
Electronic nicotine delivery systems (ENDS, also known as e-cigarettes) are battery-powered electronic devices which heat a liquid solution, most commonly containing nicotine, to form an inhalable vapor (1). Compared with traditional cigarettes which combust tobacco (2), causing the formation of thousands of potentially harmful chemicals which smokers inhale (3), the vapor from ENDS contains many fewer toxicants, and those which are present are typically found at significantly lower levels than those in cigarette smoke (4–6). Due to these significantly lower toxicant yields of e-cigarette vapor compared with cigarette smoke, a number of both longitudinal and cross-sectional assessments of biomarkers of toxicant exposure have demonstrated that complete switching from cigarette smoking to using ENDS products reduces biomarker levels, in some cases to levels seen in never smokers (7–12). Although it has not yet been explicitly demonstrated, this is expected to have a beneficial impact in reducing the considerable harm associated with cigarette smoking. The global toll of smoking-related disease has been estimated at up to 100 million deaths in the 20th century (13), and the reduced harm potential of ENDS means that they may provide a viable solution to a global public health issue and greatly reduce the disease burden associated with cigarette smoking (14). Modelling studies have suggested that the availability of ENDS could prevent over 6 million deaths in the United States (U.S.) alone this century, resulting in a predicted reduction in life years lost of over 86 million (15). This potential population health benefit has led many public health bodies, such as Public Health England (now known as the UK Office for Health Improvement and Disparities), the UK Royal College of Physicians, the New Zealand Ministry of Health and Health Canada (6, 16–18), to support the use of ENDS as a potentially reduced-harm alternative to cigarette smoking for adult smokers, particularly those who have been unable to quit using other methods.
An increasingly strong body of evidence, coming from randomized controlled trials, uncontrolled intervention studies, and observational studies, suggests that ENDS help to support smokers in their switching away from combustible cigarette smoking, particularly when ENDS are used daily and non-intermittently (19–25). Furthermore, at the population level a recent analysis demonstrated that in countries which have a high adoption level of alternative nicotine products such as ENDS have been able to achieve a lower prevalence of cigarette smoking (26). It has been proposed that in order to maximize the ability of ENDS to help smokers switch, both the appeal and the dependence potential (also known as abuse liability) of any given ENDS need to be optimized in order to make the use of that ENDS a viable and satisfactory alternative to smoking cigarettes (14, 27). In this regard, appeal encompasses the attractiveness of the ENDS product, its sensory characteristics, and its ability to elicit subjective satisfaction. Dependence potential (also known as abuse liability) refers to the potential for the ENDS product to provide satisfaction and induce a degree of addiction, which is a function both of its pharmacological and its subjective rewarding and sensory properties (14). Given this proposition, assessing the appeal and dependence potential of ENDS is critical in order to be able to assess both their ability to help smokers switch and to understand their tobacco harm reduction potential. Due to this need, the U.S. F
Abuse liability is a composite measure incorporating assessments of both the nicotine pharmacokinetics and subjective effects during use of an ENDS product (27, 30). For nicotine pharmacokinetics, Cmax (the maximum blood nicotine concentration) and Tmax (the time at which the maximum blood nicotine concentration occurs) are considered to be the most important factors contributing to an abuse liability assessment (27, 30–32). For subjective effects, studies typically assess a number of subjective domains including satisfaction, product liking, and intent to use again (27, 30). This paper describes two independent studies, one study in smokers and another in ENDS users, in which nicotine pharmacokinetics and subjective effects were assessed in order to estimate the abuse liability of two flavor variants (tobacco and menthol) of a novel ENDS product, the RELX Infinity ENDS. The abuse liability assessments are compared with the abuse liability of combustible cigarettes and nicotine gum in smokers, and with the abuse liability of subjects’ usual brand ENDS in ENDS users. Separate populations were evaluated in each study to provide information on the abuse liability of the products and their potential to provide an acceptable alternative for both smokers and ENDS consumers. The data are intended to be used in conjunction with that from other clinical and nonclinical studies to establish the potential of the Infinity ENDS to contribute to tobacco harm reduction through displacement of combustible cigarettes by a potentially less toxic product that provides sufficient appeal and satisfying levels of nicotine for the intended consumer population.
