Nurses play a very important role in a society with an aging population, such as in the rehabilitation of stroke patients. Stroke is a leading cause of early mortality among neurological diseases. Disruption of blood flow to the brain leads to brain cell damage, impacting cognitive function. Consequently, cognitive impairment is a common complication following a stroke.1,2 Poststroke cognitive impairment refers to the cognitive impairment of patients after stroke, including but not limited to memory decline, inattention, impaired executive function, speech disorders, etc.3,4 This can significantly impact quality of life and increase the risk of depression, underscoring the importance of poststroke rehabilitation.3–5 The current clinical treatment and nursing strategies often fail to meet expectations, and they mainly focus on primary treatments, including drug therapy, rehabilitation training, and psychological intervention.
CiteSpace, a Java-based application, analyzes and visualizes research hotspots and frontiers in scientific literature using econometrics, co-occurrence analysis, and cluster analysis. The volume of published papers can reflect the developmental progress and trends within a specific research field.6 Bibliometric analysis serves as a methodology for studying scientific development, and it can conduct quantitative and qualitative analysis on the research performance of individual researchers, institutions, countries, journals, or disciplines.7,8 Emergence analysis looks for literature that suddenly receives a lot of attention during a certain period of time,9 with the appearance and disappearance of literature exhibiting high emergence intensity reflecting the transition of academics from 1 research topic to another. In recent years, there has been a proliferation of research results based on prestroke and poststroke cognitive reserve training in interventions for the prevention and rehabilitation of cognitive impairment. Utilizing the Web of Science Core Collection database, this study employs CiteSpace 6.3.R1(64-bit) as the primary analytical tool. This study analyzes the advances, trends, and gaps in the application of cognitive reserve for treating stroke-induced cognitive impairment. Suggestions from the author are presented to help us better understand the effect and prevention of cognitive reserve on poststroke cognitive impairment.
A search was conducted in the Web of Science Core Collection database to obtain the literature on cognitive reserve and stroke cognitive impairment from 1 January 2010, to 1 January 2024. Table 1 shows the literature retrieval style.
Literature retrieval strategies.
| Steps | Strategies |
|---|---|
| #1 | TS = (“stroke” OR “apoplexy” OR “cerebrovascular accident” OR “cerebral hem OR rhage” OR “cerebral thrombosis”) |
| #2 | TS = (“cognitive function” OR “cognitive dysfunction” OR “cognitive impairment” OR “cognitive decline” OR “cognitive dis OR der” OR “cognitive deficit” |
| #3 | TS = (“cognitive reserve”) |
| #4 | #1 DNA #2 AND #3 |
After a preliminary data search, 1246 articles were obtained, all of which were individually screened by 2 researchers to ensure that they were relevant to the topic of the article. Researchers conducted the analysis and finally obtained 860 literatures. The final results were exported in “plain text” format, the record contents were selected as “Full record and reference,” and the download_*.txt format is stored.
Initially, the obtained literature and its citation information were imported into the Citespace 6.3.R1(64-bit) software9 for analyzing distribution across countries, institutions, literatures, keywords, journals, and authors.9 (The analysis period was set from January 2010 to January 2024, with annual time slices and the top 50 records per slice. The G-index was set at 25, and the pruning method used was the path-finding algorithm.) Other parameters remained default for co-cited literature analysis, including centrality, citation frequency, cluster analysis, and emergence analysis of co-cited literature. Centrality assesses the significance of a paper. High centrality signifies that the literature is not only frequently cited but also plays a pivotal role in the evolution of various research topics. Cluster analysis of co-cited literature was carried out by using the citation relationship among literatures to explore high-impact literature and important research topics in the field of cerebral stroke cognitive impairment rehabilitation, and a cluster map of co-cited literature was drawn at the same time. (Cluster labeling involves grouping closely related literature keywords and calculating the weight value of each keyword. The keyword with the highest weight value within a cluster is selected as the category representative and serves as the cluster label). The module value (Q value) and the average contour value (S value) in the clustering map serve as benchmarks for assessing map clarity. A Q value exceeding 0.3 indicates a sound clustering structure. An S value ranging from 0.5 to 0.7 signifies reasonable cluster analysis results, while an S value surpassing 0.7 indicates compelling outcomes. The emergence analysis identifies key literature within a time frame, with higher intensity indicating greater attention during that period.
The publication volume over various periods reflects the popularity and developmental trends within a specific research domain. Following the defined retrieval strategy and screening process, 860 articles related to the application of cognitive reserve in the rehabilitation of cerebral stroke cognitive impairment were collected in this paper. Excluding 2 papers published in January 2024, 858 papers were retained. As shown in Figure 1, the publication frequency in this domain has been relatively unstable, and it can be seen that stroke prevention and treatment represent a global challenge. However, from 2021 to 2023, an upward trend in publications suggests growing research interest in this area.
