
Breast hamartomas are benign masses, consisting of variable amounts of glandular, fibrous tissue, epithelial elements and fat (1). Hamartomas can be called as lipofibroadenoma, fibroadenolipoma, or adenolipoma, depending on their composition. Myxoid hamartoma is rare hamartoma that contain considerable amounts of smooth muscle tissue (2).
The usual age of presentation is in middle aged females above 35 years with incidence around 4.8%, however the incidence is likely increased due to breast cancer screening programs. Breast hamartomas are usually asymptomatic, or can present as a painless soft breast lump or unilateral breast enlargement with an impalpable mass (3).
If the mass is well circumscribed with characteristic pseudocapsule and no suspicious features of malignancy on mammography and ultrasound, there is no need for intervention. Further assessment with biopsy is indicated in cases with suspicious findings on ultrasound or mammography (1).
51-year-old female presented to a symptomatic breast clinic with a long standing lump in her left breast. Clinical examination of left breast showed a soft mobile mass. Examination of axilla was normal. Full field digital mammography (FFDM) and ultrasound (US) of left breast was performed. Mammography showed well encapsulated 70mm heterogenous mass consistent with a breast hamartoma in the lower inner left breast with lucent and dense areas mimicking breast tissue. The center of the hamartoma showed an area of distortion with associated calcification (Figure 1a&b). On US there was an oval, well defined heterogenous mass with posterior acoustic shadowing area (Figure 2a&b). Imaging raised suspicion of underlying malignancy within the hamartoma, and a 14 G ultrasound guided core biopsy was performed through the distortion and biopsy marker placed.
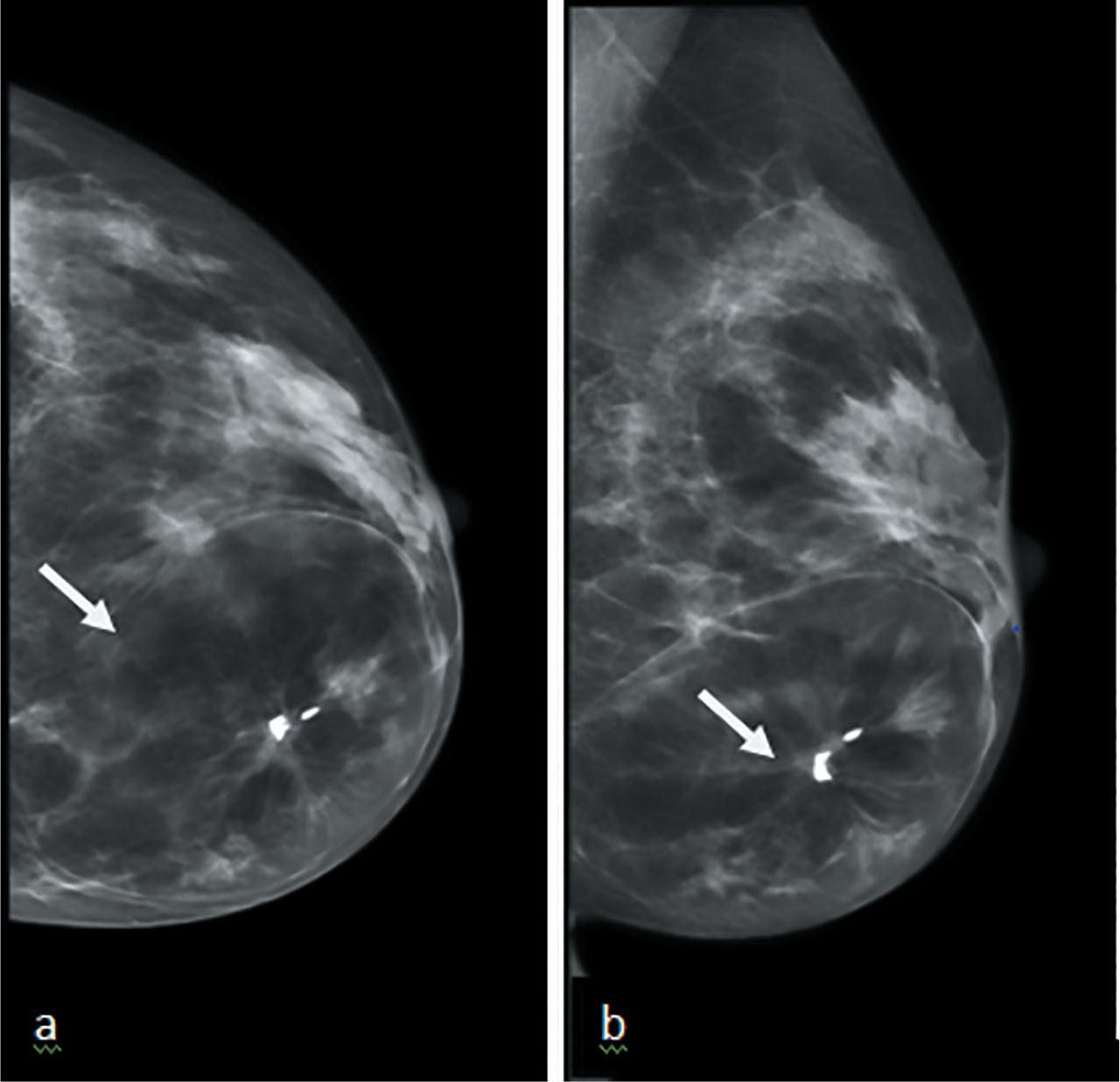
(a) CC and (b) MLO views of hamartoma, seen as encapsulated heterogenous mass in the lower and inner breast with central macrocalifications and distortion (arrows).
