
In 2020, 19.3 million new cases of cancer were diagnosed globally, with colorectal cancer (CRC) contributing to 1.93 million cases and 935,000 deaths. Approximately 20% of CRC patients present with metastatic disease, while 25% of initially localized cases progress to develop metastases (1). The relative 5-year survival rate for metastatic CRC (mCRC) is only 14%, compared to 71% and 90% for regional and localized disease, respectively (2).
While high-income countries have seen improvements in mCRC survival due to advances in systemic chemotherapy, targeted therapies, and surgical resection of metastases, the extent to which these approaches are utilized in low- and middle-income countries (LMICs) remains unclear. The burden of CRC remains significant, particularly in low- and middle-income countries (LMICs) where access to timely diagnosis and comprehensive care is limited (3). Common sites of metastasis include the liver and lungs, and patient outcomes are influenced by tumor biology, treatment modalities, and patient factors such as baseline performance status (4).
In Pakistan, CRC ranks as the fourth most commonly occurring cancer, with an estimated incidence of 9447 cases (5.1%) and a mortality of 5,235 (4.4%) in 2022 (5). However, the true burden is likely underestimated due to the absence of reliable cancer datasets and a national cancer registry (6). The lack of organized screening programs, geographic disparities in healthcare infrastructure, and socioeconomic barriers further contribute to late-stage presentation and suboptimal outcomes in the country (7). Access to healthcare is particularly limited in rural areas, where there is a shortage of specialists, diagnostic tools, and treatment facilities, which exacerbates the challenges in early detection and the appropriate management of CRC (8). Urban-rural disparities in access to timely and quality care significantly influence survival outcomes, with patients in rural areas often presenting at more advanced stages of the disease.
This study aims to provide an overview of clinical characteristics, treatment patterns, and outcomes of patients diagnosed with mCRC at Aga Khan University Hospital (AKUH). Given the limited data on how CRC presents and progresses in Pakistan, this research aims to provide a foundational understanding of the disease in the local context.
This retrospective study reviewed patients diagnosed with metastatic colorectal cancer (mCRC) at Aga Khan University Hospital (AKUH), Karachi, Pakistan. Patients were identified using the International Classification of Diseases, 10th Revision (ICD-10) codes C18–C20 from the Health Management Information System (HMIS) at AKUH. The study included patients diagnosed with colorectal carcinoma between January 2020 and December 2022. The study has been reported in accordance with STrengthening the Reporting of OBservational studies in Epidemiology checklist for cohort studies (Supplement Table 1). All patients with evidence of distant metastases during the study period were eligible, regardless of the timing of metastatic presentation.
The initial list of patients with colorectal carcinoma was screened by two investigators (F.A. and M.I.) to identify patients presenting with metastatic disease (stage IV CRC) or who developed metastases during follow-up within the study period. Metastatic disease was identified based on documented evidence from imaging (CT scans), or clinical records indicating the presence of metastases. The follow-up period was defined as the time from initial presentation at our institution to the last documented visit within the study period or the date of death, whichever came first. Patients with no evidence of metastasis at any point during the study period were excluded. All patients meeting the inclusion criteria were included in the study using consecutive sampling.
Relevant data were extracted through comprehensive chart reviews using the hospital's electronic medical records. The following information was collected: demographics (age, gender, comorbidities), tumor characteristics (stage, grade, histology, lymph node involvement, lymphovascular invasion, and sites of metastasis), clinical history (comorbid conditions, medical and surgical history), treatment details (neoadjuvant therapy, surgical interventions, adjuvant therapy) and outcomes (postoperative complications, readmissions). Missing data were reported as missing without imputation.
This study received an exemption from the Ethical Review Committee at Aga Khan University (2023-8917-25434). Informed consent was obtained from all participants prior to their inclusion in the study.
Descriptive statistics were used to summarize the data, with continuous variables reported as means with standard deviations (SD) or medians with interquartile ranges (IQR), and categorical variables summarized as frequencies and percentages. Kaplan-Meier curves were used to assess survival from the time of metastasis to death. All analyses were conducted using SPSS (version 26).
Follow-up time was calculated as the time from CRC diagnosis to death or the last follow-up visit. Time from metastasis to death was calculated as the time from the first discovery of metastasis to death.
A total of 141 patients diagnosed with metastatic colorectal carcinoma (mCRC) from 1st January 2020 to 31st December 2022 were included in the study. Of these, 40 patients (28.4%) presented with metastatic disease at the time of diagnosis, while 101 patients (71.6%) initially presented with localized colorectal cancer (CRC) that later progressed to metastatic disease (Table 1).