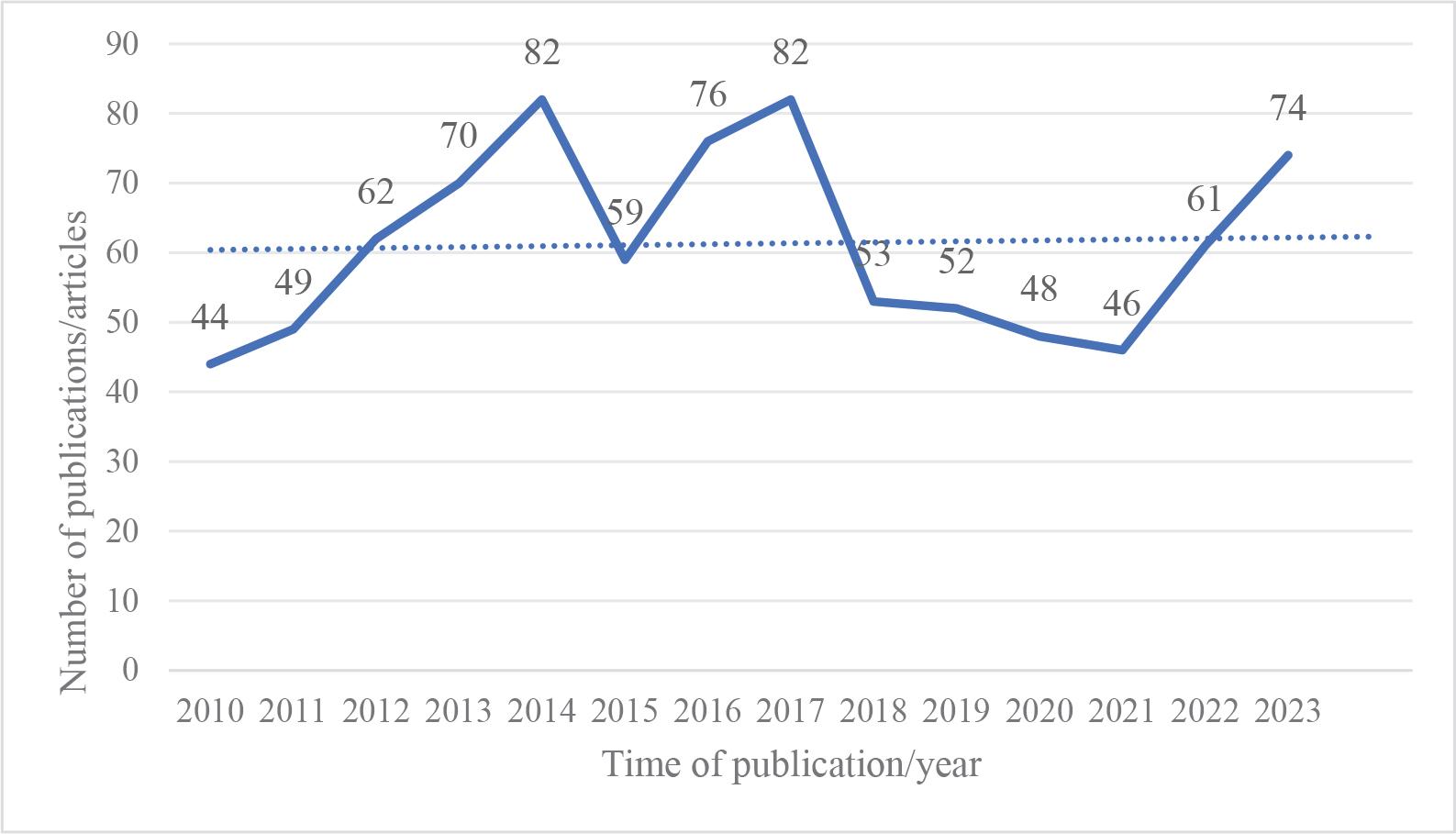
The application of cognitive reserve in stroke cognitive impairment (Web of Science database).
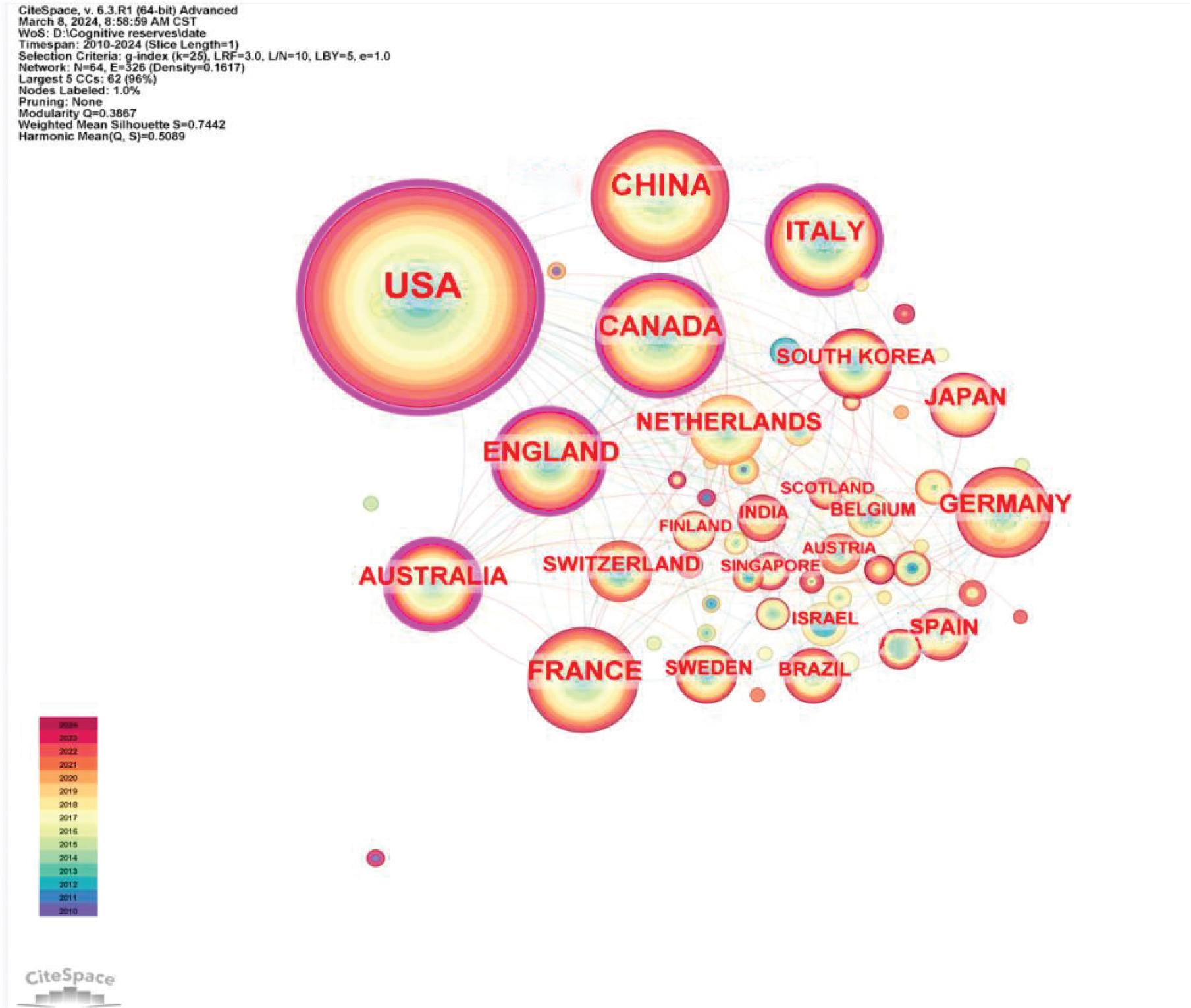
The application of cognitive reserve in stroke cognitive impairment.
Note: N = 54 (involving 54 countries), E = 326 (326 lines, representing the relationship between countries), Q = 0.3867 (>0.3), and S = 0.7442 (>0.7), which means that the distribution credibility is convincing. Larger node circles indicate a higher volume of research output from more countries. More lines signify increased co-authorship frequency among countries, indicating closer collaboration.