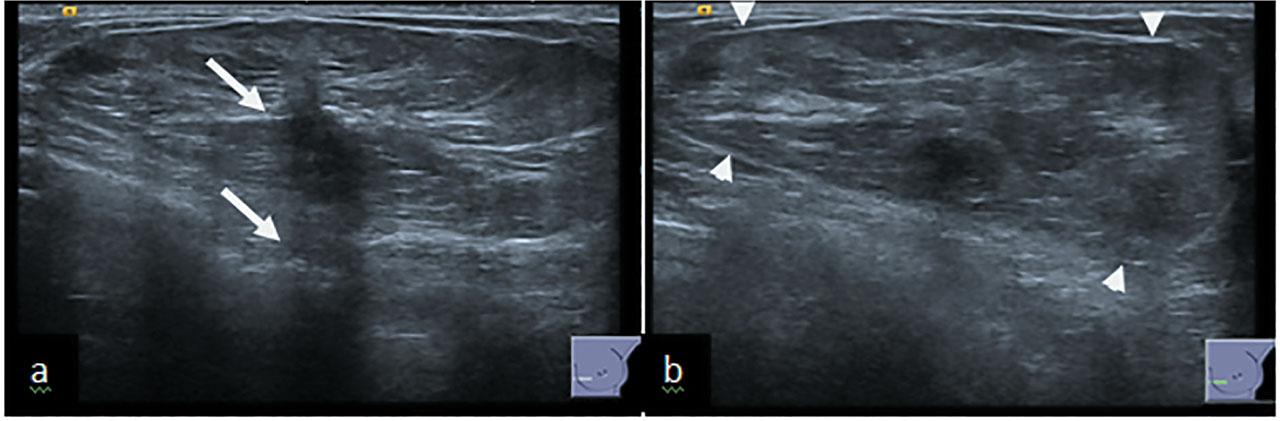
(a) US of hamartoma showing a central small hypoechoic area with associated acoustic shadowing (arrow). (b) The thin echogenic pseudocapsule can also be appreciated (arrowheads).
A 61 year old woman was recalled for assessment after a screening mammogram. She was known to have long standing benign lump in her left breast which had shown interval development of central distortion. On clinical palpation, there was mobile mass in left breast. Digital breast tomosynthesis was performed which confirmed the presence of architectural distortion (Figure 3a&b). Ultrasound showed an oval encapsulated mass running parallel to the skin with central hypoechoic areas (Figure 4a&b). The central distortion and corresponding hypoechoic change was suspicious, therefore 14G US guided core biopsy was performed.