Demographic and Clinical Characteristics of Patients with Metastatic Colorectal Cancer.
| Demographic Characteristics | Frequency (n) | Percentage (%) |
|---|---|---|
| Age (mean and STD) | 51 | 17.4 |
| Age at the time of diagnosis | ||
| ≤30 years | 14 | 9.9 |
| 31–40 years | 23 | 16.3 |
| 41–50 years | 25 | 17.7 |
| 51–60 years | 23 | 16.3 |
| 61–70 years | 33 | 23.4 |
| 71–80 years | 8 | 5.7 |
| 81–90 years | 6 | 4.3 |
| >90 years | 1 | 5.7 |
| Missing | 8 | 1.2 |
| Gender | ||
| Male | 80 | 56.7 |
| Female | 61 | 43.3 |
| Province of origin | ||
| Sindh | 101 | 71.1 |
| Punjab | 6 | 4.2 |
| Balochistan | 5 | 3.5 |
| Gilgit/Baltistan | 2 | 1.4 |
| Outside Pakistan | 12 | 8.5 |
| Missing | 15 | 10.6 |
| Clinical Characteristics | Frequency (n) | Percentage (%) |
| BMI (mean and STD) | 25 | 5.6 |
| BMI | ||
| Underweight | 16 | 11.3 |
| Normal | 30 | 21.3 |
| Overweight | 15 | 10.6 |
| Obese | 51 | 36.2 |
| Missing | 29 | 20.6 |
| Smoking | 24 | 17 |
| Hypertension | 49 | 34.8 |
| Diabetes Mellitus | 40 | 28.4 |
| Cardiovascular Disease | 16 | 11.3 |
| Cerebrovascular Disease | 0 | 0 |
| Chronic Kidney Disease | 7 | 5 |
| Hyperlipidaemia | 4 | 2.8 |
| Thyroid Disease | 6 | 4.3 |
| Pulmonary Disease | 8 | 5.7 |
| Weight Loss (>=5%) in last 6 months | 86 | 61 |
| Positive Family History of CRC/FAP/HNPCC | 24 | 17 |
| Personal History of Cancer excluding CRC | 5 | 3.5 |
| Charlson Comorbidity Index | ||
| ≤8 | 94 | 66.7 |
| 9–10 | 19 | 13.5 |
| ≥11 | 12 | 8.5 |
| ECOG Classification | ||
| 0 | 7 | 5 |
| 1 | 44 | 31.2 |
| 2 | 12 | 8.5 |
| 3 | 7 | 5.0 |
| 4 | 7 | 5.0 |
| Missing | 49 | 34.9 |
| Demographic Characteristics | Frequency (n) | Percentage (%) |
| Bowel Obstruction | ||
| Yes | 50 | 35.2 |
| No | 79 | 55.6 |
| Missing | 12 | 8.6 |
| Bowel Perforation | ||
| Yes | 9 | 6.3 |
| No | 116 | 81.7 |
| Missing | 16 | 11.4 |
The mean age of the patients was 51 years (SD ± 17.4), with 23.4% aged 61–70 years, the most represented age group (Figure 1). Of the included patients, 80 (56.7%) were male. The study included patients from all over Pakistan, with the majority residing in Sindh (71.1%) followed by smaller proportions from Punjab (4.2%), Balochistan (3.5%), and Gilgit-Baltistan (1.4%). Additionally, 8.5% of patients were from outside Pakistan.