Analysis using CiteSpace 6.3.R1(64-bit) software revealed that the 5 leading countries by publication volume are the United States, China, Canada, Italy, and the United Kingdom. These countries are foremost in research output in the field of applied research on cognitive reserve and stroke cognitive impairment.
FRONT NEUROL’s total citation frequency was 18.76, highlighting its significant focus on the application of cognitive reserve in the study of cognitive impairment in stroke, and has sustained interest in pertinent topics from 2018 to the present. See Figure 3.
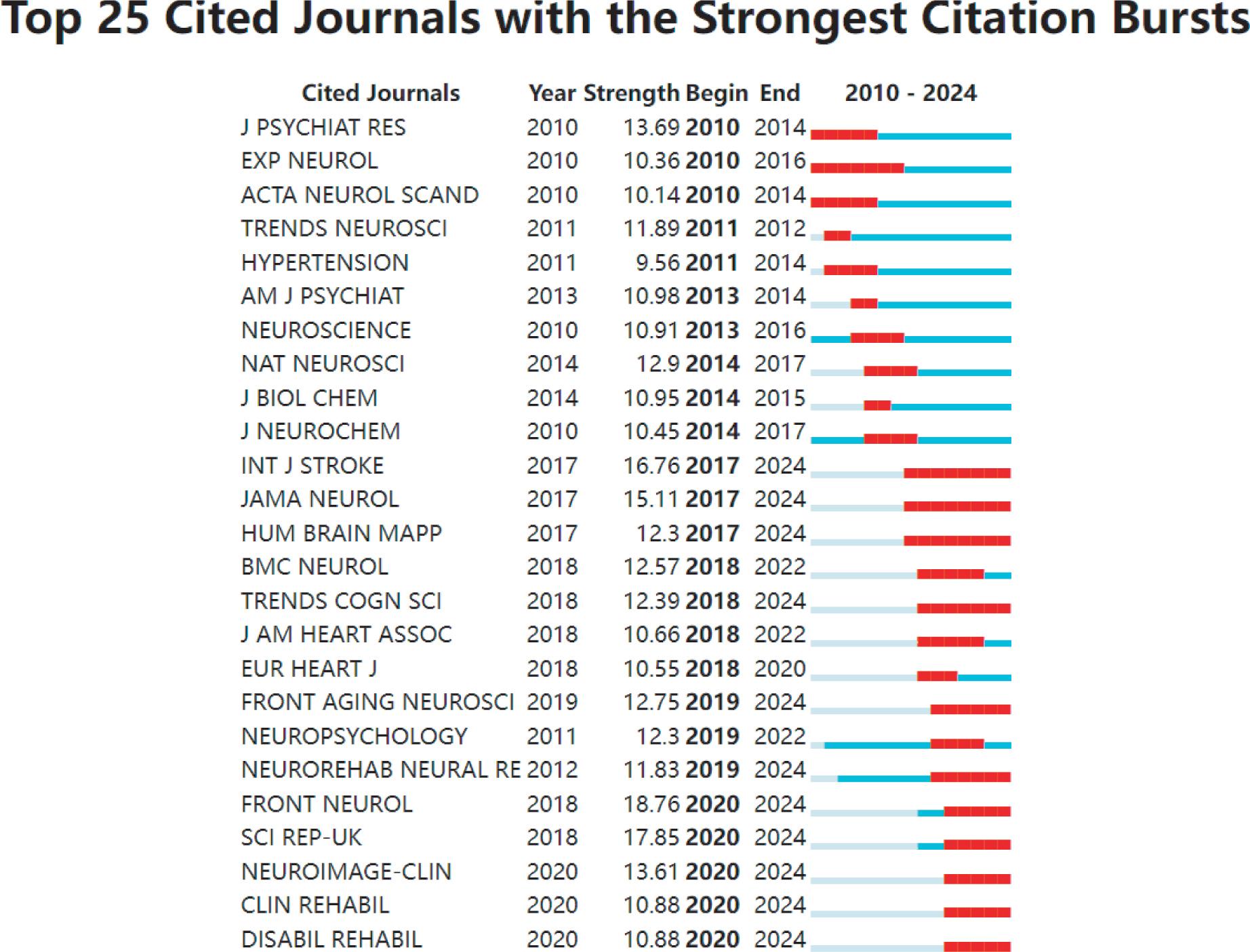
Distribution of co-cited journals in the application of cognitive reserve in stroke cognitive impairment (Web of Sciences Database).
Note: A “burst journal” refers to a journal that experiences a sudden surge in citations within a specific timeframe. The chart displays the top 25 journals with citation bursts, based on an analysis of 860 articles published between January 2010 and January 2024. The red squares represent the Year in which the burst occurred; “Year” represents the earliest year in which the cited journal article appeared. “Strength” indicates the citation frequency. “Begin” and “End” correspond to the start and conclusion of the citation burst, respectively.
The CiteSpace 6.3.R1(64-bit) software facilitated keyword co-occurrence, clustering, and burst analysis of the 860 articles. Excluding the query keyword “stroke,” keyword co-occurrence analysis revealed that the 3 most frequent keywords were “Alzheimer’s disease,” “cognitive impairment,” and “risk factors,” respectively (Figure 4). The cluster analysis yielded 6 keyword clusters: #1 vascular dementia, #2 oxidative stress, #3 cerebral palsy, #4 executive functions, #5 cognitive reserve, and #6 Montreal Cognitive Assessment. Consequently, this study identifies the research direction of the application of cognitive reserve in stroke cognitive impairment: brain-related diseases, executive ability, cognitive reserve, and cognitive assessment (Figure 5). Keyword burst analysis indicates that the primary research hotspots in this field are “reserve,” “education,” and “cognitive reserve impact recovery” (Figure 6).