The studies described in this manuscript were open-label, randomized, crossover, confined clinical studies (clinical-trials.gov identifiers NCT04640285 [Study 1] and NCT04620616 [Study 2]) conducted at either one or two clinical sites in the United States (U.S.). Study 1 was conducted at Altasciences Clinical Kansas Inc (Overland Park, KS, U.S.) and Study 2 was conducted both at that site and at WCCT Global Inc. (Cypress, CA, U.S.). Prior to study commencement each study was approved by the WCG Institutional Review Board (IRB; Puyallup, WA, U.S.). Both studies were conducted in compliance with the study protocol, with the U.S. Code of Federal Regulations (CFR) 21 Parts 50, 56, and 312, with the ethical principles set forth in the Declaration of Helsinki, Good Clinical Practice (GCP), and with the International Council for Harmonization (ICH) harmonized tripartite guideline regarding GCP (E6 Consolidated Guidance, April 1996). All subjects provided written informed consent prior to the commencement of any study procedures, including screening assessments.
Eligibility was assessed during a screening process to ensure that subjects were in generally good health, satisfied all of the inclusion criteria, and met none of the exclusion criteria. General health evaluations included a standard physical examination (including vital signs and an electrocardiogram [ECG]), medical history (including concomitant medications), and clinical laboratory assessments (chemistry, hematology, urinalysis, serology, drug, and alcohol screening). In Study 1, subjects were required to be 21 to 59 years of age, inclusive, at the time of consent, to have been a smoker for at least 12 months prior to Screening, and to self-report typically smoking 10 or more 83 mm (king size) to 100 mm combustible cigarettes per day. Smoking status was confirmed by an expired breath carbon monoxide (eCO) level > 10 ppm and a urine cotinine concentration ≥ 200 ng/mL at Screening and at Check-in to the site. Primary exclusion criteria included any clinically significant uncontrolled medical condition that could jeopardize the safety of the subject or impact the validity of the study results, other clinically significant abnormal findings, any acute illness (e.g., upper respiratory infection, viral infection) within 14 days prior to Check-in, use of very low nicotine content (VLNC) cigarettes (e.g., Moonlight, Spectrum) as their usual brand, use of any tobacco-or nicotine-containing products (including ENDS) other than manufactured cigarettes within 7 days of Check-in, postponement of a planned smoking quit attempt in order to participate in the study, and females who were pregnant or lactating.
The inclusion and exclusion criteria for participation in Study 2 were similar to those described above, except that subjects were required to have been a daily ENDS user for at least 3 months prior to Screening and through Check-in, to self-report weekly use of at least 3 mL of e-liquid from an ENDS product at Screening, and to have an exhaled carbon monoxide (eCO) concentration < 10 ppm at Check-in. In addition, subjects were not to have used any tobacco-or nicotine-containing products (including cigarettes) other than ENDS products within 7 days of Check-in.
Study 1 aimed to randomize at least 20 non menthol and 20 menthol cigarette smokers to ensure that at least 16 of each type evaluated each study product. Study 2 aimed to randomize at least 30 ENDS users to ensure that at least 25 evaluated each study product.
The RELX Infinity ENDS is a two-piece closed-system ENDS comprised of a rechargeable 380 mAh battery (RELX Infinity device) with a power output of 6.5 W and a disposable pod (RELX Pod Pro). The pods contain the mouthpiece and heating element and are pre-filled with 1.9 mL of tobacco- or menthol-flavored e-liquid. The heating element is activated upon inhalation by the consumer which generates an inhalable aerosol from the e-liquid. A maximum puff duration of 5 s is controlled by the device. Each e-liquid contains a mixture of glycerin, propylene glycol, nicotine salts (4% nicotine concentration by weight, approximately 46.4 mg/mL), and a proprietary blend of flavorings.
In Study 1, subjects’ usual brand combustible cigarettes served as a high abuse liability reference product. Usual brand cigarettes were limited to those which were non VLNC, machine-manufactured, and commercially available in the U.S. Nicorette® White Ice Mint 4 mg nicotine polacrilex gum (GlaxoSmithKline Consumer Healthcare, L.P., London, UK) served as a low abuse liability reference product.