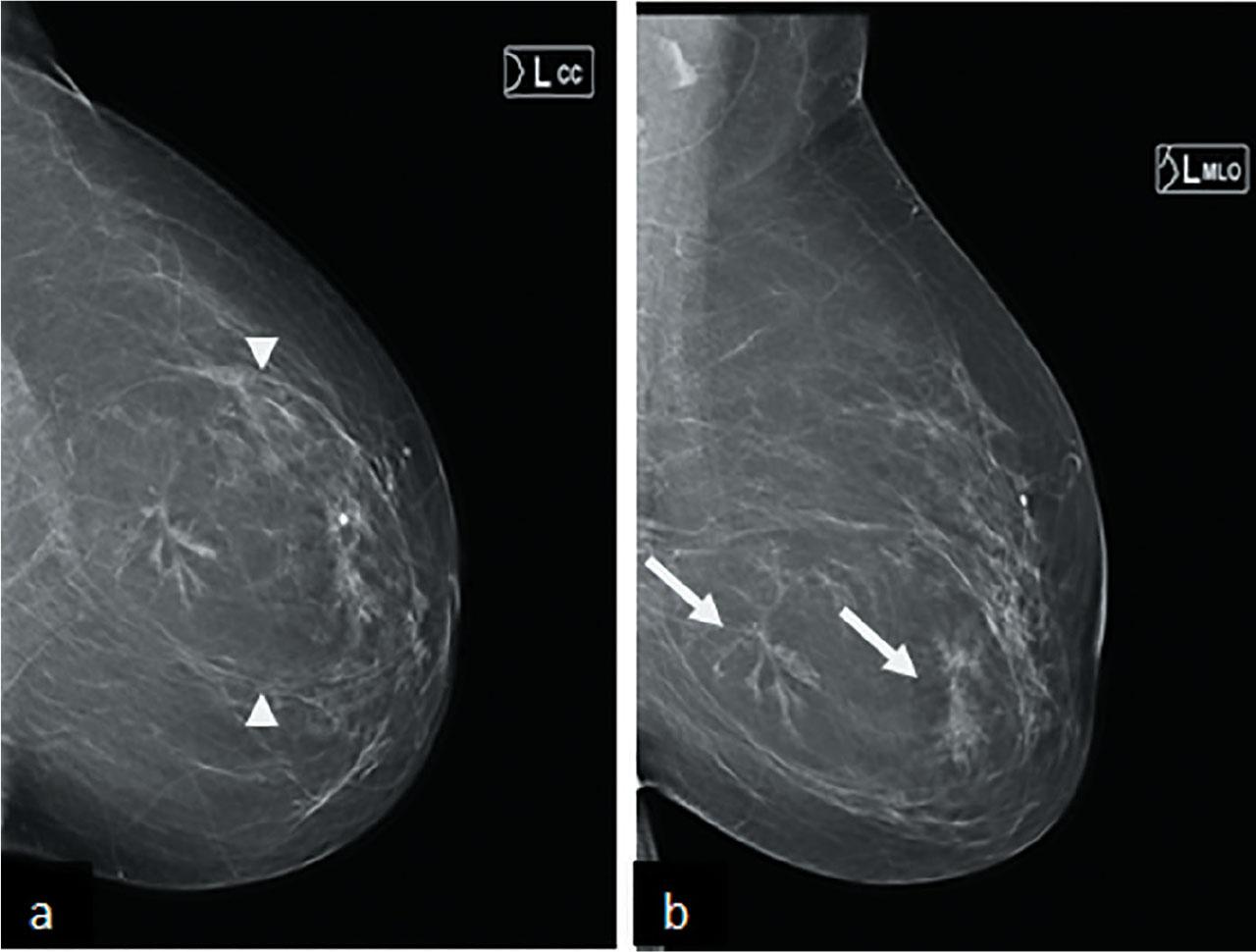
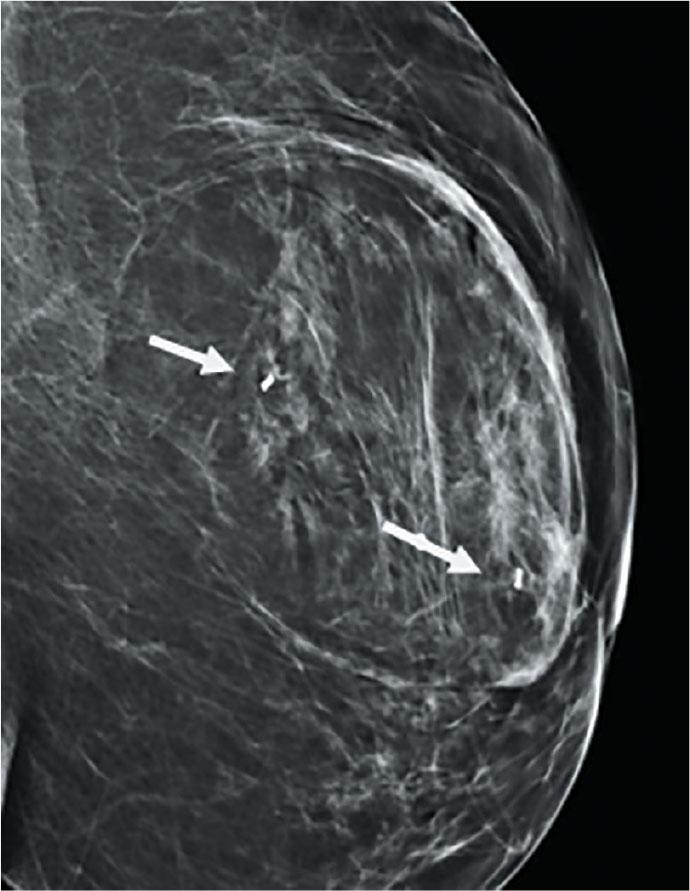
(a) CC and (b) MLO views of mammogram, showing circumscribed mass with pseudocapsule (arrow heads) and central area of distorsion (arrow) in the left lower central breast.