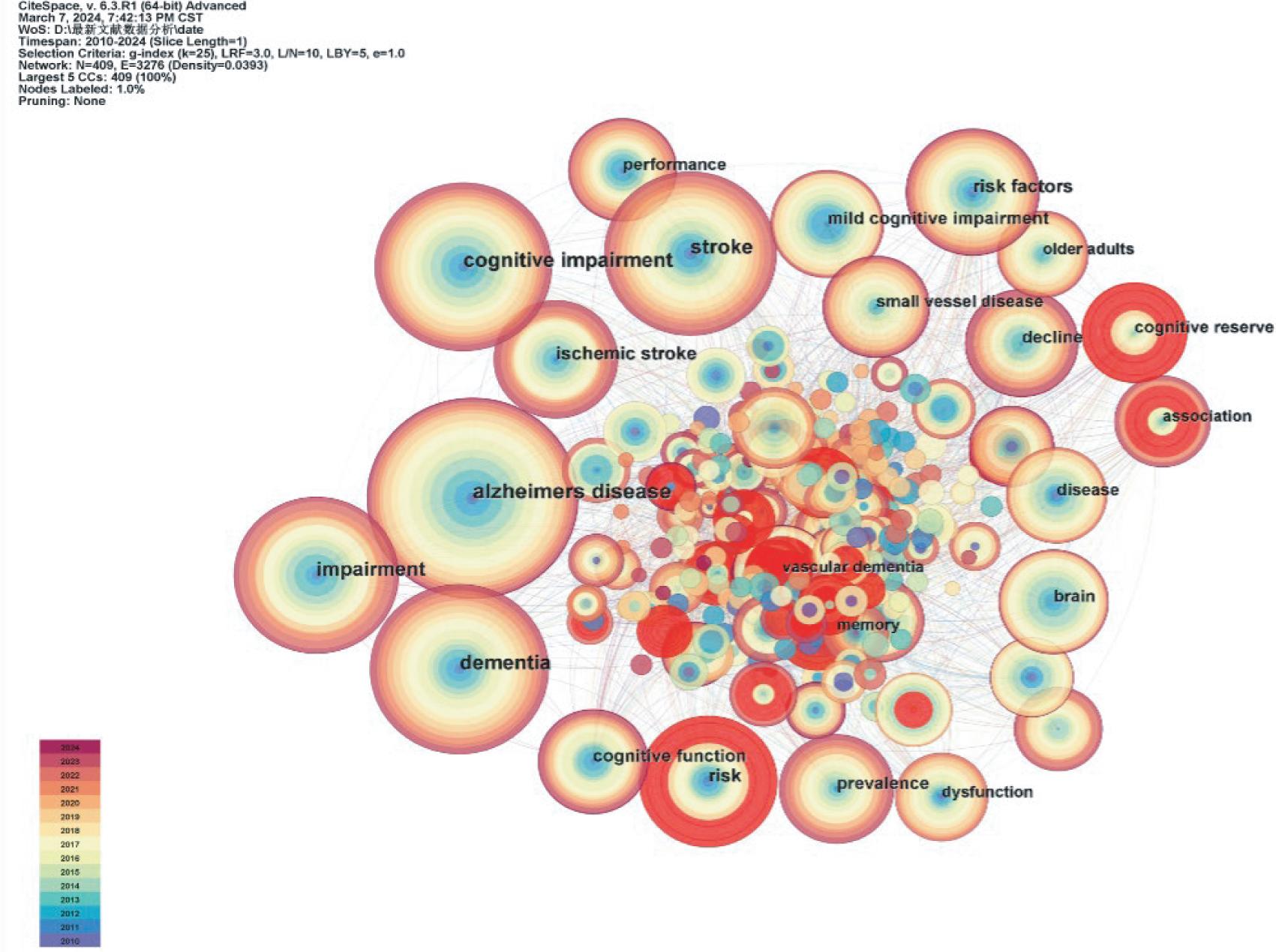
Co-occurrence distribution of keywords in the application of cognitive reserve in stroke cognitive impairment (Web of Sciences Database).
Note: In the keyword co-occurrence graph, the node size corresponds to the frequency of keyword occurrence, which is the research hot word in this field and also the research direction.
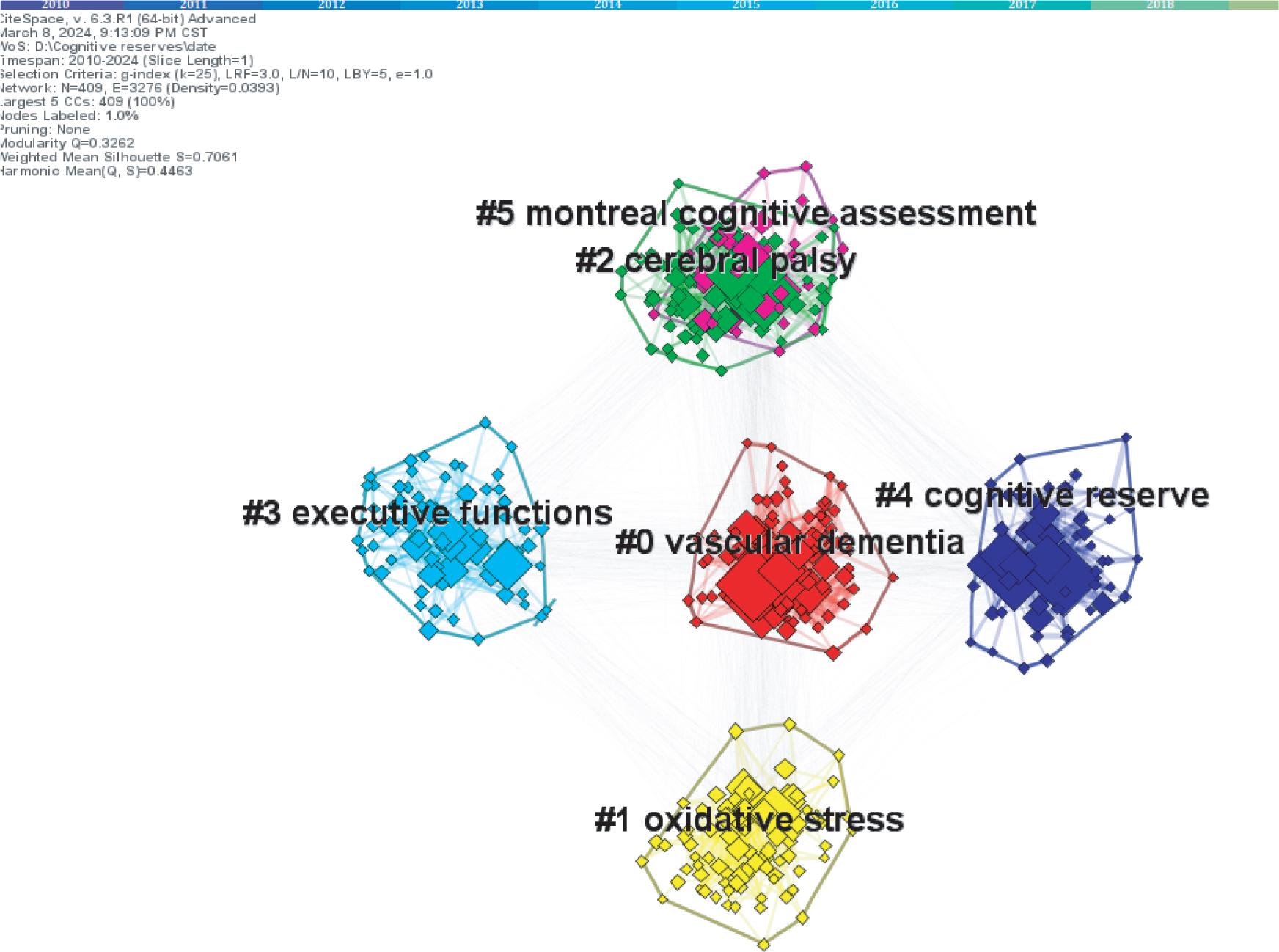
Application of cognitive reserve in cognitive impairment in stroke (Web of Sciences Database).
