
Acute myeloid leukemia (AML) is a heterogeneous disorder characterized by clonal expansion of myeloid precursors in the bone marrow and peripheral blood (1). The clonal proliferation of an aberrant, committed stem cell at the level of Colony forming unit stem cells or later stages of differentiation, results in the accumulation of immature forms with or without restricted maturity. AML, which was once incurable, is now treated in 35%–40% of patients under the age of 60. The prognosis is bleak but improving for patients over 60 years of age as well. Over the past ten years, there have been significant changes in the clinical assessment and prognosis of patients with AML.
For diagnosis, categorization, and risk assessment, bone marrow aspirate and biopsy, including morphology assessment, immune-phenotyping, cytochemistry, and genetics testing are crucial. Our comprehension of the pathophysiology and prognosis of AML has been aided by studies in the fields of molecular biology, cytogenetics, and immunology (2). Patients with AML have a median age at diagnosis of 68 years, and because they cannot receive rigorous chemotherapy, their options for effective treatment are frequently limited (3). In this population, low dose cytarabine (LDAC) or hypomethylating drugs (azacitidine, decitabine) can be utilized, however they have been linked to subpar results. The combination of venetoclax plus hypomethylants was associated with a higher response rate and better overall survival according to preliminary findings and subsequent confirmatory data as reported by DiNardo et al (4). To treat newly diagnosed AML patients who are poor candidates for rigorous chemotherapy due to age or comorbidities, the Food and Drug Administration (FDA) has extended the indication for venetoclax. It can now be used in combination with azacitidine, decitabine, or LDAC (5).
The BCL-2 family of molecules, which control the intrinsic apoptotic pathway have been linked to tumorigenesis as well as cell survival in numerous haemato-oncological malignancies (6). Research has demonstrated that stem cells require BCL-2 for survival, and that its inhibition can promote apoptosis in these cells. Abnormal over expression of BCL-2 has been observed in AML cells. Oral venetolcax, which is highly selective for BCL-2, has demonstrated strong anti-leukemic action in AML cell lines (6). The primary objective of our study is to determine the overall survival (OS) of elderly AML patients taking venetoclax in conjunction with azacitidine. We describe the clinical and disease-related characteristics of individuals diagnosed with AML at our institution over the last 5 years.
This was an observational retrospective study conducted at Aga Khan University Hospital (AKUH), a tertiary care hospital in Karachi, Pakistan, from January 2018 to December 2023. The sample consisted of 58 diagnosed AML patients, who were ≥ 50 years of age and treated with venetoclax in combination with azacitidine. The diagnosis of AML was made after reviewing routinely stained peripheral blood smears and bone marrow biopsies/aspirates according to the World Health Organization criteria (7). Patients were risk stratified according to European Leukemia Net (ELN) stratification with the majority of patient’s falling in the intermediate risk group (8). Cases of primary AML, transformed AML, AML secondary to therapy and relapsed/refractory AML were all included in our analysis. However, we excluded patients with myelodysplastic syndromes who were treated with Azacitidine.
On obtaining ethical approval from the institution’s “Ethical Review Committee” (AKU-ERC #: 2023-9071-27189), relevant data regarding the patients was extracted from the hospital’s information management system. In order to ensure standardized data extraction, a proforma was prepared digitally and utilized by the investigators for data collection. We retrieved the patients’ dates of diagnosis, and information regarding the outcome of each patient. The date of death, or last follow up with the hospital was also recorded. Additionally, we obtained information regarding any cytogenetic or molecular testing performed, the white cell counts at initial presentation, and the number of cycles of venetoclax and azacitidine received by the patients.
The majority of patients in our cohort were receiving antifungal prophylaxis with voriconazole 200 mg twice daily. As a result, the dose of venetoclax was adjusted to 100 mg once daily in most patients for a total of 28 days. However, in the case of severe neutropenia and sepsis, venetoclax was stopped at day 14 or earlier. Azacitidine was administered once daily rounded of to a dose of 100mg for a total of 7 days. This constituted a single cycle. The maximum number of cycles for these regimens is unknown, and treatment may continue as long as tolerated and effective.