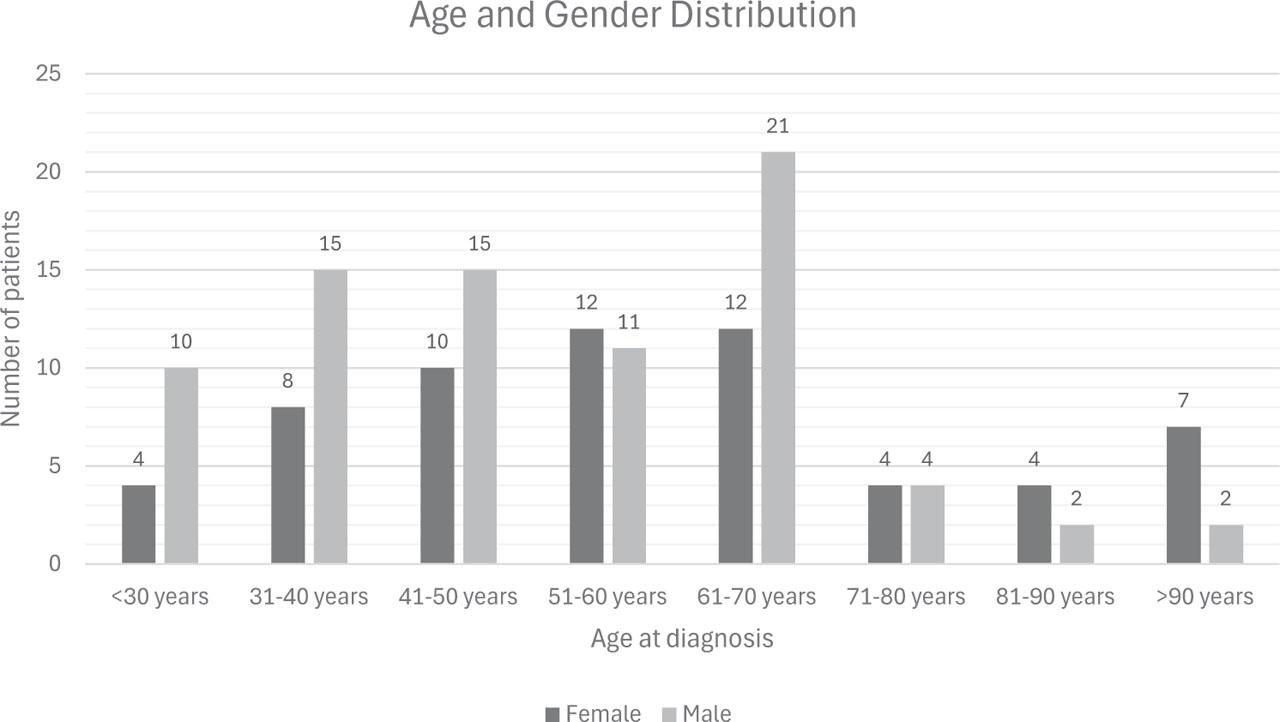
Age and gender distribution of metastatic colorectal cancer (mCRC) patients.
The mean BMI of the cohort was 25+ 5.6 kg/m2. Common comorbidities included hypertension (34.8%), diabetes mellitus (28.4%), and smoking (17%). The Charlson Comorbidity Index (CCI) distribution showed that 66.7% of patients had a CCI <8, 13.5% had a CCI between 9–10, and 8.5% had a CCI >11, indicating varying levels of comorbidity severity within the cohort. Weight loss ≥5% in the past six months was reported in 61%, and 17% had a family history of Colorectal Carcinoma, Familial Adenomatous Polyposis, or Hereditary Non-Polyposis Colorectal Cancer (Lynch Syndrome).
The most common tumor location was the rectum (27.5%), followed by the sigmoid colon (20.4%) and rectosigmoid junction (16.9%). Multisite colorectal cancer involvement was noted in 5.6% of patients. Adenocarcinoma was the predominant histological type (90.1%).
Liver-only metastases were the most common, observed in 39 patients (27.5%), followed by peritoneum-only (14.1%) and lung-only (4.9%). Multisite metastases (≥2 organs) were reported in 68 patients (48.2%). When accounting for all metastatic sites, the liver was involved in 49.6% of patients, followed by the peritoneum (35.5%) and lungs (15.6%) (Table 2).
Tumor and Metastatic Characteristics of Patients with Metastatic Colorectal Cancer.
