The global population of elderly people is increasing. By 2050, the world’s population will include 1.6 billion people over the age of 65, meaning that 1 in 6 people will be elderly.1 For Thailand, it is assumed that by 2050, the elderly population will be around 19 million, accounting for 31.4% of the total population.2 In 2022, the statistics showed that 7.00% of the elderly in Thailand were in the early senior age group (60–69 years old), which was a period when they could still care for themselves. Meanwhile, 3.65% were in the middle senior age group (70–79 years old) when their health began to decline, and they started experiencing chronic conditions. Additionally, 1.82% were in the late senior age group (80 years and older), where illness became more frequent.3 The transition to an aging society significantly impacts the country’s healthcare system.4 Aging leads to physical deterioration that causes major health issues in the elderly (Geriatric syndrome), such as blurred vision, hearing loss, thinning and wrinkling skin, reduction of ability to perform daily activities, decrease in sensory perception, chronic diseases, cognitive impairment, loss of mobility, slower movement, and reduction of joint flexibility and muscle strength.5,6 This can cause an inability to maintain balance while walking or changing body posture, leading to falls, which often occur repeatedly.7 The incidence of repeated falls tends to increase with age, particularly in people aged 65 and above, with 28%–35% of this group experiencing falls.8 The rate increases to 32%–42% for those aged 70 and over.9 Falls are the second leading cause of death after road traffic accidents in the group of unintentional injuries, mostly affecting people over 60 years of age.10 According to the 2022 Health Survey of the Thai Population, >10,000 elderly people fell and were injured in the hip and thigh areas, and 20% of those with hip fractures had a chance of dying within 1 year.11Aging is associated with progressive decline in functional status and psychological health, increases risk of comorbidity, and is related to falls in older adults.
In Thailand, over 2000 people die from falls each year, and nearly half of them are elderly. Males have a death rate 3.5 times higher than females, while elderly females experience falls 1.6 times more frequently than elderly males.12 Falls among the elderly are often caused by accidents such as slipping or tripping over obstacles. Risk factors for falling include gender, age, impaired vision, memory, walking, and balance.13 When elderly individuals fall, they tend to have longer hospital stays compared to younger age groups.14,15 Effective fall prevention measures include exercises to improve walking and balance, education on fall prevention, creation of a safe environment, appropriate medication use, and nutrient provision suited to the needs of the elderly.16 In 2023, Thailand had a total of 13,064,929 elderly people, accounting for 20.08% of the total population. In Chanthaburi Province, there were 112,229 elderly people, making up 21.1% of the province’s population, ranking it as the 28th province with the highest elderly population in Thailand.17 In the past, elderly care focused on providing reactive services such as establishing elderly clinics in hospitals, conducting health check-ups and bone density tests as well as treating falls after they had occurred. However, proactive services aimed at preventing falls among the elderly have not been systematically implemented, even though the trend of falls among the elderly in the community is increasing.
Currently, there is a large amount of research on fall prevention in older adults. However, there is still limited research on fall prevention in older adults who live in the community. Thus, the researchers recognized the importance of establishing a fall prevention program for the older adults in the Chanthaburi community. The objective was to study the effects of a fall prevention program for older adults dwelling in the community in Chanthaburi. The research hypothesis suggested that the fall prevention program would improve the older adults’ knowledge of fall prevention, increase their fall-preventive behaviors, develop their walking and balance, reduce their fear of falling and lower risk of falling.
This study was designed as a randomized pretest-posttest control group, single-blinded (blinded statistician). The trial was registered with the Thai Clinical Trial Register: Identification number TCTR20240802008.
There are 24 elderly schools in Chanthaburi province. The elderly schools are established by sub-district municipalities, which aim to develop the quality of life and promote healthy aging for community-dwelling older adults. Two elderly schools under the supervision of different sub-district municipalities in Chanthaburi province were randomly selected by using a lottery method, then were randomly assigned to either an intervention or a control trial site in order to avoid the potential for contamination of intervention occurring during the trial.
The number of older adults registered at the elderly schools in the intervention site and the control site was 50 and 110, respectively. The researchers approached the older adults attending the regular activities of the elderly schools and informed them about the study. Then, they were screened for eligibility based on the following inclusion criteria: aged 60 years or above, able to understand and communicate effectively in Thai, free from severe complications that would hinder their participation in activities or other conditions that may pose risks during participation, and willing to voluntarily participate in the research. The older adults were excluded if they met any of the following criteria: receiving palliative care; having a diagnosis of heart disease, myocardial ischemia, myocardial infarction, cancer, severe hypertension, severe depression, and severe muscle weakness or taking psychotropic, hypnotic drugs, or antiarrhythmic medications.
