Chronic kidney disease (CKD) is a progressive condition that affects more than 10% of the population globally. It accounts for a huge burden, especially in low-and middle-income countries.1 It impairs kidney function irreversibly and slowly, resulting in end-stage renal disease (ESRD). Patients with ESRD require dialysis or kidney transplantation to live.2 However, the patients receiving hemodialysis (HD) suffer a high symptom’s burden, which adversely impacts their quality of life (QoL).3 One of the most overwhelming symptoms suffered by HD patients is fatigue.4 According to Debnath et al.,5 fatigue is a subjectively overpowering sensation of tiredness even at rest or lack of endurance that interferes with everyday chores. It is a multifaceted concept with both physical and psychological aspects. Because it is illogical, unseen, and challenging to evaluate objectively, it is frequently disregarded by patients and caregivers.6
Understanding the factors that predict fatigue is crucial for helping HD patients to manage their weariness. The patients believe that identification of symtoms, along with the knowledge of the preferred treatment approaches, is the first crucial step in supporting innovation in symptom alleviation.7 The two psychological disorders that are thought to be most frequently associated with ESRD are depression and anxiety. These symptoms, which are all closely related to fatigue in HD patients, can deteriorate patients’ health and QoL and increase their risk of death.8–10
Fatigued HD patients experience more emotional and physical symptoms than non-fatigued HD patients.11 However, the overall symptom distress, the patients’ perception of their ability to manage their symptoms, and their relation to fatigue have not been investigated among HD patients. Although the specific cause of fatigue is not fully understood, it is known that several conditions are associated with its occurrence. Therefore, managing symptoms and addressing fatigue are crucial in the care of patients undergoing HD. Nursing assessment of factors related to fatigue plays a significant role in providing effective care for these patients.12
The present study aimed to evaluate the factors predicting fatigue among HD patients.
- 1.
What are the factors predicting fatigue among HD patients?
- 2.
What are the common associated distress symptoms and their rank among HD patients?
- 3.
What is the level of fatigue among HD patients?
The current descriptive study was conducted at the hemodialysis departments of Main Mansoura University and Mansoura International Hospitals in Mansoura, Egypt. A convenient sample of 200 subjects was enrolled for 6 months from January to June 2023. The sample size was calculated utilizing this formula: n = Z2 × (p) × (1–p)/d2, and it was 196, where the expected prevalence (p) of fatigue was 85% based on a previous study by Bossola et al.,13 the margin of error (d) = 0.05, and Z = 1.96.
The inclusion criteria included all available patients on HD for at least 3 months and who were aged ≥18 years.
The exclusion criteria included acutely ill patients, patients with physical disability, or those who were unable to participate.
The data were collected using four tools.
Part I: The demographic data sheet of the study subjects, consisting of age, sex, education, and occupation.
Part II: The medical history data sheet, which includes disease duration, frequency of HD, and duration of session.
The revised Piper Fatigue Scale (PFS) is used for assessing the multidimensional fatigue of patients with chronic diseases.14 It consists of 22 numerically scaled “0” to “10” items which measure the behavioral/severity (six items; from 2 to 7), affective meaning (five items; from 8 to 12), sensory (five items; from 13 to 17), and cognitive/mood (six items; from 18 to 23) dimensions of subjective fatigue. These 22 items are utilized to determine the total fatigue scores and the four sub-scale scores. The scores of 22 items are added, then divided by 22, and classified as either none (“0”), mild (“1–3”), moderate (“4–6”), or severe (“7–10”).
The Hospital Anxiety and Depression Scale (HADS) was validated among the Arab community by Malasi et al.15 and has a sensitivity of 79% and a specificity of 87%. It is composed of 14 items that measure the levels of anxiety and depression (7 items for each). All items obtain a score of “0–3’, and the total score is categorized as: normal from ‘0 to 7”, borderline from “8 to 10”, and abnormal from “11 to 21.”16
The General Symptom Distress Scale (GSDS) was adapted from Badger et al.17 In the first part, the patients were provided with a 12-symptom list that is common among patients diagnosed with chronic diseases. They were asked to rank symptoms from the most distressing (rank of 1) to the least distressing. In the second part, patients were asked to give an overall rating on a 10-point scale about how distressing their symptoms are; the higher the scores, the higher the distress. In the final part, patients were asked to globally rate their perceived ability to manage symptoms on a 10-point scale; higher scores indicate a better ability to manage their symptoms.
