
The pressure ulcer advisory panels defined a pressure ulcer/injury as “localized damage to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear, but may also occur from medical devices or other objects.”1,2
A lack of repositioning compliance results in vessels being constricted under gravitational pressure, which stops or critically minimizes the amount of blood passing through to the target tissues.3 This soon results in irreversible tissue damage,4 which might occur even earlier in overweight patients.5 Irreversible tissue damage then initiates the formation of a pressure injury.6,7 Pressure ulcers reduce patients’ quality of life8 and place a burden on hospital resources as the prevention cost is much less than the treatment cost.9 According to the current understanding of pressure formation, relieving pressure from the bony prominences or sites of medical devices is the cornerstone in preventing pressure ulcer formations.3,4,10,11
Experts consider patient repositioning to be a significant pressure ulcer prevention measure1,2,12 that is defined as an effort to regularly modify patient posture.13 In hospital settings, repositioning is a nursing responsibility14 and hospitals have created repositioning policies to help nurses achieve proper repositioning.15 Nurses are accountable for complying with such policies to prevent the incidence of pressure ulcers. Repositioning compliance refers to the performance of repositioning in manner of such quality and frequency to achieve the pressure relief.
However, it has been observed that compliance with repositioning policy in nursing units is low.16,17 Low compliance refers to situations in which nurses are unable to achieve the required quality or frequency in repositioning patients according to policy instructions. For instance, in Saudi Arabia, the national guideline states that hospitals must clarify what pressure ulcer preventions are in place, including their repositioning policy18,19 but clinical evidence indicates that nurses typically do not comply with the repositioning policy.15,20 Internationally, the situation is similar. In the United States, reports indicate that only 40% of patients in need of repositioning were treated appropriately.21 This was also the case as observed in India where approximately only 30% of patients received the required repositioning.22 Results of studies were similar in Belgium,23 Sweden,24 Egypt,25 China,26 Australia,27 Hong Kong, China,28 Saudi Arabia,15,20 and the Netherlands.29 Therefore, low repositioning compliance is an observed phenomenon among nurses in hospitals across cultures. Therefore, this article aimed to identify factors affecting repositioning policy compliance among nurses at the clinical level to support stakeholders in understanding repositioning compliance phenomena and to aid in the design of suitable changes to evidence-based repositioning policy. To achieve this goal, we followed the methodology used by Whittemore and Knafl30 to answer the review question: “What are the factors affecting repositioning compliance among nurses in clinical units?” The review methodology consists of five steps: problem identification, review of the studies, evaluation of the data, data analysis, and presentation of findings.
Although nurses’ compliance in performing repositioning should be 100% compliance with repositioning policy ranges between 13.9%23 and 75%.14,31 The current low compliance rate increases the possibility that at-risk patients will develop pressure ulcers32 as well as highlights the low quality of nursing care that patients are subjected to.8,9 Therefore, leaders and stakeholders are obligated to identify the reasons for this low compliance.
This review included manuscripts published between 1997 (when the European Pressure Ulcer Advisory Panel [EPUAP] began) and 2019 and included all studies that investigated factors influencing nurses’ repositioning compliance. Cohort studies were included if they outlined or reported factors associated with repositioning compliance among nurses. Qualitative studies and quality projects were included if the studies presented repositioning compliance among nurses as a concern. The search was not limited to any specific methods of addressing repositioning compliance as a primary or secondary outcome of processes indicated for preventing pressure ulcers. Studies that investigated repositioning compliance among non-nursing staff or in a non-pressure ulcer prevention context were not included.
The following electronic databases were searched: Coherence Wounds Group (Jan 1997 to Jun 2019), Ovid MEDLINE (Jan 1997 to Jun 2019) based on the Saudi Commission for Health Specialties (SCFHS) access, EBSCO CINAHL (Jan 1997 to Jun 2019), Clinical Key database (Jan 2014 to Oct 2018), and the reference sections of retrieved studies. During the search, the authors applied the same terms to all databases, which are as follows: repositioning compliance, positioning compliance, repositioning, change in patient positioning, change patient position, pressure ulcer prevention, pressure ulcer prevention policy/guideline, pressure injury prevention, pressure ulcer injury policy/guideline, bedsores prevention, and decubitus ulcer prevention.