| Tumor Characteristics | Frequency (n) | Percentage (%) |
|---|---|---|
| Tumour Location | ||
| Ascending Colon | 10 | 7.0 |
| Descending Colon | 6 | 4.2 |
| Transverse Colon | 10 | 7.0 |
| Sigmoid Colon | 29 | 20.4 |
| Rectosigmoid junction | 24 | 16.9 |
| Rectum | 39 | 27.5 |
| Others | 11 | 7.7 |
| Multisite CRC Involvement | 8 | 5.6 |
| Missing | 4 | 2.8 |
| Histological Type | ||
| Adenocarcinoma | 128 | 90.1 |
| Lymphoma | 2 | 1.4 |
| Squamous Cell Carcinoma | 2 | 1.4 |
| Others | 4 | 2.8 |
| Missing | 5 | 3.5 |
| Subtype Classification (based on histopathologic features) | ||
| Glandular | 4 | 2.8 |
| Mucinous | 21 | 14.8 |
| Signet Ring | 23 | 16.2 |
| Mixed | 11 | 7.7 |
| Not Reported/Missing | 82 | 57.8 |
| Level of Differentiation | ||
| Well-differentiated | 19 | 13.4 |
| Moderately differentiated | 58 | 45.1 |
| Poorly differentiated | 41 | 40.8 |
| Undifferentiated | 1 | 0.7 |
| Unknown/Missing | 22 | 15.3 |
| Pathological T stage | ||
| T1 | 0 | 0 |
| T2 | 4 | 2.8 |
| T3 | 40 | 28.2 |
| T4a | 22 | 15.5 |
| T4b | 6 | 4.2 |
| Not reported/Missing | 69 | 48.7 |
| Pathological N stage | ||
| N0 | 10 | 7 |
| N1 | 23 | 16.2 |
| N2 | 35 | 24.6 |
| NX | 65 | 45.8 |
| Not reported/Missing | 8 | 5.7 |
| Stage at Presentation | ||
| I–III | 101 | 71.6 |
| IV | 40 | 28.4 |
| Location of Metastasis | ||
| Liver-only | 39 | 27.5 |
| Lung-only | 7 | 4.9 |
| Peritoneum-only | 20 | 14.1 |
| Bone-only | 3 | 2.1 |
| Multisite (≥2 organs) | 68 | 48.2 |
| Other – single site metastasis | 4 | 3.2 |
| Total Involvement Across All Metastatic Sites** | ||
| Liver | 70 | 49.6 |
| Lung | 22 | 15.6 |
| Bone | 16 | 11.3 |
| Brain/Spinal cord | 1 | 0.7 |
| Peritoneum | 50 | 35.5 |
| Lymphovascular Invasion | ||
| No | 36 | 25.4 |
| Yes | 58 | 40.8 |
| Missing | 43 | 30.3 |
The total frequency exceeds the number of patients (141) due to overlapping sites in multisite metastases. Percentages are calculated out of the total number of patients.
Chemotherapy was administered to 106 (74.6%), with 52.8% receiving preoperative chemotherapy, 10.4% both pre- and postoperative, and 6.6% postoperative only. FOLFOX was the most common regimen (38.3%), followed by CAPEOX (19.9%). Radiotherapy was performed in 31 patients (21.8%), primarily preoperatively (7.7%) (Table 3).
Treatment Modalities, Complications, and Outcomes in Metastatic Colorectal Cancer Patients.
| Treatment Details | Frequency (n) | Percentage (%) |
|---|---|---|
| Chemotherapy | ||
| Yes | 106 | 74.6 |
| No | 33 | 23.2 |
| Missing | 2 | 1.4 |
| Chemotherapy Timing | ||
| Both preoperative and postoperative | 11 | 10.4 |
| Preoperative only | 56 | 52.8 |
| Postoperative only | 7 | 6.6 |
| Chemotherapy without surgery | 31 | 29.2 |
| Missing | 36 | 25.5 |
| Chemotherapy Regimen* | ||
| CAPEOX | 28 | 19.9 |
| FOLFIRI | 4 | 2.8 |
| FOLFOX | 54 | 38.3 |
| Others | 26 | 18.4 |
| Radiotherapy | ||
| Yes | 31 | 21.8 |
| No | 104 | 73.2 |
| Missing | 6 | 4.3 |
| Radiotherapy Timing | ||
| Preoperative only | 11 | 7.7 |
| Postoperative only | 10 | 7.0 |
| Radiotherapy without surgery | 10 | 7.0 |
| Primary Tumor Resection | ||
| Yes | 69 | 43.7 |
| No | 72 | 56.3 |
| Type of Primary Tumor Resection | ||
| Abdominoperineal resection | 6 | 4.2 |
| High anterior resection | 8 | 5.6 |
| Left hemicolectomy. | 16 | 11.3 |
| Low anterior resection | 16 | 11.3 |
| Right hemicolectomy | 17 | 12.0 |
| Sigmoid colectomy | 6 | 4.2 |
| Surgery performed for metastatic Lesions | ||
| Liver resection | 11 | 7.8 |
| Lung resection | 1 | 0.7 |
| Others** | 3 | 2.1 |
Some patients received multitherapy treatment.
CAPEOX: Capecitabine + Oxaliplatin.
FOLFIRI: Folinic Acid (Leucovorin) + Fluorouracil (5-FU) + Irinotecan.
FOLFOX: Folinic Acid (Leucovorin) + Fluorouracil (5-FU) + Oxaliplatin.