In Study 2, subjects’ usual brand ENDS products served as the study comparator product. Similar to Study 1, the subjects’ usual brand was chosen as a positive control to maximize the benefit of using a familiar product for which the subjects had established behaviors and preferences. Users of closed-system products commercially available in the U.S. were initially recruited. No limitations on nicotine strength or usual brand flavor were set, provided that the subjects agreed to use either a tobacco- or menthol-flavored e-liquid with their device while at the clinical site. Due to recruitment challenges (low numbers of closed-system ENDS users in the locality of the clinic site and COVID-related recruitment issues) the protocol was amended to add a second clinic site and to also allow recruitment of open-system ENDS users. The ENDS product use duration and weekly e-liquid volume inclusion criteria remained in place regardless of which type of ENDS subjects were using. Following this protocol change, recruited subjects who were open-system ENDS users were asked to use only a closed-system ENDS of their own choosing for 7 days prior to Check-in at the clinic site, and that closed system ENDS was deemed their ‘usual brand ENDS’ for the purposes of product comparisons and data analyses.
To minimize bias and reduce sequence effects, subjects in each study were randomly assigned to a product use sequence using a randomization scheme based on a Williams Latin squares design. The subjects were not informed of the sequence in which they were to use the products; however, the nature of the study products prohibited blinding during use.
The studies evaluated nicotine pharmacokinetics, subjective effects, and product safety of the Infinity ENDS compared with either combustible cigarettes and nicotine gum, or with the subjects’ usual brand ENDS. An overview of each study design is presented in Figure 1.
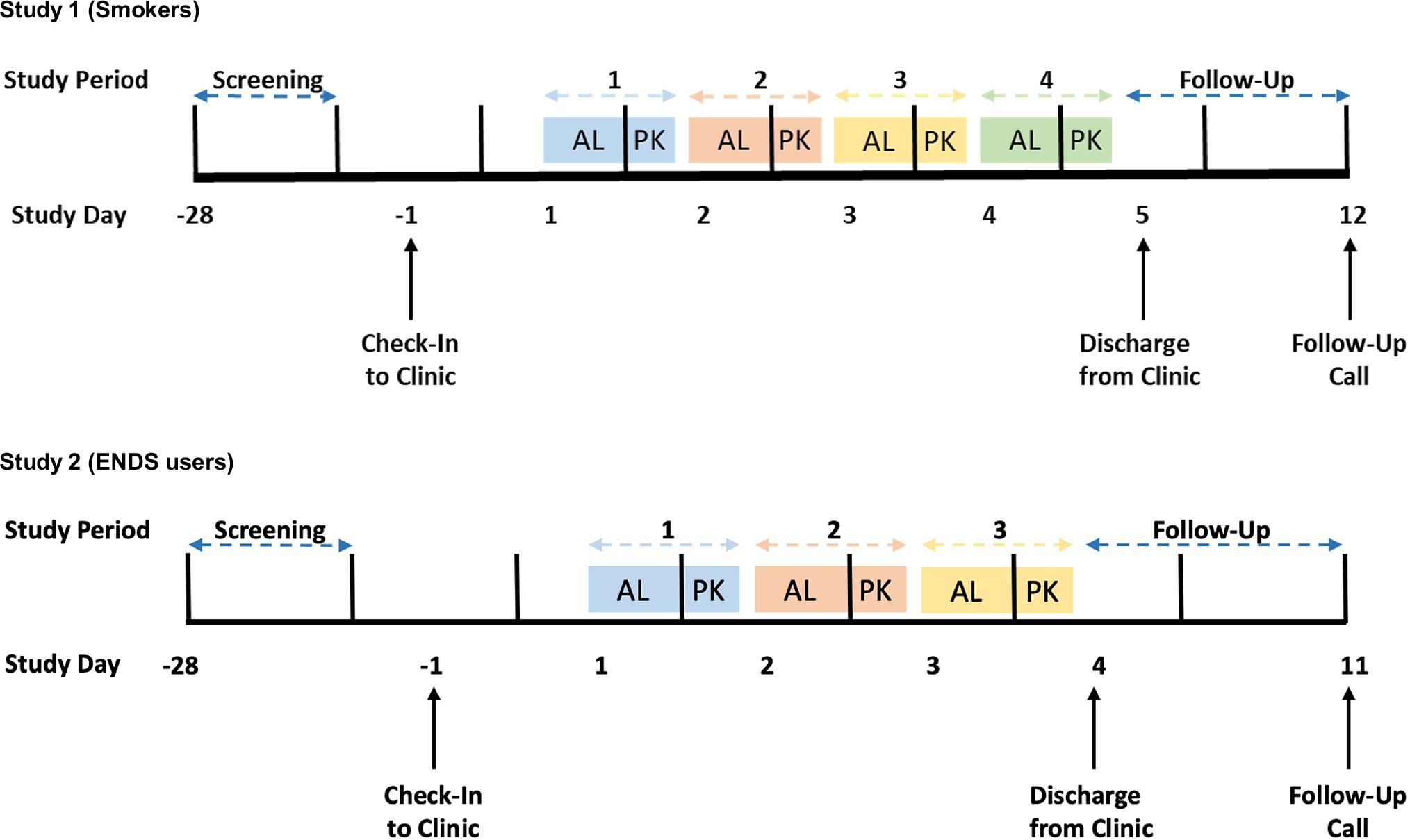
Overview of study designs. In both studies, subjects underwent an 8-h ad libitum (AL) use session, after which they abstained from any nicotine product use for 10–13 h prior to nicotine pharmacokinetic (PK) sessions the following day. This sequence was followed once for each study product, in a randomized order. Each product use study period was completed over approximately 24 h. Subjects were confined to the clinic site throughout the assessments.