BM biopsy for response assessment was performed on day 28 of the first cycle. Even if there was no morphologic remission (persistent blasts > 5%) we proceeded with the second cycle when clinical improvement was indicated by hematologic parameters such as recovering of platelet counts, improving hemoglobin levels and transfusion independence. The marrow biopsy was repeated on day 28 of the second cycle to establish whether morphologic remission was achieved. If there was no evidence of disease after the first cycle, then no further bone marrow examination was required, and sequential cycles were continued with up to 14-day interruptions between cycles for count recovery and/or growth factor support. If count recovery worsened over time, we ruled out relapsed disease with by repeating a marrow biopsy. If morphologic remission was ongoing however, with worsening blood counts, we reduced the dose of venetoclax and/or azacitidine.
The data was analysed using Statistical Package for the Social Sciences version 21 (SPSS 21). Categorical variables were described using frequencies and percentages whereas continuous variables were summarized using either means and standard deviations or medians and interquartile ranges. We conducted a survival analysis on our cohort with the outcome event as death. The date of diagnosis was used as the starting time. Kaplan-Meier survival curves were generated for overall survival (OS), survival by gender, and survival by comorbid status. Additionally, we used the log-rank test to compare median overall survival times for both the genders and the presence of comorbid conditions. Patients lost to follow-up, or alive at the end of the observation period were right censored. The multivariable Cox proportional hazards regression model was used to adjust the p values and hazards for key factors. All results have been quoted with their 95 percent confidence intervals. A p value less than 0.05 was considered statistically significant for all tests.
Our cohort comprised of 58 patients with confirmed Acute Myeloid Leukemia. Of these, 11 (18.9%) were cases of transformed or secondary leukemia. The median age in our cohort was 61.5 [55.0 – 67.0] years. A majority of our patients were males (77.6%). In 75.9 % of cases the final outcome was death, with only 15.5% of cases under treatment at the end of the study period. 70.7 % of our patients had one or more comorbid condition in addition to their AML diagnosis. A majority, 20 (34.5%) of cases had diabetes mellitus. Additional information regarding the characteristics of patients in our cohort can be viewed in Table 1.
Patient characteristics.
| Variable | n (%) or mean ± SD |
|---|---|
| Gender | |
| Male | 45 (77.6) |
| Female | 13 (22.4) |
| Age | 61.5 [55.0 – 67.0] |
| Number of cycles | 4 [2 – 6] |
| White cell counts at presentation | 5.8 [2.4 – 16.1] |
| Outcome | |
| Death | 44 (75.9) |
| Under treatment | 9 (15.5) |
| Palliative care | 1 (1.7) |
| Lost to follow up | 4 (6.9) |
| Secondary leukemia | |
| MDS transformation | 7 (12.1) |
| CMML transformation | 2 (3.4) |
| MF transformation | 2 (3.4) |
| Remission achieved | |
| Yes | 22 (37.9) |
| No | 33 (56.9) |
| Not known | 3 (5.2) |
| Cause of death | |
| Refractory disease | 30 (63.8) |
| Relapsed disease | 10 (21.3) |
| Secondary Cause* | 4 (8.5) |
| Not Known | 3 (6.4) |
| Comorbid conditions | |
| Hypertension | 17 (29.3) |
| Diabetes Mellitus | 20 (34.5) |
| Coronary Artery Disease | 4 (6.9) |
Abbreviations: SD – Standard Deviation, MDS – Myelodysplastic Syndrome, CMML – Chronic Myelomonocytic Leukemia, MF – Myelofibrosis.
Secondary causes includes 3 cases of acute respiratory distress syndrome due to Covid-19 and 1 case of Septic Shock.