These included: appendectomy, cholecystectomy, hysterectomy, and splenectomy in one patient; cytoreductive surgery with HIPEC (including total abdominal hysterectomy, bilateral salpingo-oophorectomy, omentectomy, peritonectomy, and appendectomy) in one patient; and partial omentectomy in one patient.
Primary tumor resection was performed in 69 patients (43.7%), with right hemicolectomy (12.0%) and low anterior resection (11.3%) being the most common procedures. Among these, preoperative obstruction occurred in 30 (43.5%) and perforation in 5 (7.3%) patients. Regarding metastases in this subgroup, 17 (24.6%) had liver-only, 4 (5.8%) lung-only, and 13 (18.8%) peritoneum-only metastases. Of the 39 patients with liver-only metastases, 11 (28.2%) underwent surgical resection of metastatic lesions, while none of the 20 patients with peritoneum-only metastases underwent surgery. Only 4.9% of patients received immunotherapy, while liver ablation and portal vein embolization (PVE) were performed in 0.7% and 2.8% of patients, respectively.
A significant proportion of patients received care at multiple hospitals, indicating fragmented care pathways. 21.4% of patients obtained at least one imaging study outside AKUH. Specifically, 12.8% and 2.1% of patients received chemotherapy and radiotherapy respectively, at an external facility. Additionally, 8.5% of patients had surgical interventions related to diagnosis outside AKUH.
The median follow-up time for all patients was 9.3 months (IQR: 3.7–19.4). The median time from diagnosis of metastasis to death was 4.9 months (IQR: 1.1–9.3). The Kaplan-Meier survival curve (Figure 2) illustrates the probability of survival from the time of metastasis diagnosis until death.
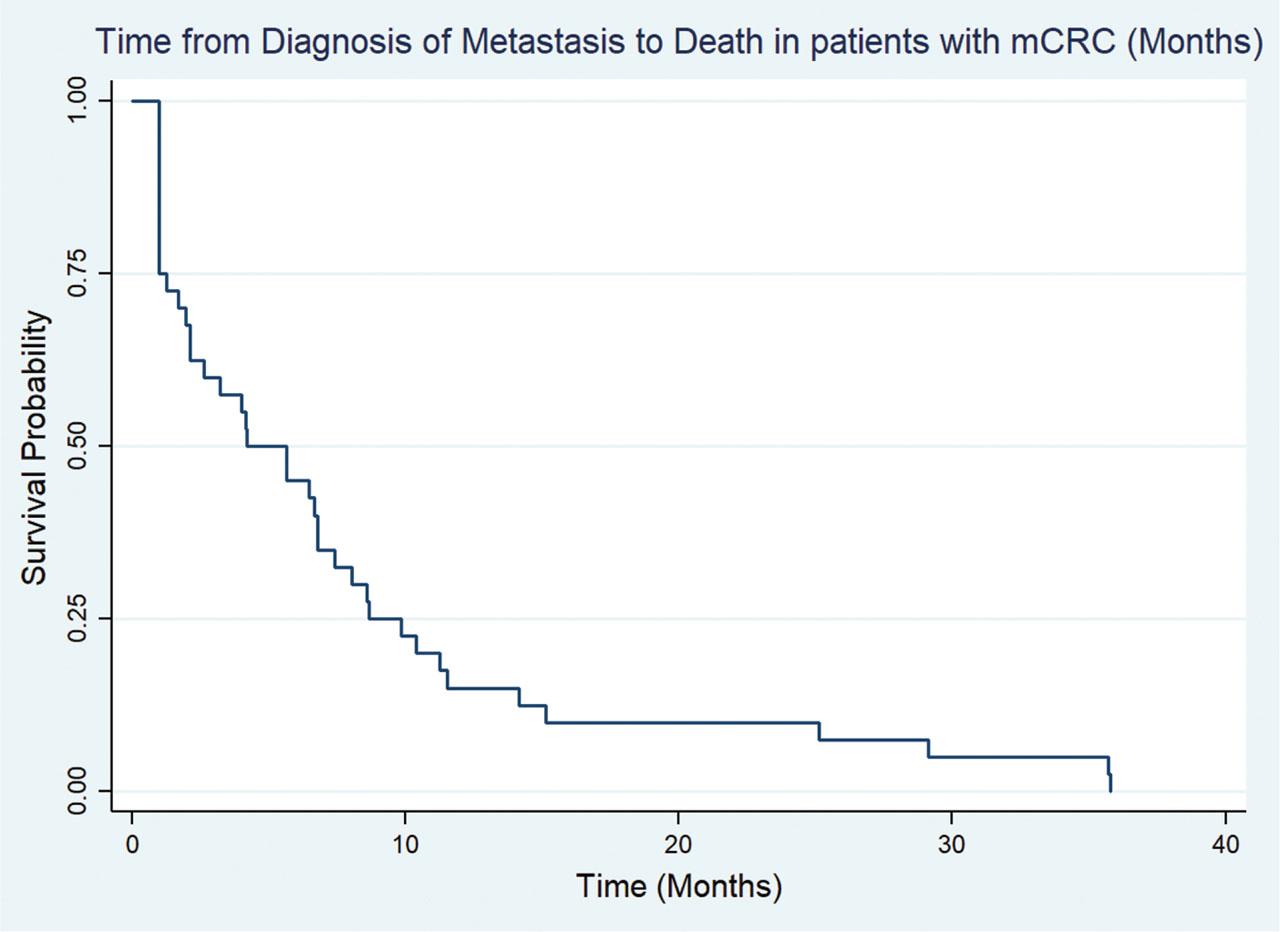
Kaplan-Meier survival curve showing survival from time of metastasis diagnosis to death in patients diagnosed with metastatic colorectal carcinoma (mCRC).