At the screening visit, potential subjects underwent assessments to check their eligibility to participate in the study, to review their health status, and to assess their tobacco/nicotine product use habits status. Subjects were reminded to continue with their usual smoking/ENDS use behaviors from Screening through Check-in.
Subjects checked in to the clinic on Day −1 and remained in the clinic through completion of study events on Day 4 (Study 2) or Day 5 (Study 1), or upon early termination from the study. All subjects were contacted by telephone approximately 7 days following discharge (including early termination, unless deemed unnecessary in the opinion of an investigator) to document the occurrence of any adverse events (AEs) and to assess the use of concomitant medications since discharge.
Subjects used each of the assigned products during two use sessions in separate study periods according to the randomization sequence. Each study period was completed over approximately 24 h. The first session consisted of 8-h of ad libitum study product use, allowing for the subjects to become familiar with the study products. During the 8-h sessions, blood sampling for nicotine concentration measurement, puffing topography, vital signs, and product use data were collected (these data are not reported in this manuscript), and subjective effects questionnaires were administered. The second use session (referred to as the “PK Session”) took place the following morning and followed a period of abstinence from the use of any nicotine-containing products of between 10 and 13 h. At the start of the PK Session, subjects underwent a 5-min period of ad libitum use of the ENDS products, a 5-min period of ad libitum smoking of a single combustible cigarette of the subject’s usual brand, or a 30-min use period with nicotine gum.
During the PK Session, product use was documented, including the weight of the Infinity and usual brand ENDS pods/cartridges before and after use, blood was sampled for nicotine concentration measurement, subjective effects questionnaires were administered, eCO was assessed (Study 1 only), and physiologic endpoint (blood pressure [BP] and heart rate [HR]) measurements took place, over 120 min. To minimize exposure to sensory cues and the potential for contamination, subjects used each assigned product in separate designated areas of the study site(s). To further minimize bias, subjects were instructed not to discuss their responses to the subjective effects questionnaires with one another.
Venous blood samples for plasma nicotine analysis were collected at −5, 2, 4, 6, 7, 8, 10, 12, 15, 30, 60 and 120 min relative to the start of the product use session. Samples were analyzed by Altasciences Bioanalytical and Research Services (Laval, QC, Canada) using a validated liquid chromatography coupled to tandem mass spectrometry (LC-MS/MS) detection analytical method in accordance with FDA Good Laboratory Practice regulations (Title 21 CFR Part 58).
A modified form of the Product Evaluation Scale (mPES), in which language was changed slightly from the original version of the PES (33) to more accurately assess ENDS effects, a future intent to use (FIU) scale (visual analog scale [VAS] asking ‘If given the opportunity, would you use this product again in the future?’ with responses anchored with ‘Definitely would not’ and ‘Definitely would’, an urge to smoke/vape (UTS/UVP) scale (VAS anchored with ‘Not at all’ and ‘Extreme’), and a product liking (PL) scale (VAS asking ‘How much do you like the product right now’ with responses anchored with ‘Not at all’ and ‘Extremely’), were administered electronically using a tablet device (Cambridge Cognition, Cambridge, MA, U.S.). The mPES and FIU questionnaires were each administered at a single timepoint following the 8-h ad libitum use sessions, and the UTS/UTV and PL questionnaires were each administered at several timepoints (−30 [UTS/UTV only], 2, 5, 10, 15, 30, 45, 60 and 120 min) relative to the initiation of product use during the PK sessions. For the mPES questionnaire, subscale scores in the domains of satisfaction, psychological reward, aversion, and relief were generated from the individual items as described previously (33).