Note: In the keyword cluster network diagram, larger nodes indicate a greater number of published articles, red, yellow, green, light blue, dark blue, red represent 6 different clusters (divided into #0 vascular dementia; #1 Oxidative stress; #2 Cerebral paralysis; #3 Execution ability; #4 Cognitive reserve; and #5 Montreal cognitive assessment), and thicker lines denote a higher correlation between keywords. Q = 0.3262, (>0.3), S = 0.7061 (>0.7), and clustering is efficient and convincing.
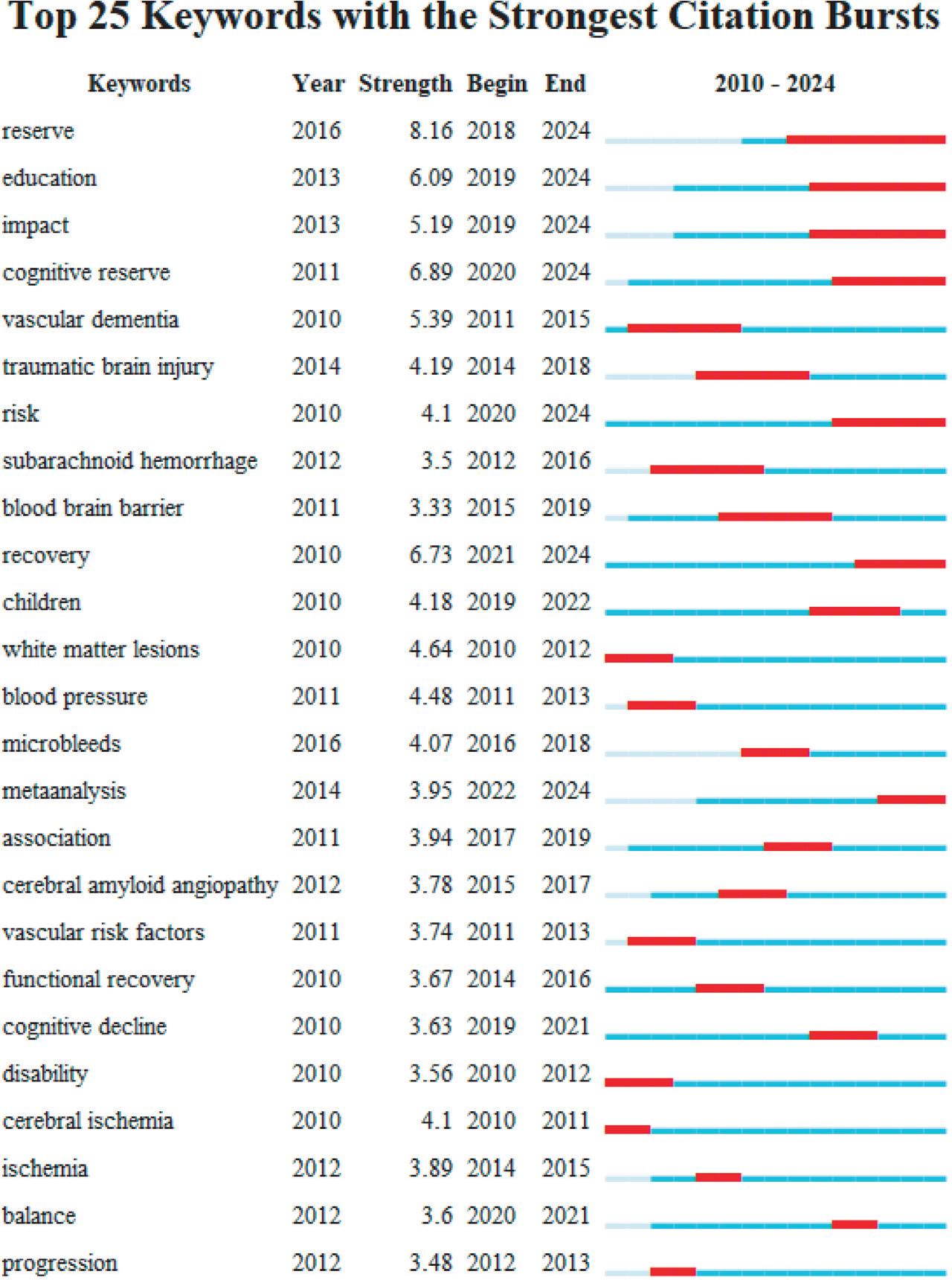
The application of cognitive reserve in cognitive impairment in stroke: keyword outbreak distribution map (Web of Sciences Database).
Note: Keyword burst analysis chart. “Keywords” represents the outburst keywords (the top 5 are as follows: in order, (reserve, education, cognitive reserve, influencing factors, and rehabilitation); the red squares represent the year in which the outbreak occurred, “year” represents the earliest year in which the keyword appeared, “Strength” represents the frequency of occurrence, and “Begin” and “End” represent the beginning and end of the keyword outbreak, respectively.
A total of 18 clusters were obtained through literature co-citation clustering and emergence analysis. Based on neutral line density and timing, 15 clusters were identified as the most significant clusters in the literature cocitation network (see Figure 7).
