhrman grade (0.822 vs. 0.807). Based on these findings, the authors concluded that the chromophobe RCC grading system is the more suitable grading approach for this tumor type. Similarly, in a recent study by Sali et al., 80 cases of chromophobe renal cell carcinoma (ChRCC) were analyzed to compare the prognostic value of the Fuhrman nuclear grade (FNG) and the chromophobe tumor grade (CTG) [18]. Both grading systems correlated with disease-free survival (DFS); however, only CTG maintained statistical significance in non-sarcomatous cases (P < 0.001). ROC curve analysis further showed that CTG had higher predictive accuracy for DFS, while FNG lost significance in the non-sarcomatous subset. Moreover, CTG (P = 0.001), but not FNG, was associated with disease-specific adverse events. These findings support the use of CTG as a more reliable and clinically relevant grading system for ChRCC, consistent with our observations.
The presence of sarcomatoid differentiation has been well established as an indicator of poor prognosis across various renal cancer subtypes [1,3,10]. The Paner grading system assigns grade 3 to ChRCC tumors with frank anaplasia and/or sarcomatoid transformation [3]. However, most adverse events in their study were observed in grade 3 tumors with sarcomatoid differentiation, leading the authors to exclude this subset from certain analyses due to its overriding impact on prognosis [3]. In contrast, our data revealed that only one of the four patients who experienced adverse events exhibited sarcomatoid differentiation, while all four cases belonged to chromophobe grade 3. This finding underscores the strong association between chromophobe nuclear grade and adverse outcomes, independent of sarcomatoid differentiation.
For the predominant non-sarcomatoid cohort, Paner et al. reported a statistically significant correlation between chromophobe tumor grade and both pT stage and adverse outcomes [3]. Our findings support this observation, as 3/4 cases with significant events in our study were classified as pT stage 3; however, we could not establish a prognostic relevance between chromophobe grading and pT stage.
Additionally, our data highlight the prognostic significance of tumor necrosis in ChRCC. All patients who experienced significant events in our cohort exhibited tumor necrosis, supporting its potential role as a key parameter in a refined ChRCC grading system. These findings align with those of Cheville et al., who identified necrosis as a prognostic factor for ChRCC in a univariate analysis in addition to the grading system proposed by Paner et al [2,10]. In support of the prognostic utility of the Paner grading system, Avulova et al. conducted a comprehensive study involving 266 patients with nonmetastatic chromophobe renal cell carcinoma (ChRCC) who underwent nephrectomy [1]. Their analysis validated the Paner grading system and further emphasized the prognostic significance of incorporating tumor necrosis. The authors observed that while the original Paner system showed a significant association with cancer-specific survival (CSS), the presence of necrosis within grade 2 tumors identified a subset of patients with worse outcomes. Based on these findings, they proposed a modified four-tier grading system that separates grade 2 tumors into those with and without necrosis, demonstrating progressively higher hazard ratios for CSS across grades 2, 3, and 4. These results suggest that while the Paner system remains a robust and practical grading approach for ChRCC, its prognostic accuracy could be further enhanced by the inclusion of tumor necrosis as an additional parameter. However, it is crucial to differentiate tumor-related necrosis from thromboembolic coagulative necrosis, which is typically macroscopic and extensive. Tumor-related necrosis is characterized by aggregates of nuclear debris and has been widely recognized as an unfavorable prognostic indicator in clear cell RCC [10]. Our findings suggest that its prognostic relevance extends to ChRCC as well.
In summary, multiple studies—including those by Avulova et al. [1], Cheville et al. [2], Finley et al. [17], Sali et al. [18], and Schieda et al. [19]—have consistently supported the prognostic relevance and practical utility of the Paner grading system and its modified versions for chromophobe renal cell carcinoma (ChRCC). These findings, in agreement with our observations, suggest that the Paner system provides a more accurate and reproducible method for grading ChRCC compared to earlier schemes. However, despite this growing evidence, the system has not yet been fully validated across larger, multi-institutional cohorts. Given the relatively indolent nature of ChRCC and the low frequency of adverse clinical events, large-scale studies with extended follow-up are needed to establish its definitive prognostic value.
Our findings further support the notion that Paner et al.’s chromophobe tumor grading system enhances prognostic reliability over the traditional Fuhrman nucleolar grading in ChRCC. Specifically, grade 3 tumors demonstrated more aggressive behavior, reinforcing the clinical relevance of this system in identifying patients at potential risk for disease progression. Incorporating the Paner system into routine practice poses no risk and may, in fact, improve the accuracy of clinical decision-making.
Nonetheless, a key limitation of our study is the relatively small cohort size. Because ChRCC generally carries a favorable prognosis, the number of significant adverse events was even smaller, potentially leading to false-positive p-values. As a result, our study demonstrates primarily clinical rather than statistical significance. Future studies with larger, multi-institutional cohorts and extended follow-up are therefore necessary to validate these findings and further refine prognostic models for ChRCC.