Studies reporting repositioning compliance in any healthcare facility that requires nurses to comply with repositioning intervention to prevent pressure injury formation were included in this article. No limitations were established based on the type of hospital, scope of services, or nursing home.
No limits were placed on the types of interventions applied to improve repositioning compliance or pressure ulcer management. The study criteria included studies that presented repositioning compliance as an outcome or process indicator for pressure ulcer management.
The initial search identified 923 citations (776 from electronic databases and 147 from the reference check). A total of 122 duplicated reports were subsequently excluded. Of the remaining 801 studies, 497 reports were excluded because they did not assess pressure injury prevention. Thereafter, 304 studies were reviewed by general reading, and an additional 215 studies were excluded for failing to meet the inclusion criteria (191 evaluated repositioning compliance among non-nursing personnel, and 24 did not analyze repositioning compliance as a nursing intervention). The entire text of the remaining 89 studies was reviewed. A total of 30 studies did not discuss factors related to repositioning policy compliance as a concern, and the authors differed in their opinions about five studies. After consultation, these studies were excluded from the analysis. A total of 54 studies met the criteria, as presented in the PRISMA chart (Figure 1).
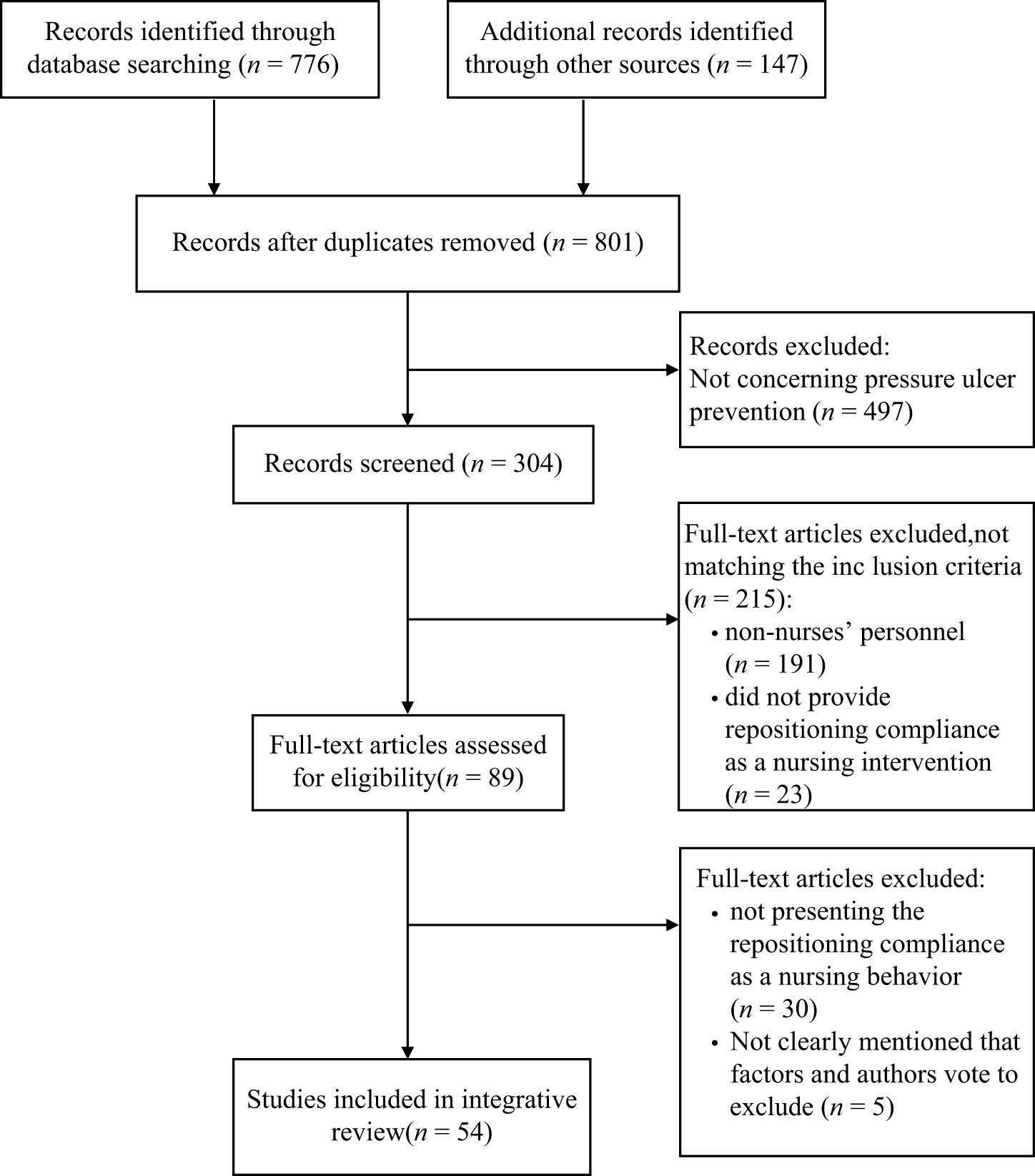
PRISMA chart.
