
Accurate staging of prostate cancer with imaging is crucial for diagnosis and forming appropriate treatment plans for patients. EAU guidelines currently recommend all patients with high-risk prostate cancer, and those with intermediate-risk and Gleason 4+3=7 histology, undergo cross-sectional abdominopelvic imaging and bone scan (1). This recommendation is based on two single-centre retrospective studies, that included just 40 and 13 patients respectively with ISUP Grade 3 histology (2,3), and pre-date the multiparametric MRI prostate era.
Conventionally, this staging is performed using CT and nuclear medicine bone scans. However, there is concern that conventional imaging techniques have insufficient sensitivity and specificity to accurately detect extra-prostatic disease in high-risk patients (4,5). We aimed to identify the detection rates of metastatic disease, specifically for patients with intermediate-risk prostate cancer with Gleason 4+3=7 histology, using CT and bone scan. We also aimed to identify the oncological outcomes of these patients who subsequently proceeded to robot-assisted laparoscopic prostatectomy (RALP) to help determine whether distant metastatic disease was missed on imaging.
We performed an institutional retrospective analysis of patients using a study population of patients at East Kent University Hospitals NHS Foundation Trust (eKUFT) in Kent, UK who underwent prostate biopsy between 2017 and 2023. The catchment area of eKUFT is approximately 700,000 people. The study design was a retrospective cohort study. The study aims were to:
- a)
Identify the detection rates of metastatic disease using conventional staging scans (CT and Bone Scan) in patients diagnosed with Gleason 4+3=7 prostate cancer.
- b)
To identify the proportion of Gleason 4+3=7 patients who developed metastatic disease post RALP in this cohort, who had negative staging beforehand, to demonstrate missed metastatic disease on imaging.
Radiological exam results after multidisciplinary team (MDT) review were assessed. From the MRI, prostate volume and Prostate Imaging Reporting and Data System (PIRADS) scoring were analysed for demographic data. CT scans and bone scans were considered either positive, negative or equivocal depending on findings as reported. Equivocal results were subsequently determined to be positive or negative after either MDT discussion or further imaging. No statistical analysis was required.
Any patient who proceeded to RALP after negative staging scans were included for sub-analysis to assess if metastatic disease. was missed on imaging. Patients were excluded if they had positive surgical margins at final histology. Missed metastatic disease on imaging was defined as any patient with positive lymph nodes at dissection or biochemical recurrence (defined as PSA >0.2ng/ml on two consecutive measurements) in those with negative surgical margins. Median follow up was included for each patient.
A total of 169 patients were initially identified. Sixteen patients had PSA ≥20ng/ml, four had MRI stage >T3b and three had both. Twelve patients had neither CT or bone scans and were excluded, leaving 134 patients for analysis (Table 1). Median age was 72 (range 45–83), PSA 7.8ng/mL (range 1.8–19.3) and prostate volume 40cc (range 10–129). 130/134(97%) had MRI scans prior to staging. 124/134(93%) patients had bone scans and 83/134(62%) had CT scans, of which 77/134 (57%) had both.
Patient demographics and staging scans for patients with Gleason 4+3 intermediate risk disease.
| Patient demographics (n=134) | Median (range or %) |
|---|---|
| Age | 72 (45 – 83) |
| PSA (ng/mL) | 7.8 (1.8 – 19.3) |
| Prostate volume (mL) | 40 (10 – 129) |
| Biopsy type | |
| TRUS | 14 (10) |
| Transperineal | 120 (90) |
| MRI prostate (n=130) | |
| PIRADS 2 | 15 (11) |
| PIRADS 3 | 9 (7) |
| PIRADS 4 | 66 (51) |
| PIRADS 5 | 40 (31) |
| MRI T stage | |
| T1 | 8 (6) |
| T2 | 74 (57) |
| T3a | 48 (37) |
| MRI N Stage | |
| N0 | 128 (98) |
| N1 | 2 (2) |
| MRI M stage | |
| M0 | 130 (100) |
| Bone scan (n=124) | |
| NM Bone scan | 121 (98) |
| SPECT CT | 3 (2) |
| CT scan (n=83) | |
| CT chest / abdomen / pelvis | 77 (93) |
| CT Urogram | 4 (5) |
| CTKUB | 1 (1) |
| CT abdomen / pelvis | 1 (1) |
| Both CT & Bone scan (n=77) | 77 (53) |
120/134(90%) prostate biopsies were transperineal rather than transrectal. Median cores involved were 8 (range 1–20), percentage of cores involved was 24 (range 3–100), percentage of Pattern 4 was 75 (<5–90) and maximum tumour length 9mm (range 1–17). 70/134 (52%) patients had bilateral Gleason 4+3=7 disease.