20 (34%) of the patients had AML with cytogenetic abnormalities. Of these, a majority – 5 (9%) had complex karyotypic abnormalities including 3 or more chromosomal aberrations. Table 2 provides a detailed overview of the chromosomal abnormalities encountered. 20 (34.5%) patients developed AML with molecular abnormalities, with FLT-3 mutations comprising the majority of cases. Table 3 describes the various molecular mutations encountered in our cohort. Figure 1 describes the proportion of patients presenting with a particular molecular abnormality.
Cytogenetic abnormalities identified in our cohort
| Cytogenetic abnormalities | n (%) |
|---|---|
| Normal | 20 (34) |
| Complex karyotypic abnormalities* | 5 (9) |
| Deletion 7q | 4 (7) |
| Translocation 8:21 | 2 (3) |
| Trisomy 8 | 2 (3) |
| Monosomy X | 2 (3) |
| Deletion 11q | 1 (2) |
| Inversion 16 | 1 (2) |
| Translocation 1:22 | 1 (2) |
| Trisomy 11 | 1 (2) |
| Trisomy 19 | 1 (2) |
| Metaphysis not found | 18 (31) |
Indicated by the presence of 3 or more chromosomal aberrations including deletions, inversions or aneuploidy.
Molecular abnormalities identified in our cohort
| Molecular abnormalities | Count |
|---|---|
| FLT 3-ITD | 7 |
| NPM 1 | 4 |
| Others (CALR, U2AF1, KRAS, PHF6) | 4 |