In the experimental group, 40 older adults met the inclusion criteria and were willing to participate. Among these, 30 were randomly selected in the study using a computer generator. In the control group, 90 older adults met the inclusion criteria, and 30 older adults were randomly selected for the study. Written informed consent was obtained from each participant.
The sample size was calculated using a G*power analysis with α = 0.05 (2 tail), power 0.80, large effect size 0.80, with a mean of the experiment group = 72.3 (S.D. = 8.6) and a mean of control group = 64.7 (S.D 10.2).18 The sample required at least 26 participants for each group to be able to identify the statistical significance of the intervention. The researchers recruited 30 participants in each group, allowing for 13%–14% dropout rate.
The fall prevention program was developed based on a guide to preventing falls in the elderly by the Ministry of Public Health of Thailand8, and the Otago Exercise Program.19 The program was validated in terms of content, activities, time, and arrangement by 3 experts consisting of a physician who is an expert in geriatric medicine, a physical therapist, and a community nurse who has experience in working with older adults. The fall prevention program included knowledge on daily self-care, fall prevention, exercises, nutrition, common diseases in the elderly, drug taking and management of a home and a safe environment for the older adults (Figure 1). The intervention program was implemented at the elderly school, and the participants in the intervention group were required to attend and train with the program 1 day a week for 6 consecutive weeks, 2 h per session. The control group did not receive any intervention during that period. They were instructed to pursue their habitual daily life activities.
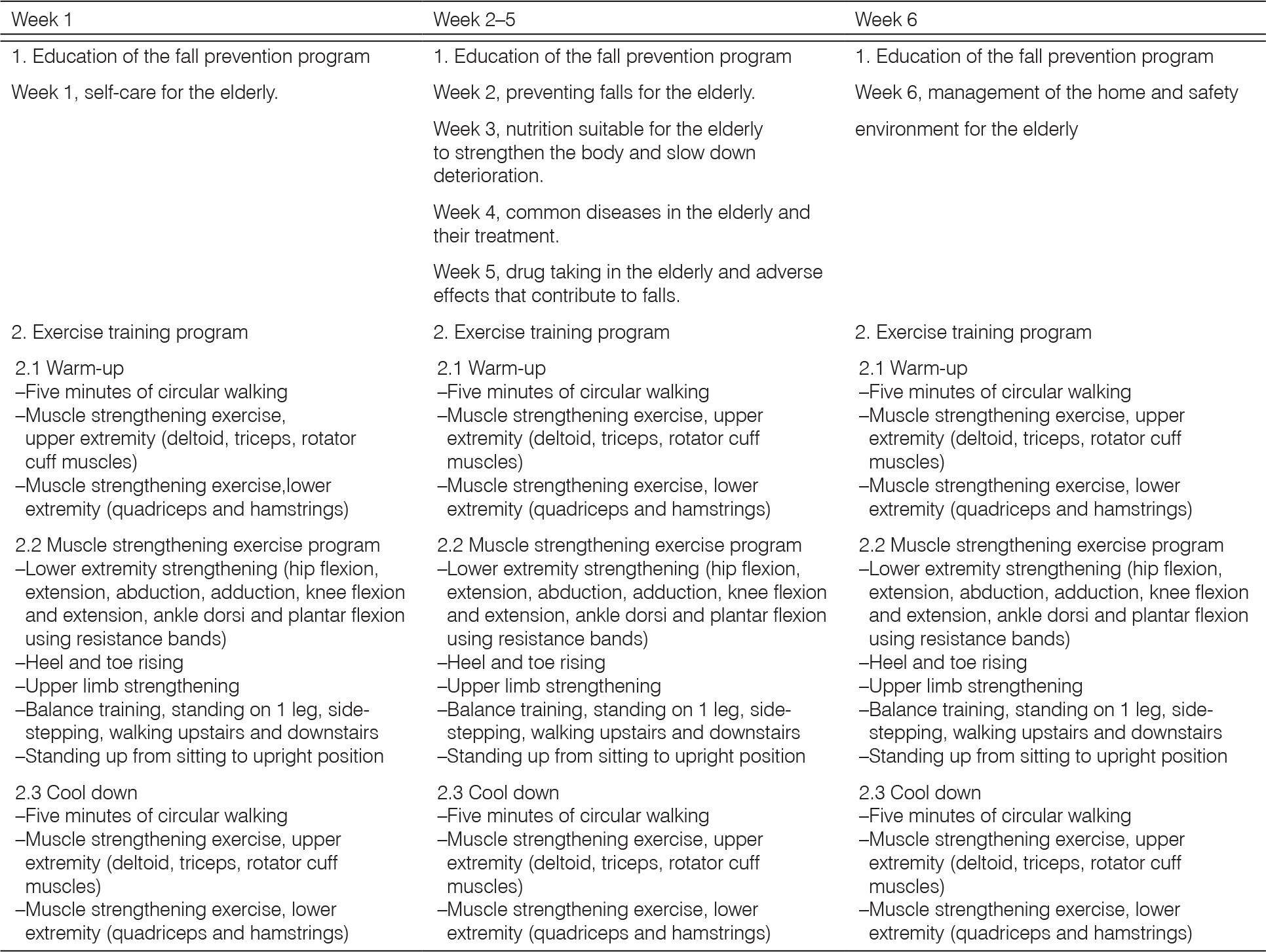
Fall prevention program.