0/124(0%) bone scans identified metastatic disease (Figure 1). 4/124(3%) were initially deemed equivocal; two were determined negative at MDT discussion and two confirmed negative on PSMA PET/CT. 1/83(1%) CT scans identified clear metastatic disease, which was already seen on MRI prostate. Three equivocal scans were found; 2/83(2%) showed borderline enlarged iliac lymph nodes and were deemed indeterminate at MDT and thus considered positive. One scan showed a rib abnormality, subsequently proved negative with PSMA PET/CT. Management changes as a result of imaging occurred in 0/134(0%) of all patients.
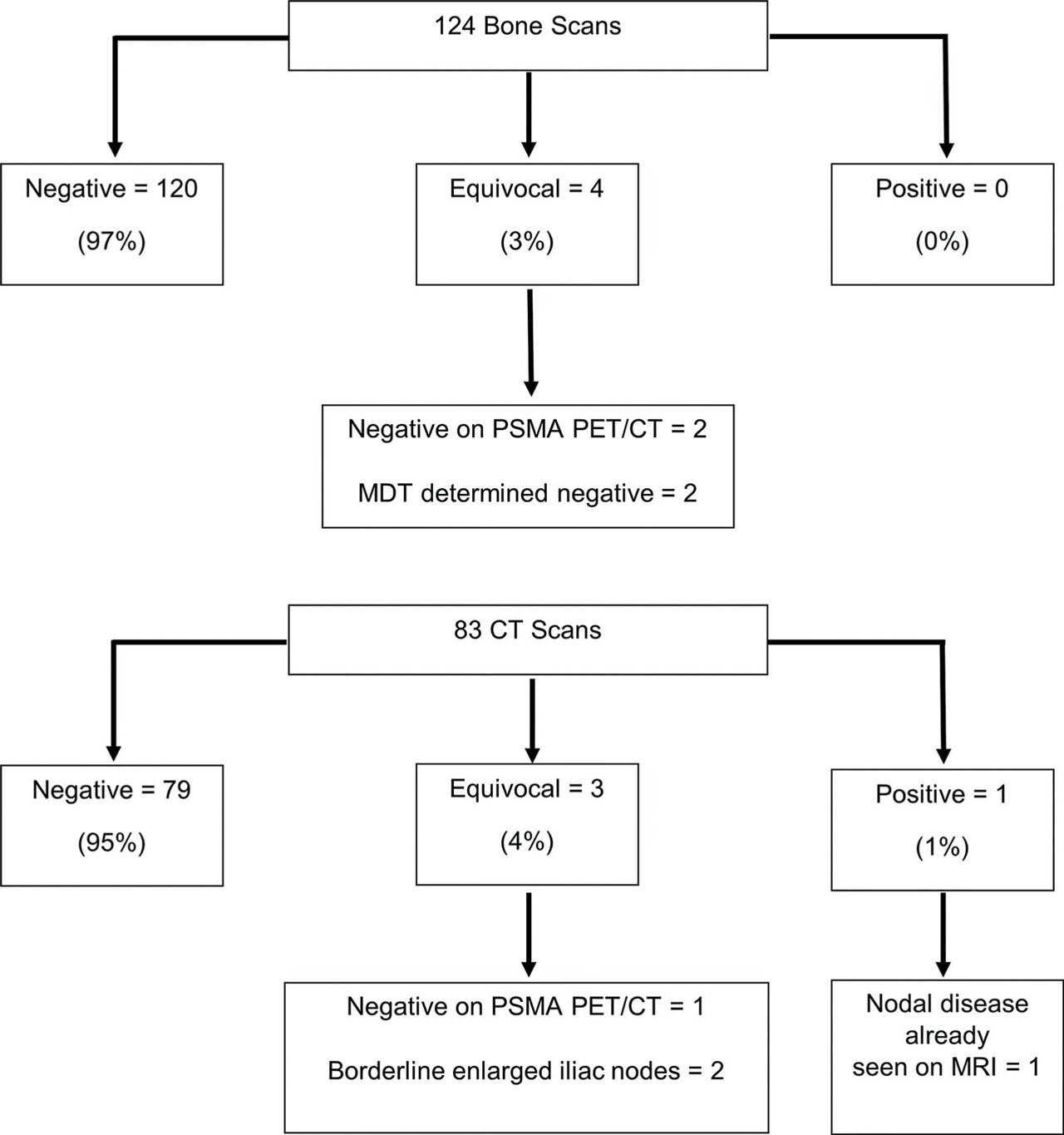
Detection of metastatic disease using both bone scan and CT in Gleason 4+3 intermediate risk disease.
59/134(44%) patients proceeded to RALP, of which 19(32%) patients had lymph node dissections. 57/59(97%) had staging with bone scan and abdominopelvic imaging using either MRI or CT, of which 32/59(54%) had MRI, CT and bone scan. In the 57 patients staged with bone scan & either CT or MRI, 6(11%) patients had metastatic disease missed on conventional staging scans; 3(5%) had biochemical recurrence despite negative surgical margins and 3(5%) had positive lymph nodes at dissection (Table 2). In the 32 patients staged with all three modalities of MRI, CT and bone scan, 2(6%) had missed disease; 1(3%) biochemical recurrence and 1(3%) positive lymph nodes at dissection. Median length of follow up was 18.7 months (range 2.3 – 49.1). Final histopathology at RALP showed 31/59 (51%) were ISUP Grade 3; 20/59 (34%) were downgraded to ISUP Grade 2 and 8/59 (14%) were upgraded to ISUP Grade 5.