| IDH-1/2 | 3 |
| TP53 | 2 |
| WT-1 | 2 |
| NRAS | 2 |
| TET-2 | 2 |
| RUNX-1 | 2 |
| JAK2 | 2 |
| ASXL-1 | 1 |
Some patients had multiple molecular abnormalities; the count indicates the number of cases with a given abnormality.
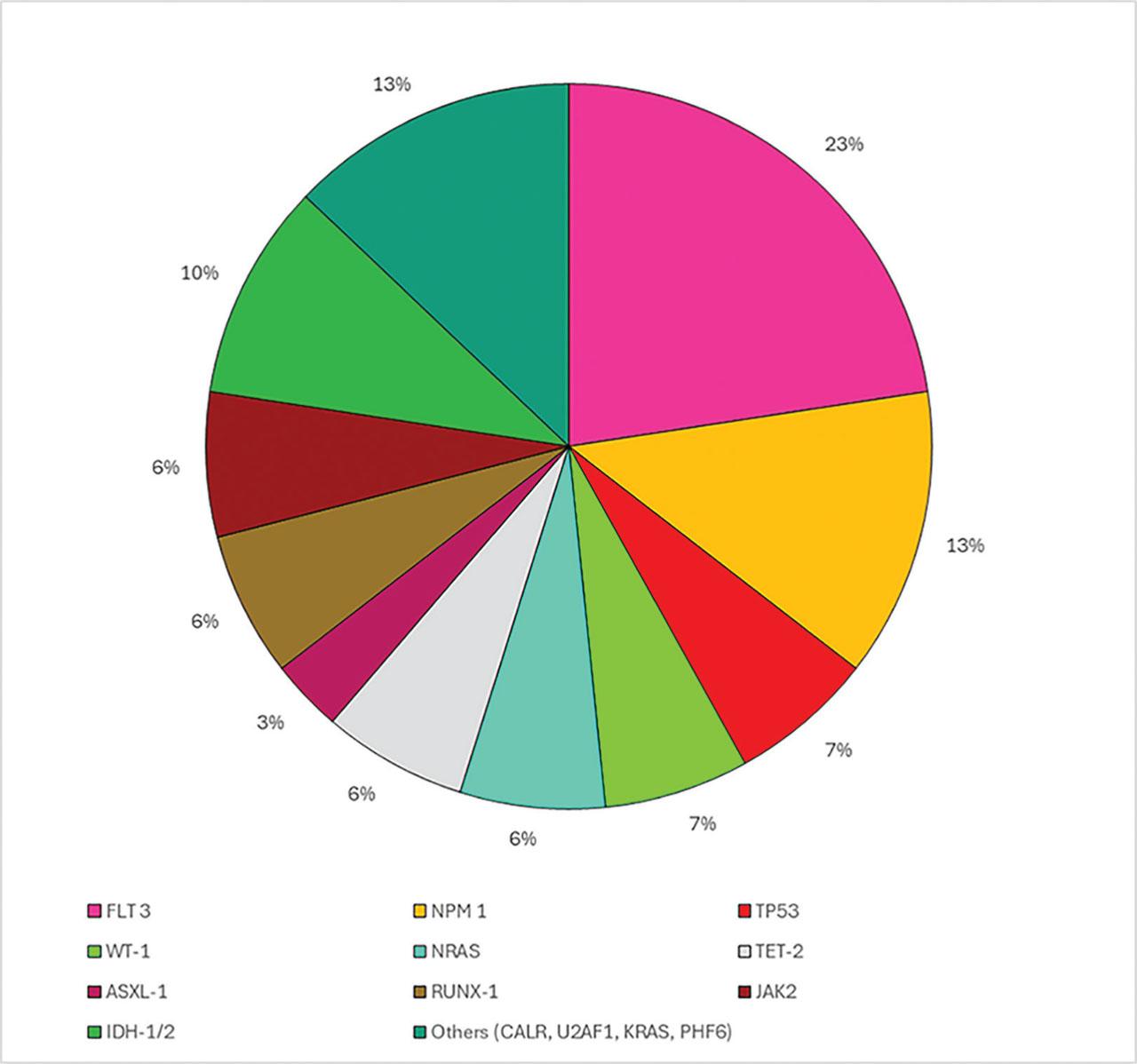
The proportion of different types of mutations observed in the patients.
Figure 2 depicts the Kaplan-Meier curve for overall (cumulative) survival among patients with Acute Myeloid Leukemia who were treated with venetoclax and azacitidine.
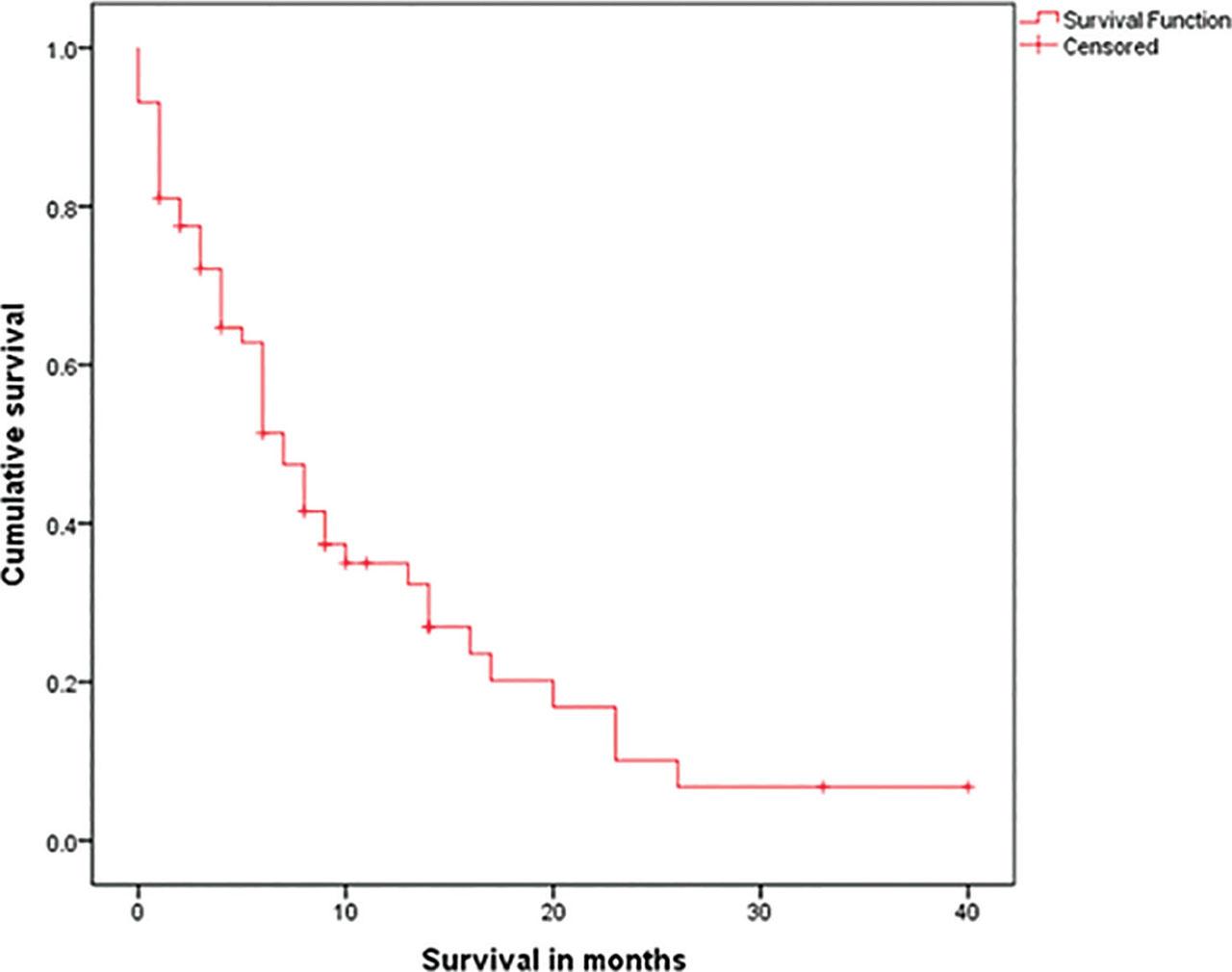
Kaplan Meier Curve for overall survival among patients with Acute Myeloid Leukemia treated with Venetoclax and Azacitidine.