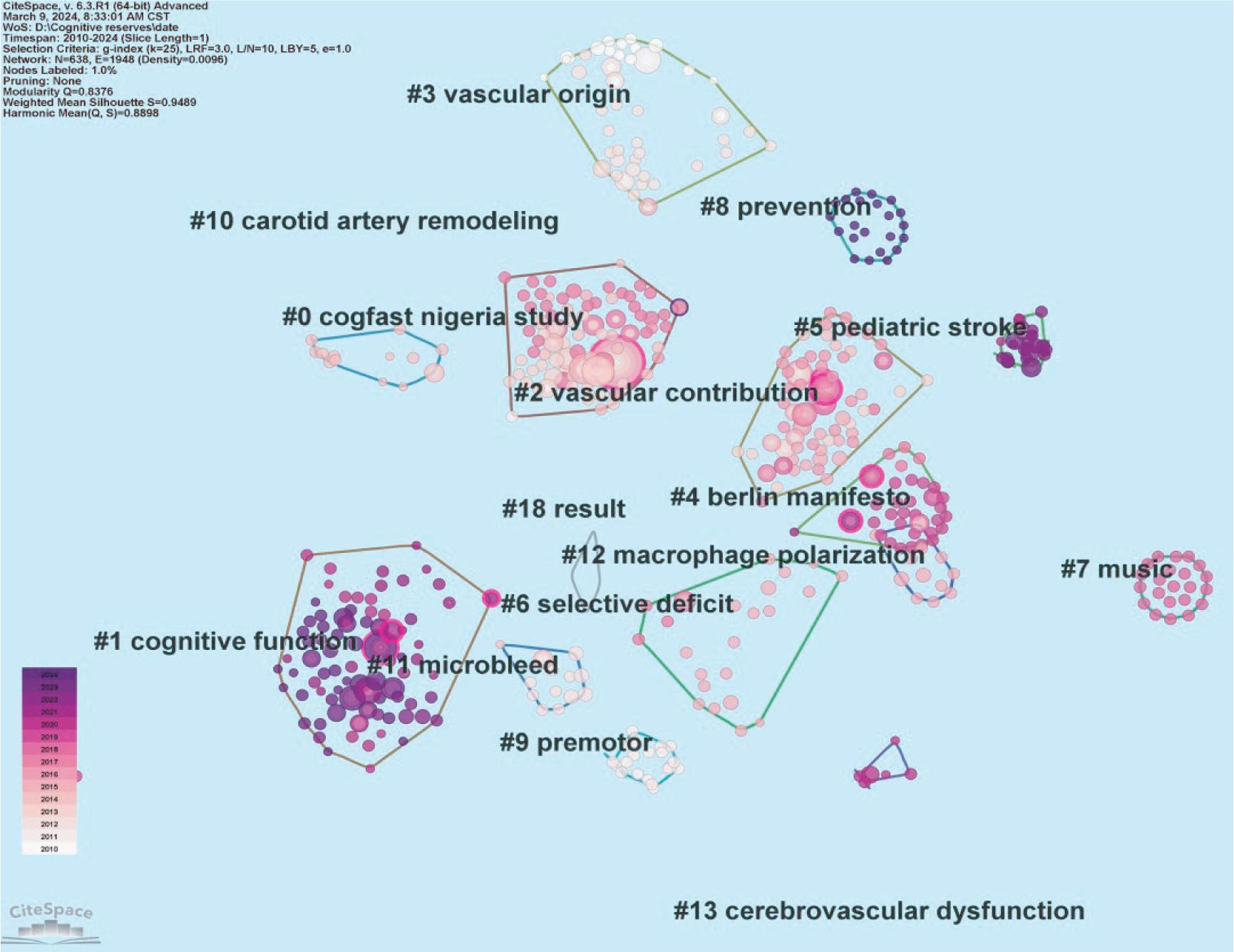
Distribution of co-cited literature on the application of cognitive reserve in stroke cognitive impairment (Web of Sciences Database).
Note: In the literature co-citation cluster graph, the color of the cluster represents the year in which the co-citation relationship first appeared in the cluster, the size of the node represents the citation frequency of the literature, and the color of the connection represents the time of the first citation. The clusters in the figure are as follows: #0 CogFAST Nigeria study, #1 cognitive function, #2 vascular contribution, #3 vascular origin #4 berlin manifesto, #5 pediatric stroke, #6 selective deficit, #7 music, #8 prevention, #9 premotor, # 10 carotid artery remodeling, #11 microbleed, #12 carotid artery resection polarization, #13 cerebrovascular dysfunction, #18 result, and cerebrovascular dysfunction. In the recent 5 years (2020–2024), literature clustering in the common citation map of research hotspots is as follows: #1 cognitive function, #5 pediatric stroke, #8 prevention, #11 microbleed, and #12 macrophage polarization. Q = 0.8376 (>0.3), S = 0.9489 (>0.7, close to 1), and clustering was efficient and feasible.
An in-depth analysis of the literature with high co-citations was conducted. The CiteSpace 6.3.R1(64-bit) software was utilized for the co-citation analysis of cognitive reserve in the application field of stroke cognitive impairment from January 2010 to January 2024, focusing on the literature with the top 10 co-citations. The results are shown in Figure 8 and Table 2. These seminal articles, due to their significant academic impact, mirror the research trends and emerging areas in the field, providing crucial insights for further studies. Gorelick,10 with a total of 33 citations, ranked the top cited literature. This paper reviews published studies on the role of blood vessels in cognitive impairment and dementia, including changes in internal physiological mechanisms, external risk factors, and potential prevention and therapeutic strategies. It found that with global aging, the incidence of cognitive impairment and dementia is rising annually. However, by mitigating related risk factors and enhancing preventive measures, the disease rate has significantly decreased. The high degree of co-citation for this article indicates the widespread scholarly recognition of the importance of preventing cognitive impairment and understanding its influencing factors. Meanwhile, Stern et al.,11 Wardlaw et al.,12 Umarova et al.,13 Shin et al.,14 Rosenich et al.,15 Uniarova16 all analyzed cognitively related risk factors before cognitive impairment and found appropriate prevention methods in advance. The main contents of the research include brain cognitive reserve, individualized rehabilitation strategies after cognitive impairment, and protective factors of cognitive impairment, which prove the dominance of cognitive reserve in cognitive impairment rehabilitation from different angles.