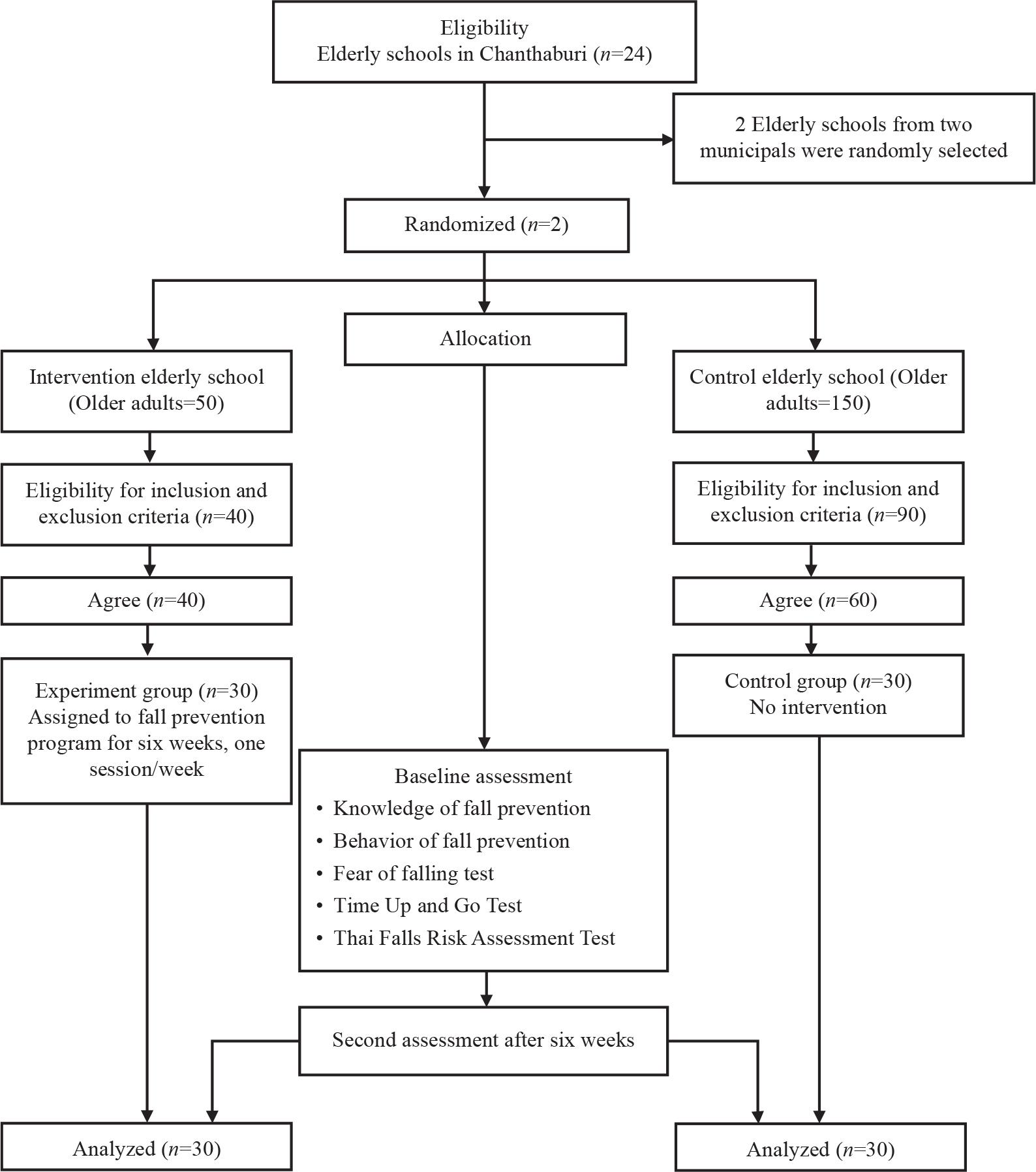
CONSORT study flow diagram.24
The demographic characteristic data were obtained from a questionnaire, such as age, gender, weight, height, and medications.