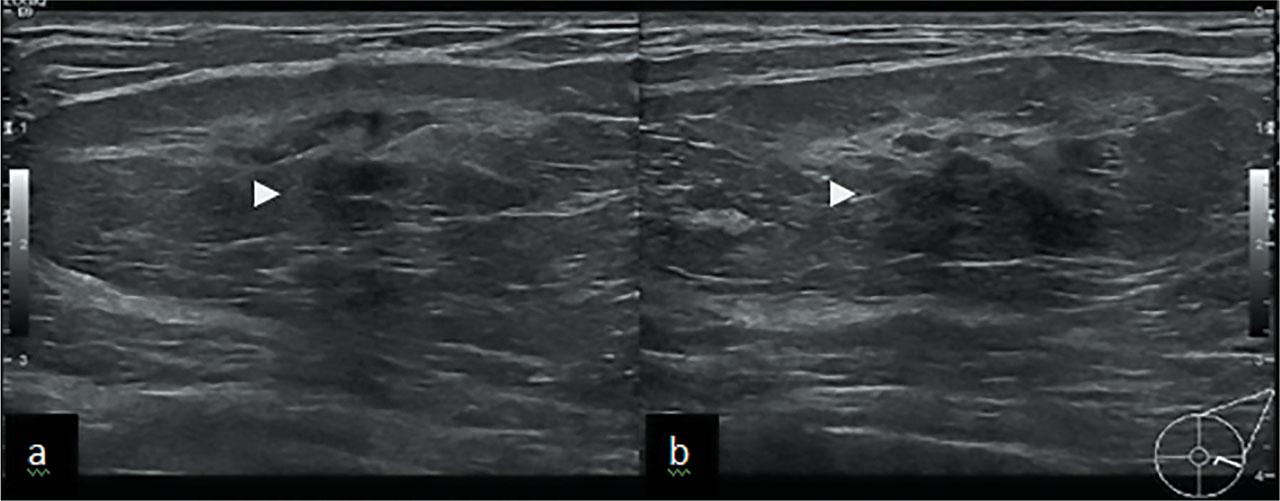
US shows well defined oval mass with central hypoechoic shadowing area (arrowheads) corresponding to mammographic distortion.
The pathology report showed normal fibro fatty breast tissue, consistent with a hamartoma. The case was discussed in the multidisciplinary team meeting (MDT). Imaging and pathologic findings were not concordant as the pathology result did not provide an acceptable explanation for the imaging features, therefore the MDT decision was for repeat biopsy. The patient underwent stereotactic guided vacuum assisted biopsy (VAB) with six, 10 gauge samples obtained. The biopsy was examined at multiple levels and showed fibro fatty breast tissue with an area of stromal fibrosis and focal chronic inflammation, again benign (B2). The case was rediscussed at MDT meeting. Without an adequate explanation for the associated distortion and microcalcification surgical excision was discussed. However due to the large size of the lesion, concern was raised about the potential cosmetic outcome if an open surgical excision was performed and tomosynthesis guided vacuum assisted excision, as an alternative to a surgical diagnostic biopsy was suggested. This time 24 cores were taken using the 10 G biopsy needle, sampling the distortion and retrieving the calcifications. The histopathology results showed fibrocystic change with sclerosing adenosis, extensive fat necrosis, two large fragments of stromal calcification in fibrous tissue and fine calcification in glands. No malignant features were identified. Following further MDT discussion, the benign histology result was now considered to be representative of the area of radiological concern and so the patient was discharged.