The authors reviewed the selected studies separately. The evaluation revised the titles of studies retrieved from the database search. Complete reports of all potential studies that matched the above-mentioned criteria were prepared on an Excel sheet for ease of access and then arranged in tables. In cases of disagreement, a senior author was asked to adjudicate on the inclusion of studies. The authors listed the causes for rejection and were not blinded to the study authorship. The authors evaluated the references used in the revised studies to verify any further reports that met the selection criteria.
Two authors autonomously evaluated the risk of bias in the selected studies. For clinical trials, the authors implemented the Cochrane Collaboration’s tool.33 The authors ranked the studies as low risk, high risk, and unclear (unknown) risk of bias.33 They also applied critical appraisal for qualitative studies to evaluate the quality level. Each qualitative study was evaluated for level of credibility, transferability, dependability, and confirmability.34 The studies were ranked on a three-point scale (high, moderate, and low) for each of the aforementioned items.34
A total of 54 studies matched the inclusion criteria. These included 4 studies of randomized controlled trials, 5 qualitative studies, 14 quasi-experimental studies, 3 retrospective studies, and 15 cross-sectional studies, as well as 4 prospective design studies, 2 observational studies, 4 quality projects, 2 triangulation studies, and 1 longitudinal study. The studies show a low to moderate level of bias, as presented in Table 1; however, no study was excluded from the analysis due to bias risks.
Summary of available studies that present the motivations for repositioning compliance.