This study provides a comprehensive analysis of patients diagnosed with metastatic colorectal cancer (mCRC) at Aga Khan University Hospital (AKUH), presenting key demographic, clinical, and treatment-related characteristics within the context of a low- and middle-income country (LMIC). Among 141 patients, the cohort demonstrated a notably younger mean age at diagnosis (51 years) compared to high-income countries (HICs), alongside a high prevalence of multisite metastases (48.2%). This study is one of the first to characterize the presentation and treatment patterns for mCRC in Pakistan, highlighting the unique challenges of managing this disease in an LMIC. The absence of routine screening programs and limited public awareness regarding CRC further exacerbate delays in diagnosis and treatment (9), underscoring the importance of studying this population.
The mean age of diagnosis in our cohort was 51 years (SD ± 17.4), substantially younger than the reported averages in HICs, where CRC is typically diagnosed at a median age of 70 years in males and 72 years in females (10, 11). This aligns with growing evidence of earlier-onset CRC in LMICs, potentially driven by a combination of factors including genetic predisposition, limited access to screening, and dietary transitions associated with urbanization—such as increased consumption of processed and red meats and decreased fiber intake—though these patterns may vary across socioeconomic groups (12,13,14,15,16,17). In HICs, widespread screening programs, such as colonoscopy for individuals over 50, have substantially reduced CRC incidence and mortality (18,19,20). However, recent data from the United States indicate a shift toward earlier-onset CRC, with the proportion of cases in individuals younger than 55 years nearly doubling from 11% in 1995 to 20% in 2019 (21). These trends highlight the need for age-adjusted screening protocols globally. For LMICs like Pakistan, public health initiatives aimed at increasing awareness of CRC symptoms and promoting early diagnosis are critical to addressing the disease burden in younger populations.
A critical issue identified in this study is the limited access to advanced treatments for mCRC in Pakistan. In our cohort, 33 patients did not receive chemotherapy, possibly due to financial constraints, late-stage diagnoses, and gaps in healthcare. As shown in our Kaplan-Meier analysis (Figure 3), patients without chemotherapy had significantly lower survival, emphasizing the vital role of systemic therapy. Additionally, modern treatment modalities, such as immunotherapy, stereotactic body radiation therapy (SBRT), liver ablation, lung resections, and cytoreductive surgery with hyperthermic intraperitoneal chemotherapy [HIPEC], have shown promising results in improving survival in HICs (22,23,24,25), but were rarely utilized. Developing the infrastructure to support comprehensive cancer care, including equitable access to systemic and advanced treatments, is imperative to bridge this gap.