The median OS of patients in our cohort was 7.0 months with a 95% CI of [5.1 – 8.9]. Figures 3 and 4 show the survival stratified by comorbid status and gender respectively. The log-rank test for difference between median survival among patients with and without comorbid conditions was not significant with a p value of 0.586. The median overall survival among males was 6 months [4 – 8], while among females was 16 months [4 – 28], with a p value of 0.021.
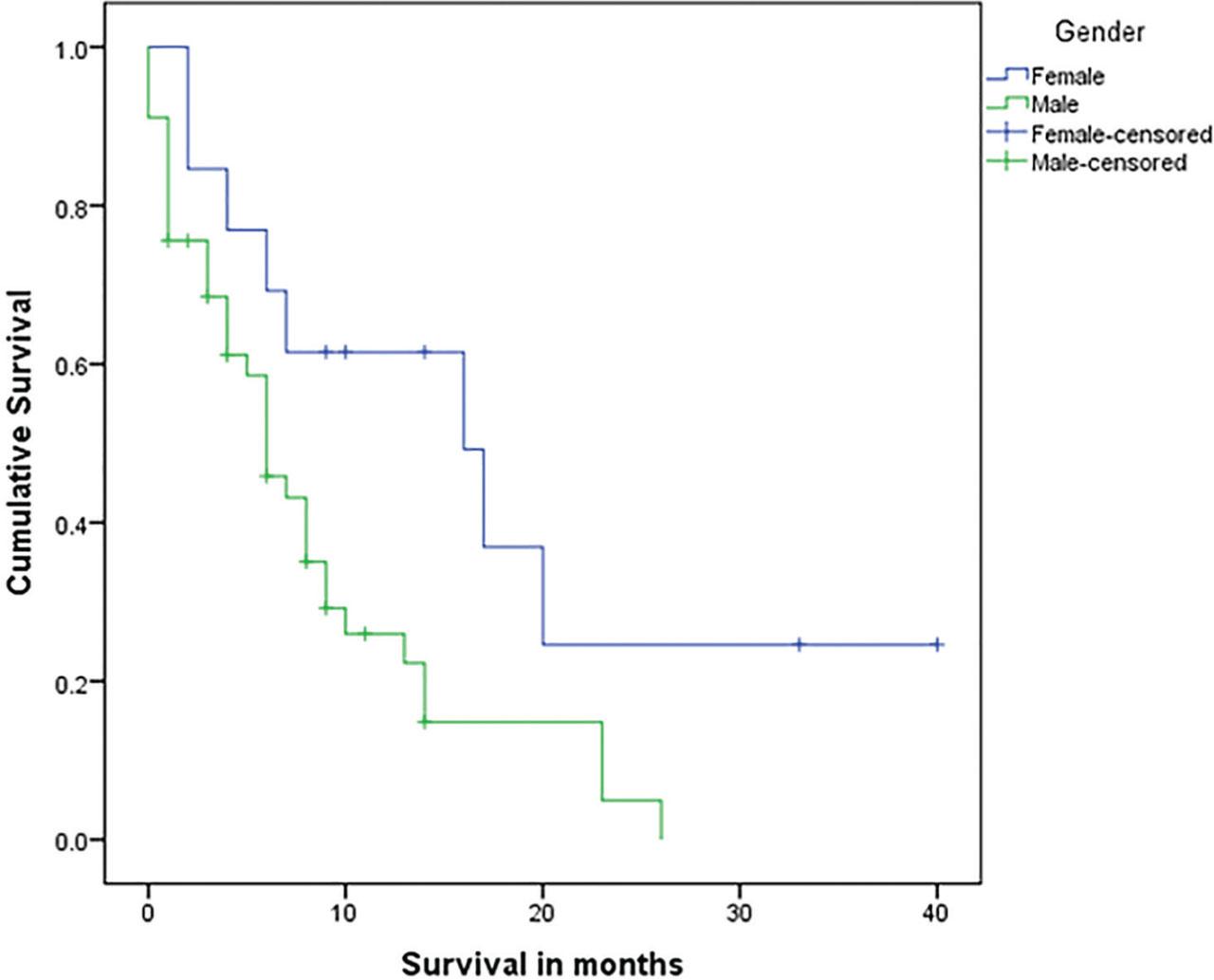
Kaplan Meier curves for overall survival among patients with AML stratified by gender.