The data were collected using four tools, and the collected data were translated into Arabic. The international guidelines recommendations were applied for cross-cultural adaptation and translation to Arabic.18 To assess the validity of the tools, they were submitted to a jury of 5 experts in the field of medical surgical nursing to test clarity, relevance, understanding, and applicability of the study tools for implementation. They showed a good validity with a Coefficients of Variation (CVI) of 1.8, and the necessary modifications were made accordingly. The reliability of the tools was assessed using the Cronbach’s alpha test, which yielded internal consistency ratings of 0.93, reflecting high consistency.
A pilot study was carried out on a sample of 20 patients, and then excluded from the study sample. The pilot study aimed to test the feasibility and clarity of the study tools.
The study was conducted more than 8 months (from the beginning of December 2022 to the end of June 2023). To achieve the aim, the following management plan was applied: The first month was spent on conducting a thorough literature review and developing research instruments, the second month was spent on obtaining ethical approval, 2 months were spent for data collection, 2 months were spent for data analysis, 2 months were spent for finalizing the study. The eligible subjects were interviewed face-to-face and individually by the researchers to fill in the questionnaire.
The study was approved by the ethics committee of the Faculty of Nursing, Mansoura University on January 31, 2023 (IRB No. p 0398). Informed written consent was received from each participant after explaining the nature and objective of the study. The patients’ privacy and the confidentiality of the collected data were assured. The patients have the right to withdraw at any time from the study without penalty.
The data were tabulated and analyzed utilizing SPSS software (version 26) (IBM Corporation, Armonk, New York, United States). The descriptive statistics were utilized as frequency, percentage, mean, and standard deviation. The normality of distribution was assessed using the Z score, absolute value of the skewness, and kurtosis (±3.29). The chi-square and coefficient relations were used to assess the relationships between study variables. Variables, with P ≤ 0.05 on bivariate tests, were inserted into the multivariate linear regression model (enter method) to determine factors affecting fatigue.
In terms of socio-demographics, 52.5% of the study subjects were aged between 30 years old and <50 years old; 51.5% were female; 59.0% were not working; 52.0% were married; and 48.5% of them were educated at secondary schools. As regards the history of HD, it was found that 32.0% of the patients were under HD for 5–10 years, 81.5% of the patients under HD had three sessions a week, and 75.5% of them had 4 h of session (Table 1).
Sociodemographic Characteristics of the Study Subjects (N=200).
| Variables | N | % |
|---|---|---|
| Age (years) | ||
| 18-30 | 33 | 16.5 |
| 30-50 | 105 | 52.5 |
| ≥ 50 | 62 | 31.0 |
| Gender | ||
| Male | 97 | 48.5 |
| Female | 103 | 51.5 |
| Working Status | ||
| Working | 82 | 41.0 |
| Not working | 118 | 59.0 |
| Marital status | ||
| Single | 36 | 18.0 |
| Married | 104 | 52.0 |
| Widow/divorce | 60 | 30.0 |
| Level of Education | ||
| Primary | 61 | 30.5 |
| Secondary | 97 | 48.5 |
| Bachelor | 38 | 19.0 |
| Postgraduate | 4 | 2.0 |
| History of hemodialysis, years | ||
| < 1 | 49 | 24.5 |
| 1 to < 5 | 62 | 31.0 |
| 5 to < 10 | 64 | 32.0 |
| ≥ 10 | 25 | 12.5 |
| Frequency of dialysis sessions/Week | ||
| Two | 37 | 18.5 |
| Three | 163 | 81.5 |
| Duration of hemodialysis sessions, hours | ||
| < 3 | 8 | 2.0 |
| 3 | 41 | 20.5 |
| 4 | 151 | 75.5 |
Regarding fatigue, most study subjects had a moderate level of fatigue regarding all sub-dimensions of the PFS, with an overall mean of 116.74 from 220 (Table 2).