The knowledge of fall prevention data was obtained from 5-item questionnaires on gender and fall, elderly living alone and fall, visual acuity and fall, illness and fall, and medications and fall. The behavior of fall prevention data was obtained from 5-item questionnaires regarding visual acuity, vision problem correction, medications used for illness, consulting doctors for side effects of drugs and prevention of falls from slippery floors. The knowledge and behavior questionnaires were developed by the researchers. The higher the scores indicated good knowledge and behaviors in fall prevention. The content validity index of the questionnaire on knowledge was 0.88 and on behavior was 0.80 with the reliability was 0.90 and 0.74 respectively.
The Falls Efficacy Scale International (FES-I) and the Short Falls Efficacy Scale International (Short FES-I)20 are measures of “fear of falling” or, more properly, “concerns about falling,” which are suitable for use in research and clinical practice as recommended by the World Falls Guidelines. The Short FES-I was then developed by the team to allow the tool to be more applicable in clinical practice and to provide a shorter version for research. Short FES-I comprised 7 questions. The FES-I test had excellent reliability and was valid across different cultures and languages (Cronbach’s alpha = 0.96, ICC = 0.96).
Timed Up and Go Test (TUGT)21 was used to assess the fall risk and functional performance of the participants. The TUGT was a timed performance of getting up from a chair, walking 3 m, turning around, and walking back to sit down again. The cutoff point was 12 s based on the findings from the previous study. It had a high retest reliability in healthy older patients (ICC = 0.92) and high inter- and intra-rater reliabilities (ICC = 0.99 for both).
Thai Falls Risk Assessment Test (Thai-FRAT)22 was developed for the community-dwelling Thai elderly. It was a valid and reliable measure of fall risk. The newly developed Thai-FRAT was composed of 6 factors including “History of falls,” “Impaired body balance,” “Female,” “Specific medication use,” “Impaired visual acuity” and “Thai style house.” The possible score of the Thai-FRAT ranged from 0 to 11. The best cutoff score identified by the receiver operating curve analysis was 4. Sensitivity and specificity were 0.92 and 0.83, respectively. The Thai-FRAT could predict recurrent falls after 2 years among the elderly subjects who had a history of falls during the past 6 months in the second set of population. An association between the Thai-FRAT score and mortality was also shown.
Primary outcomes were assessed to evaluate the effectiveness of the fall intervention program which included knowledge of fall prevention, behavior for fall prevention, fear of falling, TUGT and the Thai-FRAT. At baseline before the intervention, participants were assessed for outcome measures and demographic characteristics, comorbid medical conditions and prior history of falls and fall-related injuries during the past year. After the 6 weeks of the fall intervention program, participants in both groups were assessed for outcome measures.
Descriptive and inferential statistical analyses were performed using the statistics software package.23 The Shapiro–Wilk test was used to check normality for continuous data. Independent t-tests were used for the homogeneity test of the participants’ characteristics and the outcome measures between the 2 groups. The comparison of all outcomes at the baseline and the 6 weeks after intervention in each group was carried out using paired sample t-tests. The P-value was deemed statistically significant at 0.05 (2-tailed).
All participants provided their written informed consent to participate in this study. The study was conducted following the Declaration of Helsinki, and the protocol was approved by Research and Development Institute, Rambhai Barni Rajabhat University, Thailand (permit number IRB 14/2567).
The total number of participants was 60 (intervention group 30 and control group 30) at the baseline and at the second assessment. Results of the Shapiro–Wilk tests showed normality distributions of the data for both groups. There was no statistically significant difference between the 2 groups regarding age (P = 0.630), body mass index (P = 0.613), average number of comorbidities (P = 0.832) and number of medication use (P = 0.149) (Table 1).