| Author and country | Population and sample | Design (level of evidence) | Findings |
|---|---|---|---|
| Alexander et al. USA | Nurses in nursing homes N = 2 | Observational (VI) | Face-to-face communication is increased when an IT system with a low level of sophistication that includes the repositioning decision is used to prevent pressure injuries, and a higher level of care is provided when a highly sophisticated IT system is used. |
| Ali et al. Egypt | Nurses in a hospital N = 83 | Longitudinal study (VI) | The changes in nurses’ performance regarding pressure injury prevention, which includes repositioning, resulted from changes in the administrative focus and the involvement of nurses in the responsibilities. |
| Amon et al. USA | Medical-surgical telemetry patients | Pre-post Intervention (III) | The incidence of pressure ulcer PU was reduced as a result of compliance with pressure injury prevention policies, including repositioning. |
| Angmorterh et al. UK | Nursing students N = 49 | Prospective experimental (III) | The pressure placed on volunteers when moving the patient on the radiology trolley is high, and the settings are not convenient for the repositioning of the patient during the diagnostic procedures in radiology. |
| Athlin et al.5 Sweden | Nurses N = 30 | Qualitative content analysis (VI) | Pressure injury prevention compliance, including repositioning, is associated with:
|
| Beeckman et al. Belgium | Hospitalized patients N = 2,105 | Cross-sectional study (VI) |
|
| Beeckman et al. Belgium | Patients in nursing homes N = 464 | RCT (II) | After implementing the supported clinical decision, nurses’ knowledge and positive attitudes increased but did not result in significant changes in their compliance toward pressure injury prevention, including repositioning, while increased compliance with the pressure injury prevention policy was observed for patients in wheelchairs. |
| Behrendt et al. UK | Hospitalized critical care patients N = 422 | Prospective control study (IV) | Following the implementation of specific equipment that provides continuous and consistent visual feedback for nurses, nurses exhibit better compliance with repositioning. No further education or any further policy changes were implemented. |
| Black and Maegley USA | Hospitalized patients 23 beds in a medical-surgical unit | Quality improvement project (III) | The project demonstrates changes in the nurses’ compliance with pressure injury prevention, including repositioning, after the application of a new policy, forms, and follow-up system. |
| Cameron et al. UK | Nurses in the NHS | Quality improvement project (III) | The project presents the experiment performed in the NHS to provide the pressure ulcer prevention program online. The project assumes an increase in pressure ulcer prevention compliance, including repositioning. |
| Chaboyer et al. Australia | Hospitalized patients N = 1,600 | Clustered randomized control trial (II) | The study shows a decrease in the incidence of pressure ulcers and an increase in prevention following the application of the pressure injury prevention care program, including repositioning, but statistically significant differences were not observed between the overall compliance of nurses in both groups. |
| Choi et al. USA | Nurses in critical care facilities N = 15 | Quality improvement project (III) | The low compliance of nurses is associated with:
|
| Courvoisier et al. Switzerland | Patients in nursing homes N = 2,671 | Cross-sectional study (VI) | The study reported relations between the prevalence of pressure ulcers and the type and size of nursing homes. |
| Co x USA | Hospitalized critical care patients N = 347 | Retrospective correlational design (IV) | The study concludes that the predictability of the Braden scale is questionable. The most reliable predictions were based on patient mobility and friction/shear. Many risk factors have been identified empirically; however, a consensus on the most important risk factors is lacking. 18.7% of patients developed a pressure ulcer. |
| Cub ukcu Turkey | Patients in nursing home care units N = 786 | Cross-sectional study (VI) | The study concludes that pressure ulcer development is associated with the Braden score, weak nutritional conditions, and chronic illnesses. |
| Cyriacks and Spencer USA | Hospitalized patients 32 beds in a pulmonary unit | Quality improvement project (III) | The study shows increased repositioning compliance following the redistribution of the nursing staff and creation of a turning team from nurses on duty. |