Fatigue levels among study subjects as measured by the Piper Fatigue Scale (N=200).
| Piper Fatigue Scale Sub-dimensions | Mild | Moderate | Sever | Mean | SD | |||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Behavioral/Severity | 13 | 6.5 | 162 | 81.0 | 25 | 12.5 | 34.69 | 9.9 |
| Affective Meaning | 50 | 25.0 | 115 | 57.5 | 35 | 17.5 | 26.34 | 10.7 |
| Sensory | 52 | 26.0 | 100 | 50.0 | 48 | 24.0 | 26.69 | 12.6 |
| Cognitive/Mood | 52 | 26.0 | 106 | 53.0 | 42 | 21.0 | 32.14 | 11.2 |
| Overall Fatigue | 36 | 18.0 | 146 | 73.0 | 18 | 9.0 | 116.74 | 31.8 |
Moreover, 78.5% of the study subjects suffer from anxiety, while 31.0% of them have depression. The total mean scores of total anxiety and depression are 12.76 and 8.11, respectively (Figure 1). Considering the severity of distressing symptoms as reported by the study subjects, it was found that fatigue, insomnia, and anxiety had the top-ranking mean scores. On the contrary, cough, vomiting, nausea, and shortness of breath got the lowest rankings (Figure 2).
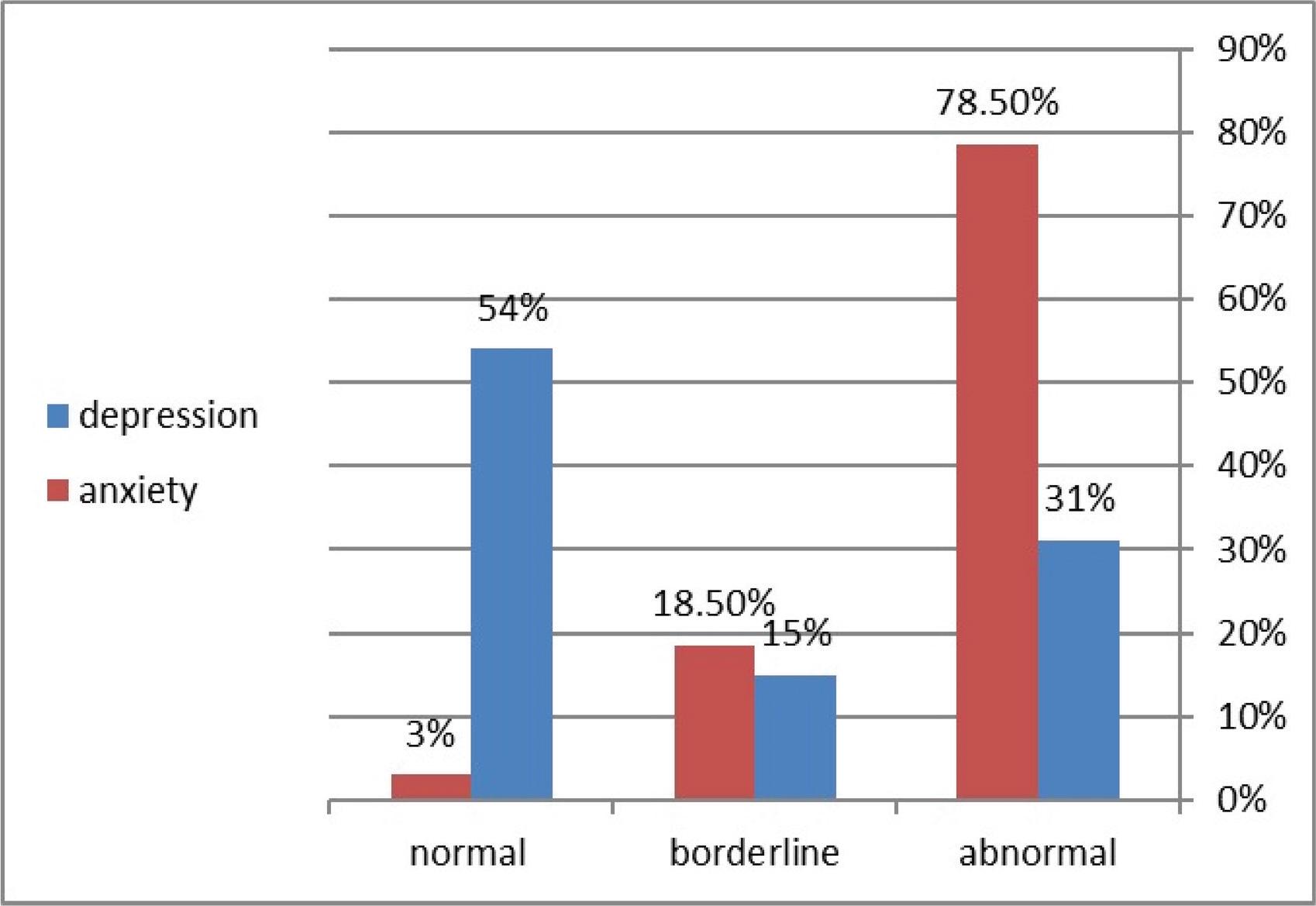
Anxiety and depression levels as measured by HAS among Study Subjects (N=200).
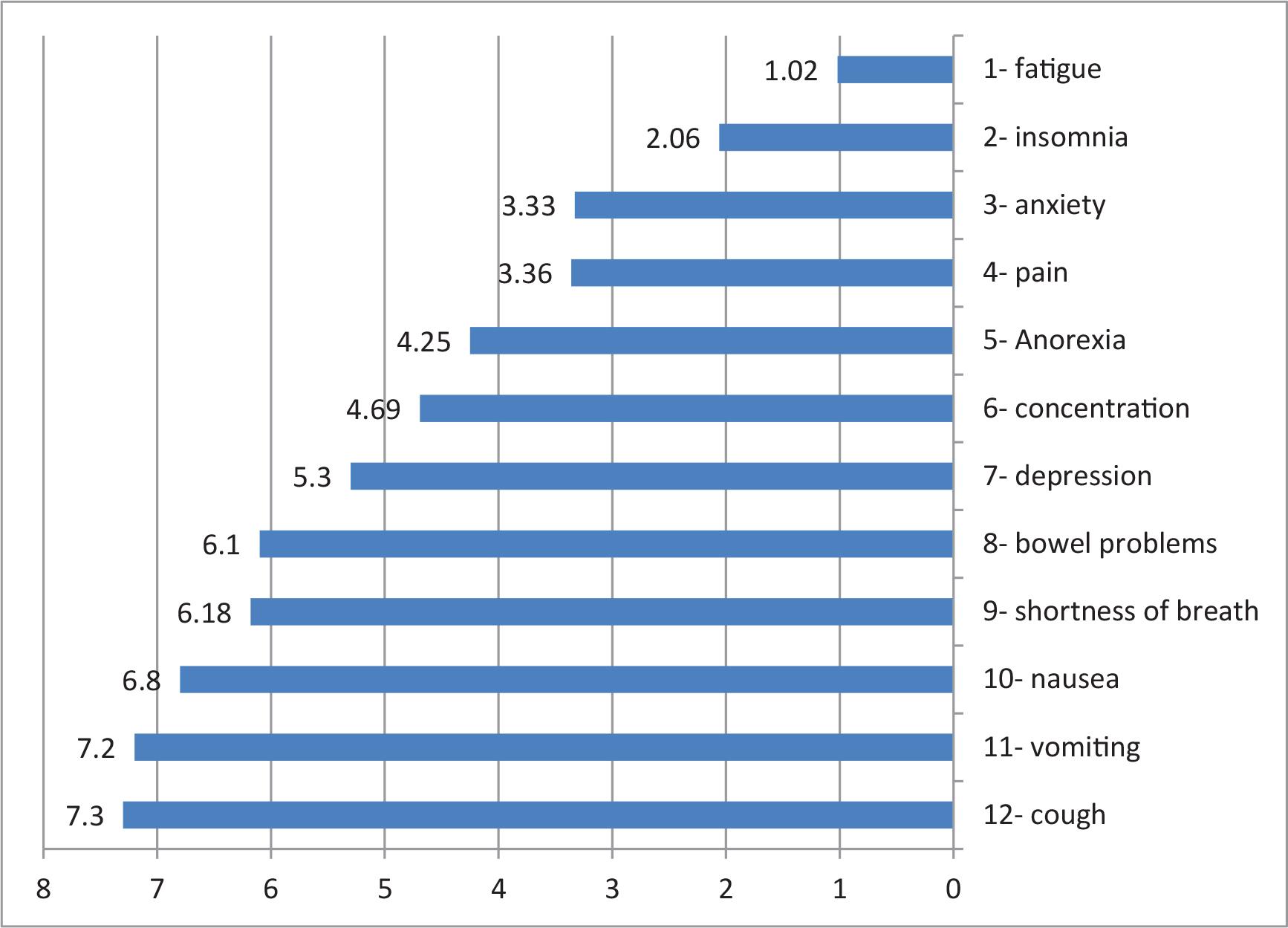
Mean ranks of the Total Symptom Distress Scale of the Study Subjects (N=200).