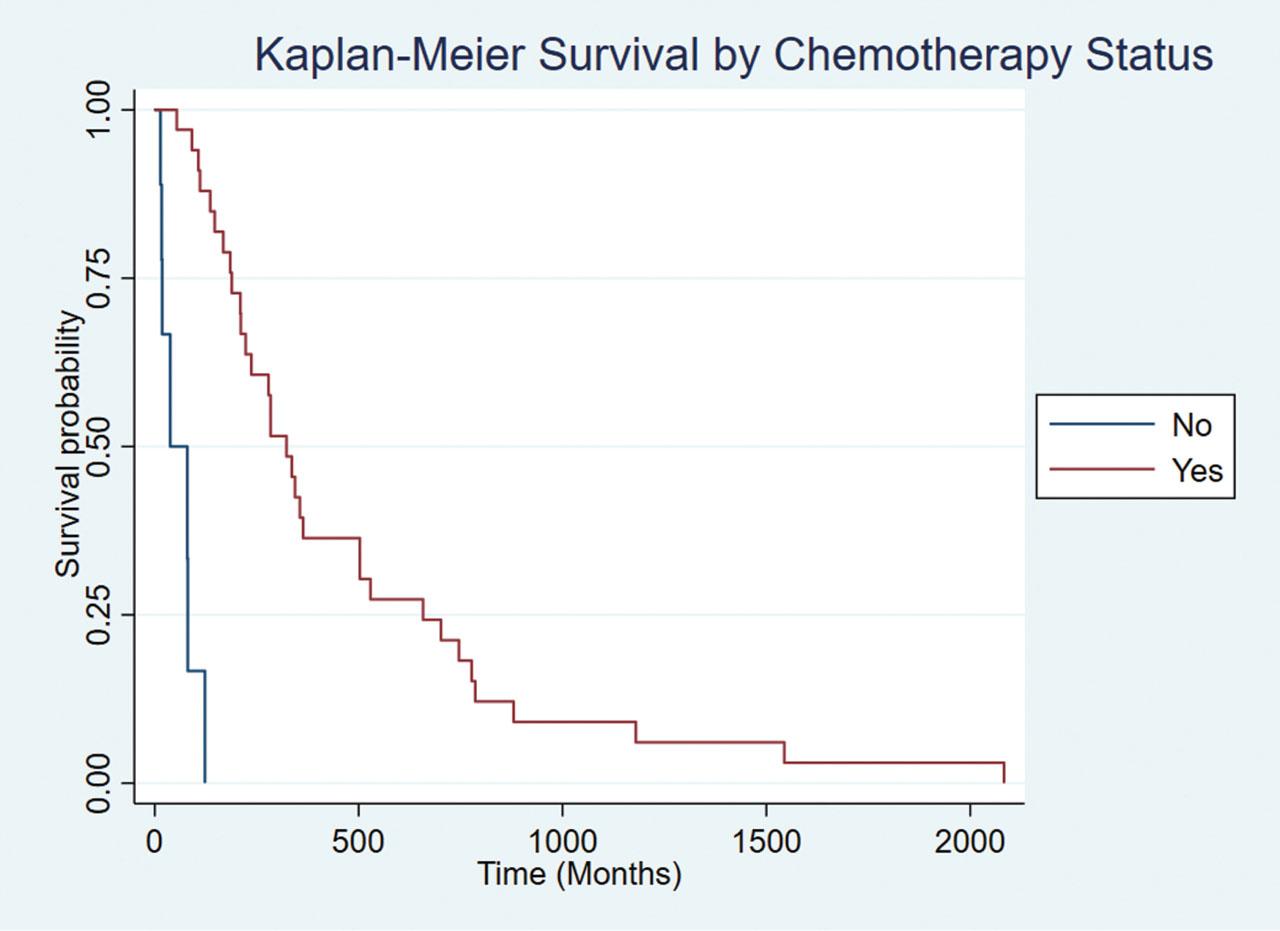
Kaplan-Meier survival curves comparing patients who received chemotherapy versus those who did not.
The surgical resection rate for patients with liver-only metastases was low, with only 28.2% undergoing surgery. Moreover, no patients with peritoneum-only metastases received surgical intervention. These findings suggest that potentially eligible patients were either not offered surgery or deemed unsuitable, potentially due to factors such as comorbidities, tumor burden, or lack of access to specialized surgical care. Delays in diagnosis and limited availability of advanced surgical techniques may have contributed to the low surgical intervention rates (26). Previous studies have demonstrated that surgical resection of liver-only metastases, particularly when combined with systemic therapy, can improve survival outcomes (27, 28). Similarly, selected patients with peritoneum-only metastases may benefit from cytoreductive surgery with HIPEC in specialized centers (29). The low rates observed in this study highlight a potential gap in care that warrants further investigation.