Safety and tolerability were evaluated based on data collected from physical examinations, clinical laboratory tests, vital signs measurements, and AEs. AEs spontaneously reported by the subjects or observed by the investigator or other study personnel were monitored from the time subjects first used the study product until the end of the study. AEs were summarized according to the study product most recently used. Any concomitant medications taken were also documented.
As these were the first studies assessing nicotine pharmacokinetics of the Infinity ENDS, no formal sample size calculations could be performed. Furthermore, no clinically relevant differences in nicotine pharmacokinetics, subjective effects, or physiologic response endpoints, have been established that may specifically distinguish the level of abuse liability between two tobacco/nicotine products. However, considering the number of products being compared, sample sizes of 40 subjects (Study 1) and 30 subjects (Study 2) are in line with similar study designs in the literature (34–44) and thus were deemed sufficient to meet the study objectives.
Data management and statistical analyses were performed by Altasciences (Overland Park, KS and Laval, QC, Canada). Subjective effects response parameters and statistical summarizations and comparisons were calculated using SAS version 9.4 (SAS, Cary, NC, U.S.). The comparisons of interest included the Infinity ENDS products versus the usual brand products and nicotine gum. Statistical comparisons were not made between the ENDS products or between the usual brand products and nicotine gum. Differences were deemed statistically significant if p < 0.05.
Measured plasma nicotine concentrations below the limit of quantitation (0.200 ng/mL) were set to one-half of the lower limit of quantitation for data summarization and calculation of PK parameters. Baseline correction for each post-baseline value was applied using the pre-use time point (−5 min) for each product use session as the baseline value. Baseline correction for each post-baseline value was applied using the formula for exponential decay as described previously (45, 46) with the nicotine concentration at the pre-use time point (−5 min) set as the baseline value for each product use session. Negative values resulting from the correction were assigned a value of zero in the analyses. Noncompartmental analysis (NCA) was based on actual sampling times, except for pre-use samples which were reported as time zero regardless of time deviations, provided that they were collected prior to product use.
NCA was performed using Phoenix® WinNonLin® software (Version 8.3; Certara, Princeton, NJ, U.S.). The following plasma nicotine pharmacokinetic parameters were derived from the baseline-adjusted concentrations: Cmax (maximum observed plasma concentration over the duration of the measurement interval after time zero), Tmax (time of maximum observed plasma nicotine concentration), and AUC(0–15) and AUC(0–120) (area under the nicotine concentration-time curve calculated from time zero [defined as the start of use session] to 15 and 120 min post start of session, respectively). AUC parameters were calculated using the linear trapezoidal method.
The primary pharmacokinetic endpoints of the studies included baseline-adjusted nicotine Cmax and AUC(0–120). Linear mixed-effects models for analysis of variance (ANOVA) were performed using SAS Version 9.3 (SAS, Cary, NC, U.S.) on the baseline-adjusted log transformed nicotine Cmax and AUC(0–120) data for each study. The models included study product, period, sequence, and sex as fixed effects, and subject as a random effect. From each model, the geometric least-squares means (LSmeans) and two-sided 90% confidence intervals (CIs) were calculated for each study product. Geometric mean ratios for each paired comparison, 90% CIs, and p values were calculated. Secondary pharmacokinetic endpoints were baseline-adjusted plasma nicotine AUC(0–15) and observed Tmax. A linear mixed-effects ANOVA model similar to the primary endpoints was performed on the baseline-adjusted log transformed nicotine AUC(0–15) data. The Hodges-Lehmann’s median analysis was used to estimate the median of the paired differences and two-sided 90% CIs of Tmax between the study products (47). P values were calculated using the corresponding Wilcoxon signed-rank test. Because the Wilcoxon signed-rank test does not rank subjects with zero differences between scores before calculation of the p value, paired scores equal to 0 were excluded before calculation of the two-sided 90% CI for the median of the paired difference so that CIs and corresponding p values would provide consistent results (48).