The overall mean score of anxiety and fatigue did not significantly correlate with the sociodemographic variables of the study subjects. There was a significant difference in the total depression mean scores of the study subjects as related to gender (P = 0.01) (Table 3).
Relation between the Sociodemographic Characteristics of the Study Subjects and Their Mean Fatigue, Anxiety, and Depression Scores (N=200).
| Variables | Anxiety | Depression | Fatigue | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Normal | Borderline | Abnormal | p-value | Normal | Borderline | Abnormal | p-value | Normal | Borderline | Abnormal | p-value | |
| Age (years) | 0.50 FET | 0.34 | 0.98 | |||||||||
| 18-30 | 1 | 9 | 23 | 13 | 5 | 15 | 7 | 23 | 3 | |||
| 30-50 | 2 | 19 | 84 | 59 | 15 | 31 | 18 | 78 | 9 | |||
| ≥50 | 3 | 9 | 50 | 36 | 10 | 16 | 11 | 45 | 6 | |||
| Gender | 0.38 FET | 0.01* | 0.53 | |||||||||
| Male | 3 | 14 | 80 | 47 | 22 | 28 | 17 | 69 | 11 | |||
| Female | 3 | 23 | 77 | 61 | 8 | 34 | 19 | 77 | 7 | |||
| Working Status | 0.58 FET | 0.64 | 0.78 | |||||||||
| Working | 3 | 18 | 61 | 46 | 10 | 26 | 15 | 61 | 6 | |||
| Not working | 3 | 19 | 96 | 62 | 20 | 36 | 21 | 85 | 12 | |||
| Marital status | 0.09 FET | 0.40 | 0.94 | |||||||||
| Single | 1 | 12 | 23 | 15 | 5 | 16 | 8 | 25 | 3 | |||
| Married | 2 | 15 | 87 | 60 | 16 | 28 | 17 | 78 | 9 | |||
| Widow/divorce | 3 | 10 | 47 | 33 | 9 | 18 | 11 | 43 | 6 | |||
| Level of Education | 0.25 FET | 0.87 | 0.72 FET | |||||||||
| Primary | 3 | 5 | 53 | 34 | 10 | 17 | 8 | 45 | 8 | |||
| Secondary | 2 | 19 | 76 | 51 | 16 | 30 | 18 | 72 | 7 | |||
| Bachelor | 2 | 7 | 29 | 21 | 3 | 14 | 9 | 26 | 3 | |||
| Postgraduate | 0 | 0 | 4 | 2 | 1 | 1 | 1 | 3 | 0 | |||
| History of the Hemodialysis,years | 0.22 FET | 0.17 | 0.52 FET | |||||||||
| < 1 | 0 | 9 | 40 | 20 | 13 | 16 | 8 | 35 | 6 | |||
| 1 to < 5 | 0 | 13 | 49 | 38 | 5 | 19 | 9 | 48 | 5 | |||
| 5 to < 10 | 4 | 11 | 49 | 36 | 8 | 20 | 15 | 46 | 3 | |||
| ≥ 10 | 2 | 4 | 19 | 14 | 4 | 7 | 4 | 17 | 4 | |||
| No of dialysis sessions/Week | 0.17 FET | 0.38 | 0.69 | |||||||||
| Two | 0 | 4 | 33 | 23 | 6 | 8 | 5 | 28 | 4 | |||
| Three | 6 | 33 | 124 | 85 | 24 | 54 | 31 | 118 | 14 | |||
| Duration of hemodialysis sessions, hours | 0.77 FET | 0.35 FET | 0.88 FET | |||||||||
| < 3 | 0 | 2 | 6 | 5 | 2 | 1 | 2 | 6 | 0 | |||
| 3 | 1 | 5 | 35 | 26 | 3 | 12 | 3 | 31 | 3 | |||
| 4 | 5 | 30 | 116 | 77 | 25 | 49 | 27 | 109 | 15 | |||
Note:. Statistically Significant (P < 0.05); FET: Fisher Exact Test.