| Dellefield and Magnabosco USA | Nurses in hospitals N = 16 | Triangulation study design (III) |
|
| Feng et al. China | Nurses in hospital N = 275 | Pre-/post-intervention quasi-experimental study (III) | Improvements in the knowledge and attitudes of nurses toward pressure ulcer prevention and repositioning through an awareness campaign are associated with higher levels of compliance and a lower incidence of pressure ulcers. |
| Fossum et al. Norway | Nurses in a nursing home N = 15 | Quasi-experimental study (III) |
|
| Gunningberg et al. Sweden | Patients in the geriatric/internal medical ward N = 190 | Pragmatic randomized trial (III) |
|
| Hanna et al. USA | Nurses working in different organizations N = 429 | Cross-sectional study (VI) |
|
| Hartmann et al. USA | Nurses in a nursing home N = 23 | Qualitative study (VI) | Staff provided the following indirect impressions of the facilitators and barriers associated with pressure ulcer prevention:
|
| Hall and Clark USA | Patients in a medical unit and surgical ICU N = 100 | Pre- and Post-intervention (III) | The study concludes that the device reduces the repositioning burden among nurses, increases repositioning compliance, and reduces the HAPU among the selected units. |
| Kalisch et al. USA | Nurses in hospitals N = 4,086 | Cross-sectional study (VI) |
|
| Kalisch et al. USA | Patients and relatives in hospitals N = 729 | Cross-sectional study (VI) | Patients with pressure ulcers (they did not receive the proper prevention measures, including repositioning) reported higher rates of missed nursing care in the following areas:
|
| Källman and Suserud Sweden | Nurses in a hospital N = 154 | Cross-sectional study (VI) |
|
| Källman et al., Sweden | Hospitalized patients N = 62 | Non-experimental, observational study (VI) | The study concludes that repositioning compliance is associated with:
|
| Knibbe et al. Netherlands | Patients in nursing homes N = 13 | Quasi-experimental pre- post-intervention study (III) | The case reports did not reveal a significant difference in nurses’ compliance with repositioning before and after implementing repositioning facilities. However, the study presents the importance of the availability of this device in reducing nurses’ working-related hazards. |
| Kwong et al. Hong Kong | Patient and nurses in nursing homes N = 474 | Action research of three main steps (III) | The changes in nurses’ behavior in complying with repositioning resulted from the factors listed below:
|
| Lavallée et al. UK | Nurses in the hospital N = 25 | Qualitative study (VI) | The study defined seven domains that interact as barriers or facilitators in manipulating nurses’ behavioral compliance, which are listed below.
|
| Lu et al. China | Bedridden patients in a gynecological unit N = 150 | RCT – Two armed (II) | The report shows a significant increase in the implementation of pressure ulcer prevention measures (including repositioning) after applying the protocol. Significant reductions in pressure ulcer incidence were also observed after applying the clinical guideline. |
| Mallah et al. Lebanon | Patients in a hospital N = 468 | Quasi-experimental pre- post-intervention study (III) |
|
| Meesterberends et al. | Patients in nursing homes N = 547 Germany and The Netherlands | Prospective multicenter cohort study (IV) |
|
| Mendoza et al. Saudi Arabia | Inpatient units N = 17 | Pre- and post-intervention (III) | An awareness campaign increases nurses’ compliance in preventing pressure ulcers. |
| Moore and Price Ireland | Nurses in a hospital N = 121 | Cross-sectional study (VI) |
|
| Moya-Suárez et al. Spain | Nurses working in hospitals N = 249 | Cross-sectional study (VI) |
|
| Peterson et al. USA | Patients in a hospital N = 23 | Observational study (VI) |
|
| Renganathan et al. India | Hospitalized critical care patients N = 40 | Prospective, non-randomized, multiphase, multicenter trial (III) | The use of a continuous repositioning monitoring system increases nurses’ compliance with the repositioning protocols. |
| Rich et al. USA | Hospitalized patients N = 269 | Observational study (VI) |
|
| Saliba et al. UK | Patients in nursing homes N = 834 | Retrospective analysis (III) |
|
| Samuriwo UK | Nurses in nursing homes N = 16 | Qualitative grounded theory (VI) |
|
| Samuriwo UK | Nurses in nursing homes N = 16 | Qualitative grounded theory “Reanalyzed data” (IV) | The reanalysis of the data also concludes a substantial role for multidisciplinary teamwork and nursing empowerment in compliance with pressure ulcer prevention measures, including repositioning. |