Responses for all subjective effects questionnaires were summarized by time point. Change from baseline (pre-use to post-use) was summarized for UTS/UTV and physiologic endpoint (HR and BP) values. Derived parameters for UTS/UTV included Emax_R (maximum reduction post-product use from pre-product use score over the duration of the measurement interval), Emax (maximum effect among all the post-product use assessments over the duration of the measurement interval), TEmax_R (time of the maximum reduction in response over the duration of the measurement interval), and AOE (area over the effect-time curve relative to pre-product use from time zero to the relevant time point as calculated by the linear trapezoidal method). Inferential analyses were performed on mPES multi- and single-item subscales, FIU scores, PL maximum response, and UTS/UTV Emax_R, Emax, TEmax_R, and AOE, and physiologic (HR and BP) endpoints.
A linear mixed-effects model for analysis of variance/ covariance (ANCOVA) was performed if the residuals were normally distributed. The model included study product, period, sequence, and sex as fixed model effects, the baseline score as a covariate, and subject as a random effect. The residuals from each mixed-effects model were investigated for normality using the Shapiro-Wilk W test. If the residuals from the mixed effects model were normally distributed, i.e., p value ≥ 0.05, contrasts were output from the mixed-effects model. LSmeans, standard error (SE), and 2-sided 95% CIs for products and product differences were derived from the mixed-effects model. P values were calculated for the effects and the contrasts. If the normality assumption of the model was not satisfied for any endpoint, a t-test or a sign test (48) was used depending on the distribution and skewness of each paired difference. If a t-test was used, treatment differences were presented using least-squares means (SE) and 2-sided 95% confidence intervals (CIs); for the sign test, median of the paired difference, first quartile [Q1] to third quartile [Q3), and 2-sided 95% CIs were presented. Like the Wilcoxon signed-rank test, the sign test does not rank subjects with zero differences between scores before calculation of the p value. Hence, paired differences equal to 0 were removed before calculation of the two-sided 95% CIs so that CIs and corresponding p values would provide consistent results (48).
In Study 1 (cigarette smokers), 107 potential subjects were screened. Of these, 66 failed screening and 41 were randomized to a product use sequence. The main reasons (≥ 5 subjects) for screening failure were not passing the drug/alcohol screen, failing the clinical laboratory tests, and failing the eCO > 10 ppm inclusion requirement. Brief demographic details are shown in Table 1. Mean age of the subjects was approximately 40 years, 58.5% were male, and approximately two-thirds were white. Two subjects were of Hispanic/Latino ethnicity.
Subject demographics by study.
| Summary statistics / characteristics | Study 1 - Smokers | Study 2 - ENDS Users | |
|---|---|---|---|
| N | Number | 41 | 29 |
| Age, years a | Mean (SD) | 39.9 (9.51) | 39.8 (11.09) |
| Sex, n (%) | Male | 24 (58.5) | 17 (58.6) |
| Female | 17 (41.5) | 12 (41.4) | |
| Race, n (%) | White | 27 (65.9) | 13 (44.8) |
| Black or African | 13 (31.7) | 14 (48.3) | |
| American | |||
| American Indian or Alaska Native | 0 (0) | 1 (3.4) | |
| Other | 1 (2.4) | 1 (3.4) | |
| Ethnicity, n (%) | Not Hispanic or | 39 (95.1) | 24 (82.8) |
| Latino | |||
| Hispanic or Latino | 2 (4.9) | 5 (17.2) | |
| Body mass index (kg/m2) | Mean (SD) | 29.1 (4.86) | 26.6 (4.84) |
| PS[E]CDI total score b | Mean (SD) | 12.1 (2.8) | 11.4 (3.6) |
At time of informed consent.
PSCDI administered to smokers, PSECDI administered to ENDS users. Higher scores indicate a higher level of dependence.
Abbreviations:
Electronic Nicotine Delivery Systems; maximum; minimum; number of observations; Penn State [Electronic] Cigarette Dependence Index; standard deviation.