In addition, a statistically significant negative relationship was shown between the frequency of HD sessions and the study subjects’ overall anxiety scores. Also, a positive correlation was found between fatigue and anxiety, depression, and overall symptom distress, whereas a negative correlation was found between fatigue and perceived ability to manage symptoms (Table 4). Multiple linear regression represents a highly positive effect of anxiety, depression, and overall symptom distress on fatigue level (B = 0.274 t = 3.716 P ≤ 0.001; B = 0.305 t = 4.489 P ≤ 0.001; B = 0.248 t = 3.285 P = 0.001, respectively) (Table 5).
Pearson Correlation between study variables (N=200).
| Variables | Fatigue | Anxiety | Depression | Overall symptom distress | Ability to manage symptoms |
|---|---|---|---|---|---|
| Hemodialysis session frequency | |||||
| Pearson correlation | –0.039 | –0.193 | 0.031 | -0.078 | -0.027 |
| P-value | 0.579 | 0.006** | 0.66 | 0.274 | 0.704 |
| Fatigue | |||||
| Pearson correlation | 0.287 | 0.148 | 0.325 | -0.21 | |
| P-value | < 0.001** | 0.036* | < 0.001** | 0.003** | |
| Anxiety | |||||
| Pearson correlation | 0.356 | 0.422 | –0.273 | ||
| P-value | < 0.001** | < 0.001** | < 0.001** | ||
| Depression | |||||
| Pearson correlation | 0.212 | 0.111 | |||
| P-value | 0.003** | 0.117 | |||
| Overall symptom distress | |||||
| Pearson correlation | –0.436 | ||||
| P-value | < 0.001** | ||||
Note: Statistically Significant (P <0.05);
Statistically Highly Significant (P <0.01)
Multiple linear regression model of psychological factors predicting fatigue (N = 200).
| Items | Unstandardized coefficient | Standardized coefficient | t | P value | |
|---|---|---|---|---|---|
| B | Sth. Error | B | |||
| Constant | 34.646 | 17.063 | 2.031 | 0.044 | |
| Total anxiety | 3.264 | 0.879 | 0.274 | 3.716 | <0.001** |
| Total depression | 1.913 | 0.426 | 0.305 | 4.489 | <0.001** |
| Overall symptom distress | 6.155 | 1.873 | 0.248 | 3.285 | 0.001** |
| Ability to manage symptoms | –1.163 | 1.337 | –0.062 | –0.869 | 0.386 |
| ANOVA | |||||
| Model | Df | F | |||
| Regression | 4 | 13.527 | <0.001** | ||
Note: Dependent variable: total fatigue score;
Significant at P <0.05;
Highly significant at P <0.01.