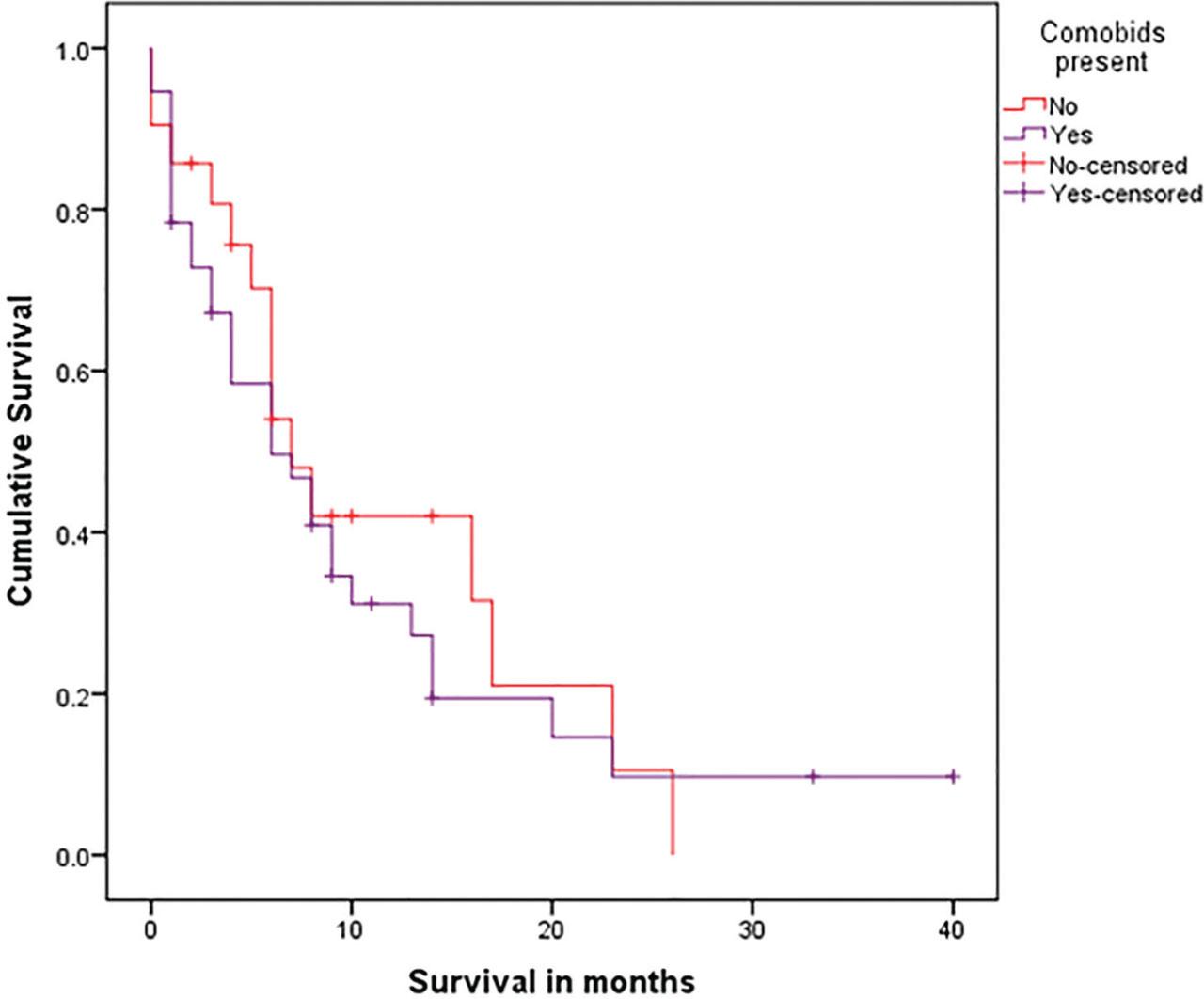
Kaplan Meier curves for overall survival among patients with AML stratified by comorbid status.
Table 4 describes the results of a multivariable regression analysis evaluating the effect of 5 factors on the hazard of death. Among these, only the number of cycles of chemotherapy had a significant impact on overall survival, with a p value < 0.01 and a declining hazard of death with an increasing number of cycles with a hazard ratio of 0.74 [0.61 – 0.87].
Multivariable cox-regression model for predictors of survival in our cohort
| Variable | Hazard Ratio | 95% Confidence Interval | p value |
|---|---|---|---|
| Age | 1.03 | [0.99 – 1.08] | 0.15 |
| Number of cycles | 0.74 | [0.61 – 0.87] | < 0.01 |
| White cell counts at presentation | 1.00 | [0.99 – 1.01] | 0.89 |
| Presence of cytogenetic abnormalities* | 0.82 | [0.40 – 1.71] | 0.60 |
| Presence of molecular abnormalities* | 0.73 | [0.27 – 2.02] | 0.55 |
Absent (No) category is used as reference
In this study, we evaluated the outcomes of patients with Acute Myeloid Leukemia (AML) who received venetoclax in combination with azacitidine at a single center in Pakistan. The primary aim was to assess the efficacy and safety of this combination therapy in a cohort that included patients of varying ages above 50 years and risk profiles. Our findings provide insights into the real-world applicability of venetoclax-azacitidine treatment in a setting that differs significantly from those of previous studies, particularly those conducted in western countries.