Fragmentation of care was another critical finding in this study, with a significant proportion of patients receiving treatment at multiple facilities, raising concerns about the continuity and coordination of treatment. Fragmented care pathways in LMICs often result from systemic barriers, such as geographical disparities, insufficient oncology centers, and socioeconomic challenges (30). Patients navigating multiple healthcare facilities often face delays in diagnosis, interruptions in treatment, and inconsistent quality of care (31). Efforts to streamline care delivery, improve inter-facility communication, and develop centralized oncology centers are crucial to addressing these challenges.
Approximately one-quarter of patients in our cohort did not receive chemotherapy. Although specific reasons for this were not systematically documented, financial and geographical constraints are likely a major barrier. Cancer treatment in Pakistan is prohibitively expensive for many patients, limiting their ability to afford systemic therapy (32). This finding is concerning, as timely treatment is crucial for improving survival outcomes in mCRC patients. Future studies should explore these barriers in greater detail to inform strategies to improve treatment adherence in resource-limited settings.
The rectum was the most common primary tumor site in our cohort (27.5%), followed by the sigmoid colon (20.4%) and rectosigmoid junction (16.9%). This contrasts with reports from HICs, where proximal colon tumors, often associated with high microsatellite instability and mismatch repair-deficient cancers, are more frequent (33). The predominance of rectal cancer in Pakistan may indicate a burden of germline mutations, particularly in the APC gene, warranting further genetic and molecular studies (34). Adenocarcinoma was the predominant histological subtype (90.1%), consistent with global trends. Liver metastases were the most frequently involved site, both as isolated metastases (27.5%) and across all cases (49.6%), aligning with international data reporting liver metastases in 25–30% of CRC patients (35). However, the high prevalence of multisite metastases (48.2%) and peritoneal metastases (35.5%) compared to lung metastases (15.6%) suggests an aggressive disease biology, potentially exacerbated by delayed diagnosis and treatment due to barriers in access to care.
The median follow-up time for all patients was 9.3 months (IQR: 3.7–19.4). The median time from diagnosis of metastasis to death was 4.9 months (IQR: 1.1–9.3). The Kaplan-Meier survival curve (Figure 2) illustrates the probability of survival from the time of metastasis diagnosis until death. These survival patterns are reflective of the advanced disease burden at presentation and highlight the need for earlier detection and more effective treatment options in Pakistan.
This study's single-center, retrospective design introduces inherent limitations, including selection and referral biases, which may affect the generalizability of the findings. Additionally, the inclusion of CRC patients who developed metastases during follow-up introduces heterogeneity that could influence comparisons of treatment outcomes and survival data. However, this approach allowed us to capture the broader spectrum of metastatic disease and provided valuable insights into the treatment and outcomes of CRC patients transitioning to stage IV disease. Missing clinical data, along with the absence of socioeconomic and treatment adherence information, further restricts our ability to assess barriers to care.
Future research should focus on identifying barriers to treatment, particularly among patients who do not receive chemotherapy or advanced therapies. Understanding whether treatment omissions stem from financial constraints, lack of access, or other social and logistical challenges is critical for improving care delivery in LMICs. Efforts to implement age-adjusted screening protocols and improve access to modern treatments, such as immunotherapy, liver resection, and SBRT, are essential. Additionally, molecular and genetic studies are needed to explore the unique epidemiological and molecular features of CRC in younger patients in LMICs. Understanding genetic predispositions, mutational profiles, and molecular factors contributing to CRC in younger populations could provide valuable insights into regional differences in disease biology and inform tailored prevention and treatment strategies.
This study highlights significant disparities in the presentation, treatment, and outcomes of mCRC patients in Pakistan. The younger age of onset, limited access to advanced treatments, low surgical intervention rates, and high prevalence of advanced disease at presentation underscore the challenges of managing mCRC in an LMIC. Addressing these gaps through improved public awareness, enhanced diagnostic and treatment infrastructure, and targeted research efforts is imperative for improving outcomes in this population (Table 4).
Strategic Solutions to Address Gaps in Metastatic Colorectal Cancer Care in LMICs.
| Challenge | Strategic Solution |
|---|---|
| No screening programs | Pilot regular screening in high-risk districts; scale up via primary care |
| Delayed diagnosis | Train frontline providers on CRC symptoms and referral pathways |
| Limited diagnostics | Establish regional diagnostic hubs with public-private partnerships |
| Limited access to chemotherapy | Expand essential medicine list and implement pooled drug procurement |
| High out-of-pocket costs | Launch targeted subsidy programs through national insurance or NGO support |
| Fragmented care | Standardize treatment via tumor boards and national care pathways |
| Poor data systems | Develop hospital-based CRC registries with digital tools (e.g., REDCap) |