| Still et al. USA | Hospitalized critical care patients in a surgical ICU N = 507 | Pre- and post-intervention quasi-experimental study (III) | Significant changes in repositioning compliance were observed after the staff were redistributed to establish a turning team in the unit. |
| Strand and Lindgren Sweden | Nurses in intensive care units N = 146 | Cross-sectional study (VI) |
|
| Schutt et al. USA | Hospitalized patients N = 138 | Quasi-experimental pre- post-intervention study (III) |
|
| Sving et al. Sweden | nurses in hospitals N = 9 | Triangulation study design (III) |
|
| Sving et al. Sweden | Hospitalized patients N = 825 | Descriptive cross-sectional study (VI) |
|
| Tannen et al. Germany and Netherland | Hospitalized patients and residents in nursing homes | Cross-sectional study (VI) | The study defines the differences in pressure ulcer prevention, including the repositioning compliance between two countries as related to:
|
| Tayyib and Coyer Saudi Arabia | Hospitalized critical care patients N = 140 | Clustered randomized control trial (II) |
|
| Tayyib et al. Saudi Arabia | Hospitalized patients N = 28 | Prospective observational study (VI) |
|
| Ünver et al. Turkey | Nurses in a hospital N = 101 | Cross-sectional study (VI) |
|
| Webster et al. Australia | Hospitalized patients with pressure ulcers N = 133 | Retrospective cohort study (IV) | The study reviewed the long-term effects of applying protocols on the compliance level. The study supports the hypothesis that nurses’ long-term compliance will increase when a bundle of care or protocols to organize the care is available. |
| Weiner et al. Israel | Nurses in a hospital N = 48 | Post-test (III) | The study classifies the participants into three groups in which repositioning was performed with different levels of assistance for patients with different weights. The equipment plays an important role in reducing low back pain among nurses, which improves compliance. |
| Wogamon USA | Nursing assistants in hospitals N = 33 | Non-randomized trial (III) |
|
After evaluating all retrieved studies and determining which ones were relevant based on the inclusion/exclusion criteria, the authors individually extracted data using a predesigned data collection sheet designed for this study based on the recommendations of Souza, Silva, and Carvalho35 The designed table summarizes the following information from the included studies, as described in the criteria in Polit and Beck36 type of publication, methodological characteristics, and level of evidence. The data extraction and analysis were based on the content of each study. The datasheet contained the information is listed in Table 1.
All studies agreed that repositioning policy compliance is a mandatory nursing practice but presented various factors and different effects with respect to repositioning compliance. Twelve factors were found to influence repositioning policy compliance. These factors were repeated 97 times across all the studies reviewed, as presented in Table 2. The most frequently mentioned variables included nursing attitudes and quality projects (15 studies), while other factors include nursing knowledge, skills, staffing, teamwork, direct managerial feedback, nursing empowerment, nursing assignments, availability of repositioning assistance devices, and patients’ characteristics. The summary descriptions for all studies are presented in Table 1.
Frequency of factors influencing repositioning compliance reported among the studies.
| Factor | Frequency of studies |
|---|---|
| Individual factor – Attitude | 15 |
| Individual factor – Knowledge | 10 |
| Individual factor – Skill | 5 |
| Environmental – Managerial follow-up | 3 |
| Environmental – Staffing | 15 |
| Environmental – Teamwork | 7 |
| Environmental factor – Equipment | 12 |
| Environmental factor – Quality projects | 15 |
| Environmental – Digital visualization | 3 |
| Patient factor – Age | 2 |
| Patient factor – Weight | 2 |
| Patient factor – Medical condition | 8 |
| Total | 97 |
The studies present nursing characteristics that influence nurses’ compliance with repositioning policy and are referred to as nursing-related factors. These factors include nursing knowledge, nursing skills, and nursing attitudes toward repositioning. Nurses require a minimum level of nursing knowledge to comply with repositioning policy.37,38,39 Studies present nursing knowledge as the level of information that nurses have regarding the need for repositioning policy compliance in pressure ulcer prevention.