Baseline characteristics and differences between the groups, n (%).
| Characteristics | Experimental group (n = 30) | Control group (n = 30) | Mean ± SD | P-value |
|---|---|---|---|---|
| Gender (m/f) | 4 (13.33)/26 (86.67) | 6 (20.00)/24 (80.00) | ||
| Age (years) | E: 70.80 ± 7.00; C: 70.00 ± 5.67 | 0.630 | ||
| 60–69 | 12 (40.00) | 13 (43.33) | ||
| 70–79 | 13 (43.33) | 14 (46.67) | ||
| >80 | 5 (16.67) | 3 (10.00) | ||
| Body mass index (kg/m2)* | E: 24.7 ± 4.7; C: 24.1 ± 4.5 | 0.613 | ||
| Underweight <18.5 | 7 (23.33) | 3 (10.00) | ||
| Normal weight 18.5–22.9 | 9 (30.00) | 12 (40.00) | ||
| Overweight 23.0–27.5 | 14 (40.00) | 11 (36.67) | ||
| Obese >27.5 | 2 (6.67) | 4 (13.33) | ||
| Number of comorbidities | E: 1.4 ± 1.0; C: 1.4 ± 1.3 | 0.832 | ||
| Number of medication use | E: 1.9 ± 1.8; C: 1.2 ± 1.8 | 0.149 |
Note: Analyzed by independent sample t-test; E, Experimental group; C, Control group; SD, standard deviation;
Asian body mass index.25
Paired sample t-tests were conducted to compare the outcome variables in the experimental group and control group before and after the fall prevention program. In the experimental group, significant improvements were observed in fall prevention knowledge (P < 0.001), fall prevention behavior (P < 0.001), FES-I scores (P < 0.05), TUGT performance (P < 0.001), and Thai-FRAT scores (P < 0.001). However, no statistically significant changes were found in the control group (Table 2).
Pre-post differences for each examined variable.
| Variables | Group | Mean pre (SD) | Mean post (SD) | Mean difference | 95% CI | t | P-value |
|---|---|---|---|---|---|---|---|
| Knowledge | Experimental | 3.83 (0.74) | 4.83 (0.37) | –1.00 | –1.25, –0.74 | –7.88 | <0.001 |
| Control | 3.06 (1.38) | 3.16 (1.48) | –0.10 | –0.75, 0.55 | 0.31 | 0.756 | |
| Behavior | Experimental | 1.79 (0.38) | 2.67 (0.30) | –0.88 | –1.08, –0.67 | –8.97 | <0.001 |
| Control | 2.25 (0.45) | 2.09 (0.61) | 0.16 | –1.07, 0.42 | 1.22 | 0.230 | |
| FES-I | Experimental | 2.43 (0.85) | 1.74 (0.66) | 0.45 | 0.08, 0.83 | 2.50 | <0.05 |
| Control | 2.31 (0.95) | 2.70 (0.87) | –0.38 | –0.79, 0.02 | –1.93 | 0.063 | |
| TUGT | Experimental | 10.82 (1.90) | 9.04 (2.09) | 1.78 | 1.37, 2.18 | 8.88 | <0.001 |
| Control | 11.03 (1.59) | 11.06 (0.90) | –0.03 | –0.57, 0.51 | –0.11 | 0.912 | |
| Thai-FRAT | Experimental | 3.13 (1.87) | 2.43 (1.45) | 0.50 | 0.20, 0.79 | 3.52 | 0.001 |
| Control | 4.76 (2.26) | 4.53 (2.45) | 0.23 | –0.03, 0.50 | 1.75 | 0.090 |
Note: Statistically significant at α < 0.05 with paired sample t-test; FES-I, Falls Efficacy Scale International; Thai-FRAT Thai Falls Risk Assessment Test; SD, standard deviation; TUGT, Timed Up and Go Test.
Independent sample t-tests showed that all outcome variables significantly changed from the baseline to the end of the intervention in the experimental and control groups (P < 0.001) (Table 3).