When comparing our results with local studies as those of Sajid et al. (2010), who studied the therapeutic outcomes in older patients with AML in a similar regional setting, there are notable differences and similarities (3). Sajid et al. reported on outcomes using conventional chemotherapy regimens, finding that older patients generally had poor outcomes with a low overall survival rate of 75.1 days (2.4 months). Our study, in contrast, demonstrates an improved survival rate in a similar demographic when treated with venetoclax in combination with azacitidine. This suggests that the addition of venetoclax may offer a significant therapeutic advantage over traditional chemotherapy, particularly in older or high-risk patients who are less likely to tolerate intensive chemotherapy.
Moreover, comparison with the pivotal study by DiNardo et al. (2019) further underscores the efficacy of venetoclax combined with azacitidine in treatment-naive elderly patients with AML (4). DiNardo et al. reported higher overall survival rates with a median OS of 14.7 months [95% CI 11.9–18.7]. In our study, although the median overall rates were lower, they still indicate substantial efficacy, which is particularly notable given the different demographic and possibly more challenging clinical setting in Pakistan. This consistency across studies highlights the robustness of venetoclax in combination azacitidine as a viable treatment option in diverse populations
In this study, we observed a median overall survival (OS) of 7.0 months for elderly AML patients treated with Venetoclax and Azacitidine in a developing country, which is comparable to the 8-month OS reported by Mirgh et al. in India (10). While Western studies as conducted by Sylvain et al. (9), Pollyea et al. (11) and Todisco et al. (12) report higher OS of 9.4, 16.4 and 12.7 months, respectively, several factors may explain the differences. In developing countries, delayed diagnoses, higher infection rates, limited supportive care, and socioeconomic challenges often contribute to poorer outcomes. Additionally, real-world patient populations in these settings typically include more high-risk individuals, which further impacts survival. These findings highlight the need for tailored treatment strategies that account for local healthcare constraints and patient characteristics, ensuring that therapies like Venetoclax and Azacitidine can achieve optimal outcomes in diverse settings
The outcomes from our study align with the growing body of evidence supporting venetoclax and azacitidine as a standard of care in AML, particularly for patients who are elderly or have comorbid conditions that preclude them from receiving intensive chemotherapy. The tolerability profile observed in our cohort is consistent with that reported by DiNardo et al., where the combination was associated with manageable adverse events, making it a feasible option in a resource-limited setting. However, our study also points to the need for further research in regional populations to optimize dosing strategies and management of adverse events, which might differ due to genetic, environmental, or healthcare system-related factors. The slightly lower response rates in our study compared to DiNardo et al. may suggest a need for adjustments in supportive care or closer monitoring, particularly in a setting where access to comprehensive care may be limited.
While our study provides valuable insights, it is not without limitations. The single-center design and relatively small sample size limit the generalizability of the findings. Additionally, the lack of a control group receiving alternative treatments means we cannot definitively conclude the superiority of venetoclax-azacitidine to other regimens in our specific population. Nonetheless, the outcomes suggest that this combination therapy is effective and warrants further investigation in larger, multi-center studies within the region.
To our knowledge, this is the first study of HMA+Venetoclax induction from Pakistan. Our findings contribute to the growing evidence that venetoclax combined with azacitidine is an effective treatment option for patients with AML, including those in resource-limited settings. The comparison with existing literature, highlights the potential benefits of this regimen over traditional therapies. Future studies should focus on further validating these results and exploring ways to optimize treatment for regional populations.