HD treatment for ESRD has debilitating symptoms like fatigue, depression, anxiety, and distress, which may affect the patient’s QoL.19 The present study aimed to evaluate the factors predicting fatigue among HD patients. Fatigue is a common distressing symptom among HD patients,3 and a complex phenomenon that includes physical, emotional, and psychological components.6 The preliminary study results showed that most study subjects were experiencing a moderate level of fatigue regarding all sub-dimensions of the PFS, and they ranked fatigue as the top distressing symptom among other symptoms experienced by HD patients. This finding agrees with Zuo et al.,10 who concluded that the prevalence of fatigue was high, and its level was moderate in HD patients. Also, Sheshadri et al.20 and Moskovitch et al.21 reported fatigue as the most reported and most bothersome symptom among HD patients. Another study also reported that HD patients prioritize fatigue, depression, and anxiety as the most bothersome symptoms that need new therapies.12 These results recognize fatigue as an important nursing issue for patients undergoing HD. It is necessary to provide alternative solutions for improving their fatigue. Enhancement in HD patients’ experience of fatigue must be further explored for a better understanding of related mechanisms and developing efficient therapeutic interventions.13
As regards sociodemographic associations, the study results show no significant relationship between the total fatigue scores of the study subjects and their demographic variables. In the same line, Kodama et al.22 reported that age and gender did not significantly affect fatigue. This result reflects how, despite the different demographic characteristics of our study subjects, HD had an impact on their level of fatigue. Although some previous studies showed significant relations, Tsirigotis et al.23 revealed that comorbidities, advanced age, marital status, and education level had a statistically significant positive correlation with fatigue level.
The results of the present study indicated that anxiety scores were higher than depression; more than three-quarters of the study subjects were suffering from anxiety, while less than one-third of them had depression. This may be related to the frequency and length of the dialysis sessions, limitations on the patients’ independence and autonomy, dietary restrictions, and their inability to engage in customary social activities with their families. These results agreed with Gerogianni et al.24 who stated that the prevalence rates of anxiety and depression were 35.9% and 29.4%, respectively. However, anxiety prevalence was lower compared with the present study, and this may be because most of the study subjects in this study were males, and women had higher levels of depression and anxiety than males according to Gerogianni et al.,24 The present study and Al-Jabi et al.25 support the same results, as females had significantly higher levels of depression than males. In contrast, another study revealed that the prevalence of anxiety was lower than that of depression.26 This may be due to the fact that most subjects were older than 60 years, and elderly patients commonly suffer from depression.
Factors predicting fatigue in the present study include anxiety, depression, and overall symptom distress. This is in accordance with Al Naamani et al.19 where anxiety and depression were the main predictors of fatigue among HD patients. Also, Ouyang et al.27 reported that patients who suffer from psychological problems such as depression and anxiety have higher levels of fatigue. Furthermore, fatigued HD clients more frequently experience physical and emotional symptoms than non-fatigued clients.11 Another qualitative study reported that psychological effects and disease-imposed constraints and needs were the top etiologies of fatigue and its continuity among these patients.28 Another study reported psychological distress as a predictor of fatigue, and they also reported perception of ability to manage symptoms as a predictor of fatigue among HD patients.29 In the present study, even though patients’ perceived ability to manage symptoms did not predict fatigue, there was a strong negative relationship between the subjects’ ability to control their symptoms and their levels of fatigue, anxiety, and symptom distress, which should be considered in patients’ care.
Finally, the present study has some limitations. First, because the study is cross-sectional, we cannot determine if anxiety, depression, and overall symptom distress cause fatigue or if fatigue leads to anxiety and depression. Second, the study subjects were recruited entirely from dialysis centers in Mansoura, which could limit the generalizability of the reported results to the broader Egyptian population or other countries. Finally, the research study relied on patient-reported questionnaires to evaluate psychological issues, which may not be the same as a clinical diagnostic interview.
In conclusion, HD patients were found to be experiencing many symptoms, such as fatigue, anxiety, and depression, at varying levels. Fatigue was ranked as the top distressing symptom among HD patients, with psychological factors such as anxiety, depression, and overall symptom distress predicting fatigue. The study suggests that regular screenings for fatigue, anxiety, depression, and overall symptom distress should be conducted for all patients with CKD undergoing HD. Additionally, the study suggests that psychological therapies to modulate these factors might decrease fatigue severity and its related disability in HD clients. Finally, multidimensional nurseled interventions involving physical and psychological therapies are required to manage fatigue in HD patients.