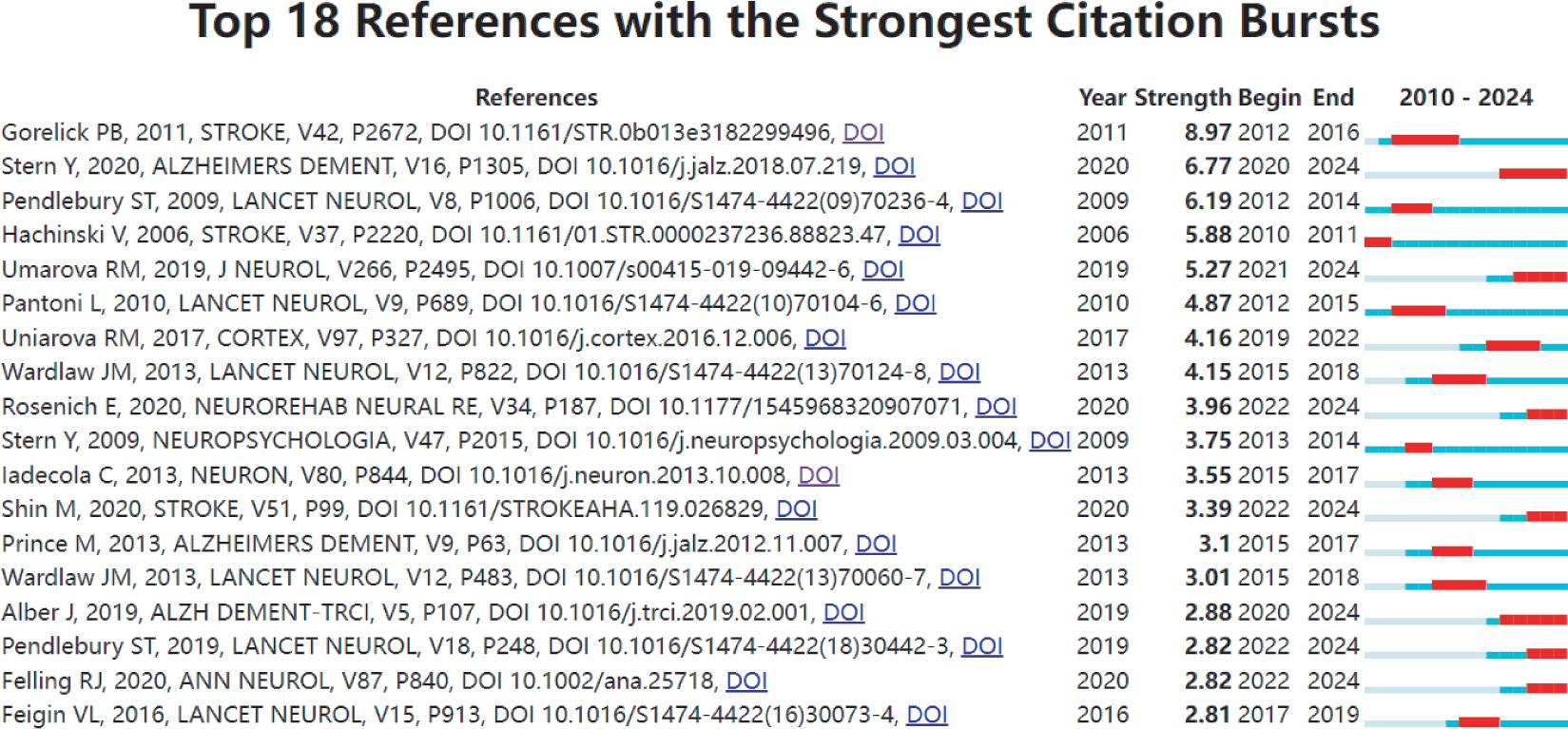
The application of cognitive reserve in cognitive impairment in stroke (Web of Sciences Database).
Note: Analysis of Emerging Co-cited References. Red squares indicate the years of significant citation spikes, “Year” denotes the initial appearance of the citation, “Strength” signifies the occurrence frequency, while “Begin” and “End” mark the start and conclusion of the citation surge, respectively.
Top 10 most-cited articles on the application of cognitive Reserve in stroke cognitive impairment (Web of Sciences Database).
| Author/year of publication | Centrality | Research results | Theme | Quote |
|---|---|---|---|---|
| Gorelick et al.10 | 0.28 | Vascular contributions to cognitive impairment and dementia are important. | Definitions of vascular cognitive impairment neuropathology, basic science, and pathophysiological aspects, role of neuroimaging and vascular and other associated risk factors, and potential opportunities for prevention and treatment are reviewed. | 33 |
| Stern et al.11 | 0.13 | Reserve, Resilience, and Protective Factors resilient against aging or disease are important | Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance | 14 |
| Pendlebury and Rothwell17 | 0.05 | The likely effect of optimum acute stroke care and secondary prevention in reducing the burden of dementia. | Assess the heterogeneity in the reported rates and identify risk factors for prestroke and poststroke dementia. | 14 |
| Pantoni18 | 0.03 | Small vessel disease should be a main target for preventive and treatment strategies, but all types of presentation and complications should be taken into account. | Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges | 14 |
| Wardlaw et al.12 | 0.24 | Completed a structured process to develop definitions and imaging standards for markers and consequences of Cerebral small vessel disease | Neuroimaging standards for research into small vessel disease and its contribution to aging and neurodegeneration | 11 |
| Umarova et al.13 | 0.01 | Cognitive reserve contributes to inter-individual variability in the initial severity of cognitive deficits and disability in acute stroke, and may suggest individualized rehabilitation strategies. | Cognitive reserve impacts on disability and cognitive deficits in acute stroke. | 10 |
| Hachinski et al.19 | 0 | Using the same standards will help identify individuals in the early stages of cognitive impairment, and will make studies comparable. | Vascular cognitive impairment harmonization standards. | 10 |
| Shin et al.14 | 0.06 | Education and occupation can buffer an individual against cognitive impairment caused by stroke and promote rapid cognitive recovery early after stroke. | Effect of cognitive reserve on risk of cognitive impairment and recovery after stroke | 9 |
| Uniarova16 | 0 | This alternative view of how neglect and other cognitive deficits occur and recover promotes discussion about plasticity and recovery to a general rather than a single stroke-based domain, providing more efficiency in recovery research. | Discussed how individual susceptibility to stroke lesion might explain the reported discrepancies in lesion anatomy, non-spatial deficits, and recovery courses. | 9 |
| Rosenich et al.15 | 0.01 | Clinicians and researchers to better consider the role of premorbid factors in the stroke, lifestyle-related variables, such as cognitive reserve, in facilitating successful neurological outcomes and recovery following stroke. | The potential significance of cognitive reserve in the context of stroke, | 8 |
Additional highly cited literature includes clinical studies focusing on the pathogenesis and clinical characteristics of vascular cognitive impairment, along with the relationship between the prevalence and incidence of cognitive impairment in relation to vascular disease onset. Through this research, criteria for the diagnosis of related diseases have been established.17–19
Cognitive Impairment Rehabilitation: An analysis conducted with CiteSpace 6.3.R1 (64-bit) software demonstrates that the United States and China are at the forefront of research in cognitive impairment and dementia rehabilitation, with the United States taking the lead. Journals such as Frontiers in Neurology, Scientific Reports, International Journal of Stroke, JAMA Neurology, Journal of Psychiatric Research, and NeuroImage: Clinical, indexed in the Web of Science database, serve as authoritative resources for applying cognitive reserve to stroke cognitive impairment rehabilitation. Research published in these journals primarily focuses on neurology, cerebral stroke rehabilitation, cardiac rehabilitation, psychiatry, and neuroimaging.