Staging scans performed in patients with missed metastatic disease prior to RALP.
| PSA ng/mL | MRI T stage | Bone Scan | CT CAP | Lymph node dissection | Biochemical recurrence | Post-op PSMA PET/CT | |
|---|---|---|---|---|---|---|---|
| Patient 1 | 18.0 | T3a | Negative | Negative | Negative | Yes | Positive |
| Patient 2 | 6.4 | T2c | Negative | Not performed | Not performed | Yes | Negative |
| Patient 3 | 5.3 | T3a | Negative | Not performed | Negative | Yes | Not performed |
| Patient 4 | 5.5 | Not performed | Negative | Negative | Positive | No | n/a |
| Patient 5 | 3.9 | T3a | Negative | Negative | Positive | No | n/a |
| Patient 6 | 4.7 | T3a | Negative | Not performed | Positive | No | n/a |
Our study found the ability of bone and CT scans to detect metastatic disease in intermediate risk disease with overall Gleason 4+3=7 histology was poor. This finding is in contrast to previous retrospective studies (2,3) on which the EAU recommendation was made. The EAU recommendations are almost twenty years old, are based on a small number of ISUP Grade 3 patients, and pre-date routine use of multi-parametric MRI scans.
Consensus on when to stage patients with CT and bone scan is also lacking. NICE has cited an absence of evidence regarding when bone scans should be performed and recommended for research in this area (6). Their use in high-risk disease groups is also questionable: one study involving 125 patients with T3a disease, no patients had positive bone scans when excluded for PSA ≥20ng/mL or ISUP group Grade ≥3 (7). CT scans too have shown poor detection rates of visceral metastases, with studies showing initial prostate MRI scan confers adequate staging information in itself (8). Despite this, a significant proportion of fully-staged patients will have positive lymph nodes at dissection or future biochemical recurrence, as evidenced by our own results. This number is likely to increase as length of follow up increases also.
The use of Prostate Specific Membrane Antigen (PSMA) PET/CT as alternative staging to CT and bone scan has increased in popularity in recent years. This follows several retrospective studies showing improved diagnostic accuracy compared to CT and bone scan (9,10). These were validated in the ProPSMA trial; a multi-centre prospective randomised controlled trial, which demonstrated greater sensitivity and specificity for distant and nodal metastases in high-risk prostate cancer when directly compared to CT and bone scan, as well as fewer equivocal findings (11). Earlier detection with PSMA PET/CT has the potential to facilitate radiologically guided lymph node dissection at RALP (12). Negative scans could also obviate the need for lymph node dissection and its associated morbidity, although this is not a consensus in guidelines as yet, reflecting both the uncertainty in the ability of PSMA PET/CT to exclude nodal disease and furthermore the clinical utility of node dissection in terms of prognostic impact.
However, most evidence for PSMA PET/CT currently relates to detection of metastatic disease in high-risk prostate cancer, rather than specifically in intermediate risk and primary pattern Gleason 4. Furthermore, the high cost of PSMA PET/CT precludes its routine use in clinical practice, although the access to PSMA PET/CT is steadily improving. In the 2023 guidelines, the National Comprehensive Cancer Network (NCCN) recommend the use of PSMA PET/CT as the first-line imaging option for primary staging of Prostate cancer, based on its higher sensitivity and specificity, compared to CT and bone scan (13,14). EAU is yet to endorse this recommendation although as of 2024, it has modified its stance of 2023 from “Treatment should not be changed based on PSMA PET/CT findings, in view of currently available data,” to “Results from RCTs (…) are awaited before a recommendation can be made to treat patients based on the results of these tests” (15). This reflects the current paucity of evidence demonstrating improved survival benefit from early detection and treatment of oligometastatic disease (16,17) compared to proceeding directly to radical treatment. Our study’s strengths include larger numbers of intermediate-risk ISUP Grade 3 patients than the studies cited by the EAU for performing staging scans in this cohort (2,3). It also helps redefine the role of traditional staging scans in the modern diagnostic work-up of prostate cancer, given the widespread use of multi-parametric MRI for accurate staging and more accurate histology with MRI targeted biopsies. Its limitations include its single-centre retrospective nature and further evidence would be required to validate its results.
Detection of metastatic disease by conventional CT and bone scan was low in patients with intermediate risk prostate cancer and Gleason 4+3=7 histology. Patients should either undergo more sensitive staging with PSMA PET/CT or proceed directly to radical treatment due to the theoretical benefit of treating patients with oligometastatic disease. Further large scale multicentred studies are warranted.