The biopsy showed fibrofatty tissue, consistent with hamartoma, B2. At the MDT, the biopsy result was not considered to reflect the radiological features and so stereotactic VAB specifically targeting the distortion was undertaken. A post biopsy mammogram demonstrated the biopsy marker clips positioned in the areas of distortions (Figure 5). The histopathology was benign. No further intervention was recommended at the MDT and the patient was discharged to normal screening.
Mammogram showing post VAB marker insertion (arrow).
Breast hamartoma shows variable amount of fat and soft tissue, is seen as well-circumscribed rounded or oval mass on mammograms, classically surrounded by a thin pseudocapsule (1,4). Hamartoma can resemble a slice of salami as there is presence of scattered nodular opacities within the translucent fat contained in the pseudocapsule. Hamartomas can be difficult to differentiate from fibroadenomas if it contains relatively high amounts of fibrous tissue and appear homogeneously dense. Hamartomas can resemble lipomas, foci of liponecrosis, or oil cysts if composed mainly of adipose tissue (2). The classic description is the term breast within a breast appearance.3 In both our cases hamartomas gave typical appearance of breast within breast appearance however it was internal area of distortion which raised suspicion of underlying sinister pathology within the hamartoma. In dense breast, hamartomas can present as heterogeneously increased asymmetric density without pseudocapsule, making detection more difficult (5). In our patients the pseudocapsule was well seen.
The ultrasound appearances of hamartomas can be variable owing to differing amounts of adipose and fibrous tissue. Mostly hamartoma appear as well defined solid masses lying parallel to the skin plane. The internal texture may consist of hypoechoic areas representing fat and scattered areas of mixed echogenicity, representing the presence of different tissue elements. It can be well encapsulated or the margins can be difficult to delineate. Hamartoma can also show microcalcification. Exact measurement can be difficult when pseudocapsule is not well seen (1,3). On US both our cases were seen as well defined heterogenous masses lying parallel to breast tissue planes with a thin pseudocapsule.
Correlating imaging-pathology concordance after biopsy is important for validating the biopsy result and providing appropriate management. The pathology needs to provide an adequate explanation for the radiological findings. In our cases, both lesions were radiologically suspicious, but histology was benign. Radiological-pathological concordance was only achieved after repeat biopsy with thorough x-ray guided sampling, with a large bore vacuum assisted biopsy and MDT discussion.
Hamartomas with typical findings on imaging studies, require no further diagnostic procedures or follow-up. Hamartomas are not a risk factor for breast cancer. Malignancies associated with breast hamartomas are rare, and only a few studies have reported breast cancer associated with hamartoma, suggesting possible malignant transformation of breast hamartomas.6 Malignant transformation although rare, can occur since the mass contains epithelial element. Mani c et al, in a review of the literature, described 15 cases of carcinoma associated with hamartomas. In the majority of cases, the diagnosis was made as a result of suspicious imaging features on mammogram such as clusters of pleomorphic or amorphous microcalcifications, spiculated opacities or asymmetry within an otherwise typical appearing hamartoma (2,7,8,9). Our cases exhibited areas of distortion on mammography within the hamartomas which raised the level of suspicion. However in both cases despite unusual imaging features, histology was benign.
The sonographic appearance such as irregular margins or vertically orientated masses or an irregular hypoechoic mass within the hamartoma should also raise the suspicion of malignancy (2,7,8,9). In both our cases hamartomas were seen as heterogenous well defined masses. The area of distortion on the mammogram corresponded with an illdefined hypoechoic areas with posterior acoustic shadowing on ultrasound which also increased the level of suspicion.
Ductal carcinoma in situ, lobular carcinoma in situ and invasive ductal carcinoma have been reported within hamartomas. Ductal epithelial hyperplasia has also been reported in hamartomas. The literature suggests that any suspicious features even with typical mammographic or sonographic findings should warrant further evaluation and biopsy (7,8,9). The first patient underwent US core biopsy, stereotactic vacuum assisted biopsy and excision following MDT decision. The second patient also underwent tissue sampling twice, but in both cases histopathology results were consistent with benign pathology of fibrofatty tissue with stromal fibrosis and focal chronic inflammation.
In conclusion, when atypical imaging features are demonstrated within a hamartoma then further investigation and biopsy is indicated. MDT discussion is crucial in the management of these cases to ensure radiological-pathological concordance.