The nursing repositioning knowledge includes general identification of the characteristics of repositioning as an intervention.40,41 It also includes an understanding of the assessment tools to determine at-risk patients.23 However, the studies do not standardize repositioning knowledge definitions but agree that the knowledge resource should be consistent with the international pressure ulcer guidelines.1,2
The second factor is nursing skill. Nursing skill in performing repositioning is divided into two parts: the ability of nurses to perform the procedure42,43 and the absence of any physical restraint that would prevent them from complying with repositioning policy.44 A nurse’s ability to perform the procedure indicates that the nurse has the required competencies to “reposition” the patients based on the predefined steps in the policy.45
The third individual factor is the nurses’ attitude. The attitude of nurses was defined as a critical factor among studies that investigated nurses’ compliance with repositioning policy.23,46 Researchers assume that attitude is the main factor contributing to nurses’ compliance with repositioning policy. Nurses have profound antagonistic feelings regarding repositioning policy compliance because repositioning – in their view – is a procedure that should be delegated to students and practical nurses, and it does not need to be performed by a registered nurse.47,48 These negative attitudes also weaken the focus of nurses to follow up on compliance with repositioning after delegation.
Patients’ characteristics also affect compliance with repositioning policy.41 For instance, patients with excess weight,41 old age,24 and pressure ulcers5 receive less repositioning than patients who are bedridden with the same conditions. Patients on medications that treat psychosis also receive less repositioning.5 While these two clinical conditions should not influence nurses in terms of less compliance with repositioning policy, patients with oncological disorders receive higher repositioning policy compliance.24
The studies did not determine whether this behavior was related to nurses’ perceptions regarding the importance of repositioning policy compliance or a negative attitude of care.24 These findings pave the way for further follow-up and in-depth investigations. Therefore, nurses’ managers should follow up on vulnerable patient groups regarding the nature of nursing care and ensure repositioning compliance.
Environmental factors are variables that reflect on the nurses’ surroundings. These factors comprise of the digital visualization feedback, teamwork, staffing, direct managerial feedback, quality improvement projects, and repositioning assistant aids. These are tangible and non-tangible supporting factors for improving repositioning policy compliance.
The first factor is digital visualization feedback. This is an electronic system that follows up on repositioning progress by the assigned nurses and presents the repositioning performance on a public screen in the unit.21,22,49 Thus, repositioning policy compliance for each staff member is in public view and the digital visualization feedback significantly improves compliance.21,22,49 However, repositioning compliance improved only when nurses were provided with visualizations of their levels of performance in a public place. There were no studies in which nurses’ compliance levels improved if compliance was not made publicly visible. Thus, the visualization of nurses’ level of performance in a public place significantly improved compliance.
The second factor is nursing teamwork. Repositioning policy compliance requires synchronized human efforts from two to three nurses to complete the patient shifts, safely establish a new posture,50 and frequently repeat the procedure based on the policy. Teamwork is a compulsory factor in establishing repositioning policy compliance.51 However, studies present the absence of teamwork as a barrier to ensuring repositioning policy compliance.52 Furthermore, the shared responsibilities inherent in teamwork play a role in reminding53 and motivating nurses21 to comply with repositioning policy. Therefore, the relationship between the clinical team and repositioning policy compliance is vital and logical.
Third, an appropriate number of nursing staff to provide proper workload distribution had a positive effect on repositioning policy compliance. For example, in the study by Cyriacks and Spencer,40 modifying the nursing staffing plan improved the repositioning compliance. The staffing plan was modified by assigning nurses to repositioning teams; these teams were responsible for the repositioning of all at-risk patients. Furthermore, as per the investigation in Still et al.,54 the manager redistributed nurses to organize a team that focused on performing the repositioning with no further assignments. However, these interventions required employing more nurses in the units or withdrawing nurses from other units and assigning them to repositioning tasks only, but this would only create a heavier workload on the remaining nurses.49 Therefore, modifying the staffing plan to include the required number of nurses would allow these nurses to adhere to the repositioning policy as well as complete other nursing tasks.