Results from the comparison of fall prevention programs between experimental and control groups, (post-test).
| Variables | Group | Mean (SD) | Mean difference | 95% CI | t | P-value |
|---|---|---|---|---|---|---|
| Knowledge | Experimental | 4.83 (0.37) | 1.66 | 1.09, 2.23 | 5.94 | <0.001 |
| Control | 3.16 (1.48) | |||||
| Behavior | Experimental | 2.67 (0.30) | 0.58 | 0.32, 0.83 | 4.63 | <0.001 |
| Control | 2.09 (0.61) | |||||
| FES-I | Experimental | 1.74 (0.66) | 0.95 | –1.35, –0.54 | –4.72 | <0.001 |
| Control | 2.70 (0.87) | |||||
| TUGT | Experimental | 9.04 (2.09) | –2.02 | –2.87, –1.18 | –4.85 | <0.001 |
| Control | 11.06 (0.90) | |||||
| Thai-FRAT | Experimental | 2.43 (1.45) | –2.10 | –3.14, –1.05 | –4.02 | <0.001 |
| Control | 4.53 (2.45) |
Note: Statistically significant at α
The study aimed to determine the effects of the fall prevention program for the older adults living in the community in Chanthaburi province. Participants were the older adults attending the elderly schools, which were randomly assigned to the experimental and control groups, 30 participants in each group (n = 30). The experimental group received a 6-week fall prevention program, while the control group received no intervention. The study was conducted as a single-blind trial.
The study found that the average outcomes after implementing the fall prevention program for the elderly people in the community between the experimental group and the control group were statistically significantly different. The older adults in the experimental group who received the fall prevention program had increased knowledge of fall prevention, improved fall prevention behaviors, reduced fear or concern about falling, developed better walking and balance and significantly reduced risk of falling (P < 0.001).
The results demonstrated that providing knowledge of fall prevention to the older adults helped raise their awareness and emphasize the importance of fall prevention, leading to more cautious and preventive behaviors regarding falls. In this research, the fall prevention program for the older adults involved activities that were held once a week, 2 h each time, for over a consecutive 6-week period. In week 1, knowledge on self-care for the older adults was provided along with exercises to strengthen arm and leg muscles, standing, walking, and balance training. In week 2, knowledge of fall prevention was given along with exercise training. In week 3, knowledge of appropriate nutrition for older adults was taught along with exercises. In week 4, knowledge of common diseases in older adults was provided along with exercises. In week 5, knowledge on medication use in older adults was imparted along with exercises. Finally, in week 6, knowledge of home and environmental safety arrangements was provided alongside exercise training. This aligned with previous research showing that falls in older adults were influenced by several factors, including lack of exercise, illness, environmental conditions, social factors, and individual factors.26 Providing fall prevention knowledge could increase knowledge levels and promote fall-preventive behaviors.27 Individual older adults in the community who received this knowledge exhibited better fall prevention behaviors than the control group.28 Moreover, the individual older adults who took multiple medications or regularly used even a single antipsychotic drug had 1.2 times higher risk of falling.29
In part of the fear of falling in older adults, the individual older adults who received knowledge of fall prevention, along with engaging in exercises to strengthen arm and leg muscles, as well as muscles for standing, walking, and balance, increased their self-confidence. This allowed them to perform daily activities independently and reduced their fear of falling. This was consistent with research showing that continuous exercise increased muscle strength, which helped reduce fear and lower the risk of falls among high-risk elderly groups.30
Older adults who engage in continuous exercise will experience improvement in walking and balance. The exercise program for the older adults in this study was adapted from the Otago Exercise Program, which included 10 exercises aiming at improving joint flexibility, muscle strength, walking, and balance.19,31,32 Continuous exercise helps individual older adults improve their walking and balance. Each older adult in the community has different physical conditions, so their exercise methods vary accordingly.33 Elderly individuals who participated in programs such as multi-system physical exercises (MPE),34 Multidimensional Exercises,35 or exercises that enhanced leg muscle strength (Strengthening exercises) combined with balance and walking training, showed improvement in balance, reduced risk of falls, and decreased fear of falling.36,37 Exercises also stimulated sensory perception and motor control in the older adults.38,39
The older adults who received knowledge of fall prevention along with continuous exercise would experience an increase in strength and a decrease in the risk of falling. This aligns with studies on patients who had experienced hip fractures due to falls. After participating in an 8-week exercise program, the older adults showed improved Thai-FRAT scores compared to before participating in the program.40
The limitation of this study was it needed to be continuously monitored over 6 weeks to evaluate the fall risk among the older adults living in the community. In addition, this trial was conducted with the older adults who were social-bound at the elderly schools, thereby the results of this study may limit the generalization to other groups.
The results of this study were consistent with previous research. The fall prevention program for the older adults dwelling in the community in Chanthaburi province proved effective in increasing knowledge and promoting fall prevention behaviors. It reduced their fear of falling, improved their walking and balance, and decreased their risk of falls. This program had 2 advantages: raising awareness of fall risks and promoting exercise. As a result, it led to an improvement in the quality of life for the older adults in the community.