Co-cited cluster analysis in the field of cognitive reserve application for stroke-induced cognitive impairment revealed 18 clusters, with 10 being notably significant: cognitive function, the role of blood vessels, vascular obstruction, the Berlin Declaration, childhood stroke, selection deficit, music, prevention, microvascular bleeding, and tissue repair. Cognitive function is identified as the primary research focus in the application of cognitive reserve to stroke patients with cognitive impairment, a finding supported by keyword, literature co-citation, and hotspot analysis of highly cocited literature. The emergence of childhood stroke as a cluster of interest highlights a future research direction. While current studies predominantly focus on the elderly due to higher incidence rates, clustering analysis of highly co-cited literature suggests a shift toward younger populations, emphasizing the importance of the focus on cognitive impairment rehabilitation in children poststroke.20,21 Moreover, prevention emerges as a significant cluster in highly co-cited literature analysis, suggesting that research in cognitive impairment rehabilitation should prioritize preventive strategies to mitigate cognitive impairment’s impact at its source, meeting clinical patients’ needs for more efficient and high-quality treatment.
Keyword co-occurrence analysis, excluding terms akin to the search query, identified primary keywords including dementia, cognitive impact, and risk factors. Keyword cluster analysis grouped these keywords into 6 main clusters: vascular dementia, oxidative stress risk factors, brain paralysis, executive function, cognitive reserve, and Montreal cognitive assessment. The predominant research focus in this field is vascular dementia, which aligns with the hot analysis results of highly cited literature. Keyword burst analysis indicated that reserve, education, and cognitive recovery aligned with the directions of the last 2 clusters in keyword cluster analysis. Education, cognitive stimulation, and cognitive assessment have emerged as new research hotspots. The author’s discussion, informed by visualizing and analyzing the literature, enhances the understanding of highly cited keywords and emerging research hotspots.
According to the above results, the author believes that education is the primary research focus of cognitive reserve in stroke cognitive impairment rehabilitation. The primary clinical manifestations in patients with cognitive impairment include declines in memory, executive function, motor skills, and coordination ability. Research indicates that, in the years following a stroke, patients with lower incidences of cognitive impairment tend to have higher education levels, exhibiting fewer deficits in memory, language, visuospatial abilities, and structure.22 Other researchers posit that education correlates with an individual’s cognitive trajectory poststroke, suggesting that higher education levels may facilitate quicker recovery of cognitive functions within the first 3 months following an initial acute stroke.14 Given societal aging, it’s advocated that future research should coincide with contemporary developments, initiating cognitive intervention education for the elderly at the earliest opportunity. This approach aims to enlighten the elderly that maintaining a habit of continuous learning can help alleviate dementia and reduce the risk of cognitive impairment.23 Informing more individuals that cognitive impairment and dementia are preventable is crucial for meeting the clinical patients’ needs for more efficient and higher-quality treatment.
Several studies have examined the impact of engaging in cognitive stimulation activities on cognitive performance poststroke.5,24 For example, activities of daily living, hobbies, and social interactions poststroke show positive correlations with self-awareness, mindfulness, and functional abilities.25 Research suggests that poststroke patients who engage in intensive cognitive stimulation activities, such as reading, visiting museums, and traveling, demonstrate enhanced cognitive performance.26 Conversely, those who receive low levels of cognitive stimulation are at increased risk of worsening cognitive impairment as the disease advances. Additional research27–29 has demonstrated that social environments, including family emotional support, are associated with cognitive enhancements. Thus, in an aging society, prioritizing the healthiness of living environments is essential for preventing cognitive impairment in the elderly and crucial for effective recovery from illness.
It is noteworthy that the identification of risk factors for cognitive impairment poststroke shows inconsistency across various studies.30 Cognitive assessments frequently rely on screening tools, such as the mini-mental state examination (MMSE), Montreal Cognitive Assessment (MoCA), and other scales, which may overestimate their capability to detect cognitive changes.31 The limitations and diversity of these studies complicate a comprehensive understanding of the issue, warranting cautious interpretation. Currently, cerebrovascular changes are considered a principal cause of neurodegeneration, though the exact mechanisms remain undefined.32,33 Furthermore, the interactions among the type, location, and severity of vascular lesions, cognitive prognosis, and outcomes, along with individual neurostability and compensatory mechanisms over different time periods, remain incompletely understood.33–35 Consequently, longitudinal studies, incorporating neuroimaging, are essential to precisely assess the extent of nerve damage and explore cognitive trajectories and recovery poststroke.
Unlike other reviews, our CiteSpace analysis offers a unique visual perspective and frontier. This analysis sheds new light on the application of cognitive reserve in rehabilitating cognitive impairment poststroke. Given the numerous variables in the population and pathogenesis of cognitive impairment, future research should delve into the interactions between different onset times and stages across populations, aiming to clarify the interplay and impact between cognitive reserve and cognitive impairment. Specifically, further investigation is warranted to examine the bidirectional effects of cognitive reserve at different stages of stroke. However, the search was limited to a single English-language database, excluding others. CiteSpace utilizes unique algorithms for keyword identification and document analysis. Additionally, due to the paper’s limited length, specific details of research methods are not fully elaborated, and only a broad overview of the literature’s perspectives is provided.
Visual analysis via CiteSpace software reveals the significant role of education in enhancing cognitive reserve. Future research should delve into the interactions across diverse populations at various onset times and stages. However, the interplay among individual characteristics, including age, lesion type, and cognitive reserve agents, may mediate variations in cognitive decline post-stroke. Variations in study methodologies, such as follow-up intervals and cognitive outcomes, account for discrepancies in current findings. Limited research exists on the dynamic changes and governing principles of cognitive reserve across different poststroke stages. Future studies are essential to unravel the mechanisms and dynamic trajectories of cognitive reserve, its impact on poststroke cognitive prognosis, and its interplay with lifestyle factors, such as diet and exercise. Promoting cognitive reserve and brain health through pharmacological or psychosocial interventions is crucial for mitigating subsequent poststroke cognitive disorders.