Direct managerial feedback on repositioning policy compliance also enhances nurses’ performance56 and thus, represents the fourth factor. Evidence indicates that when frontline managers make more effort to follow up on repositioning policy compliance, nurses demonstrate a higher compliance level.25,57
The fifth factor is quality improvement projects. A quality improvement project is a multidisciplinary effort aimed at enhancing or improving the practice related to pressure ulcer prevention in the hospital. Studies demonstrate that an increase in repositioning policy compliance occurs in institutions that have quality improvement projects.48,51,56 Hospitals with quality improvement plans to reduce pressure ulcer formations follow and monitor nursing behavior in repositioning compliance. These effects are observed with all types of quality projects either at the higher26,58 or at the lower administrative level.29,40
Sixth, repositioning aids are devices or tools that support nurses during the repositioning procedure.59 The absence of these aids was mentioned as a barrier for ensuring a good repositioning policy in two qualitative studies and led to complaints from the nurses.47,49 However, other evidence contradicted any role of the presence of a repositioning aid in enhancing nurses’ compliance.35,56 In addition, while such aids are likely to play an essential role in facilitating compliance, it might be a secondary variable in these situations.
Overall, this article presents several factors that influence nurses to comply with the repositioning policy. These factors do not affect the nurses’ behaviors separately, but rather simultaneously. In essence, the factors are not independent of each other but go hand in hand. However, there is no available evidence to consider the effects of these factors on each other. For instance, enhancing nursing knowledge will have an impact on nursing attitudes; how one factor affects another would be reflected on the compliance of the nurses to the repositioning policy. In another example, organizations that work to enhance the nursing knowledge among nurses may be focused on other things at the same time such as quality improvement projects or the purchase of repositioning aids. Therefore, the compliance of the nurses would be representative of how these factors affect/influence each other. However, there are no available studies that present these relations at the clinical level or how these actions interact together to shape the repositioning policy compliance phenomena, but the available knowledge about its effects may suffice.
A nursing manager will not be able to organize a straightforward evidence-based practice that does not take all of these factors into consideration. This article presents groups of factors in different categories. Each of these factors affects each other in various ways, but there is no method available that can identify or calculate the effect of these factors collectively. Hence, there is a need for further investigation to understand the synergy between these factors and how they interact to influence nurses’ compliance with the repositioning policy.
This article presents several issues related to repositioning compliance. First, it is a significant challenge in many hospitals. Also, repositioning compliance is a multifactorial phenomenon,60 and several factors influence the nursing compliance level. Hospitals need to interact with the current challenges in the immediate future. The hospital intervention should assure the presence of systematic efforts to address poor compliance. Specifically, only single interventions or focusing on specific aspects will not necessarily lead to the desired changes. Thus, changing the current situation requires an understanding of all of these factors and organizing the change interventions that take all of these issues into consideration. Nursing management must consider all these factors in organizing a straightforward evidence-based practice to enhance repositioning compliance.
The authors designed a chart that presents all these factors that relate to repositioning policy compliance (Figure 2).

Presentation of the factors.
Several factors influence repositioning policy compliance. This integrative literature review of 54 studies reveals three main types of factors that influence nurses’ compliance with repositioning policy: nurse-related factors, patient-related factors, and environment-related factors. The nurse-related factors include nurses’ knowledge, skills, and attitudes toward repositioning compliance. Patient-related factors include patients’ age, weight, the presence of a pressure ulcer, and certain medical diagnoses, such as cancer or the use of medications to treat psychosis. The environment-related factors include digital visualization feedback, teamwork, staffing, direct managerial feedback, availability of quality improvement projects, and availability of repositioning supporting aids. The conclusions of this article demonstrate the necessity of including all these factors to overcome the challenges of developing evidence-based programs to improve the repositioning compliance of nurses.
This integrative literature review did not exclude any study on repositioning policy compliance that was published in English; however, other relevant studies that were either not published in English or not available for review may have been overlooked. Thus, repositioning policy compliance might be modified by additional influential factors that are not presented in this review.