Among the randomized subjects, on average they had been smoking for > 15 years (range 2–44 years). Twenty-one subjects were menthol cigarette smokers and 20 were nonmenthol cigarette smokers, with mean (SD) consumption of 14.5 (4.81) and 20.0 (7.75) cigarettes per day, respectively. One subject reported having used an ENDS within 30 days prior to Screening, while 25 subjects reported ever-use of an ENDS.
In Study 2 (ENDS users), 71 potential subjects were screened across the two study sites. Of these, 38 failed screening and 29 entered the study and were randomized to a product use sequence. Four subjects passed screening but were not randomized. The main reasons (≥ 3 subjects) for screening failure were not meeting usual brand ENDS use requirements, not passing the drug/alcohol screen, vital signs outside of the normal range, and abnormal ECG. Brief demographic details are shown in Table 1. Mean age of the subjects was approximately 40 years, 58.6% were male, and approximately half were black/African American. Five subjects were of Hispanic/Latino ethnicity.
Among the randomized subjects, on average they had been using their usual brand ENDS for approximately 1 year (range < 1 year to 6 years) and used an average of 10 mL of e-liquid per week. The majority of subjects (approximately 80%) were using a closed-system ENDS with a salt-based e-liquid at the time of screening and approximately 35% of subjects reported most commonly using a tobacco flavor, 21% reported a menthol flavor, and approximately half reported using a flavor other than tobacco or menthol. Nine subjects reported having smoked within 30 days of Screening and 21 subject reported having ever smoked. During the study, VUSE Alto was the most common device used [11], followed by JUUL [6] and NJOY Ace [2]. Ten other device/pod combinations were used by 1 subject each. A 5% nicotine e-liquid strength was used during the study by 22 subjects, while 3 subjects used a 2.4% strength, 2 subjects used a 3% strength, and 1 subject each used a 1.8% and 3.6% strength.
In their respective studies, subjects smoked one usual brand cigarette, used one piece of nicotine gum over 30 min, or were allowed to use the Infinity or usual brand ENDS products as much or as little as desired over 5 min, during the PK Sessions. Two ENDS users were mistakenly allowed to use usual brand flavors other than tobacco or menthol and their data from these periods were excluded from summarization. Median (range) pre- to post-use pod mass loss for smokers was 0.0386 g (0.0011–0.1090 g) for the Infinity Tobacco ENDS and 0.0412 g (0.0048–0.1256 g) for the Infinity Menthol ENDS. Use was higher among the ENDS users, but relatively consistent across products, with median (range) pod mass loss of 0.0641 g (0.0116–0.1251 g) for the Infinity Tobacco ENDS, 0.0692 g (0.0103–0.1370 g) for the Infinity Menthol ENDS, and 0.0633 g (0.0149–0.0296 g) for the usual brand ENDS.
Plasma nicotine levels rose and reached a peak following the end of product use during the PK session in both smokers (Figure 2A) and ENDS users (Figure 2B) for all study products. In smokers, the peak plasma nicotine concentration (Cmax) was significantly lower (p < 0.05) for both Infinity Tobacco ENDS and Infinity Menthol ENDS (mean [CV] values of 18.5 [100.2%] ng/mL and 16.6 [84.9%] ng/mL, respectively) compared with usual brand cigarettes (mean [CV] 27.0 [60.5%] ng/mL) and significantly higher (p < 0.05) compared with nicotine gum (7.5 [56.2%] ng/mL; Table 2 and Table 3). Median Tmax values were 6 min for both Infinity ENDS flavors, 7 min for usual brand cigarettes, and 35 min for nicotine gum (Table 2). These values were not significantly different between both Infinity ENDS flavors and usual brand cigarettes (p > 0.05), but significantly different between both Infinity ENDS flavors and nicotine gum (p < 0.05; Table 3). Regarding nicotine overall exposure (AUC(0–15) and AUC(0–120)), values were highest for usual brand cigarettes, lowest for nicotine gum, and intermediate with consistent results for both Infinity ENDS flavors (Table 2). For AUC(0–15) and AUC(0–120), values were significantly lower for the two Infinity ENDS flavors compared with usual brand cigarettes (p < 0.05; Table 3). In contrast, when compared to nicotine gum, AUC(0–15) was significantly higher for both Infinity ENDS flavors (p < 0.05; Table 3) but the difference between the products was not significant for AUC(0–120) (p > 0.05; Table 3).
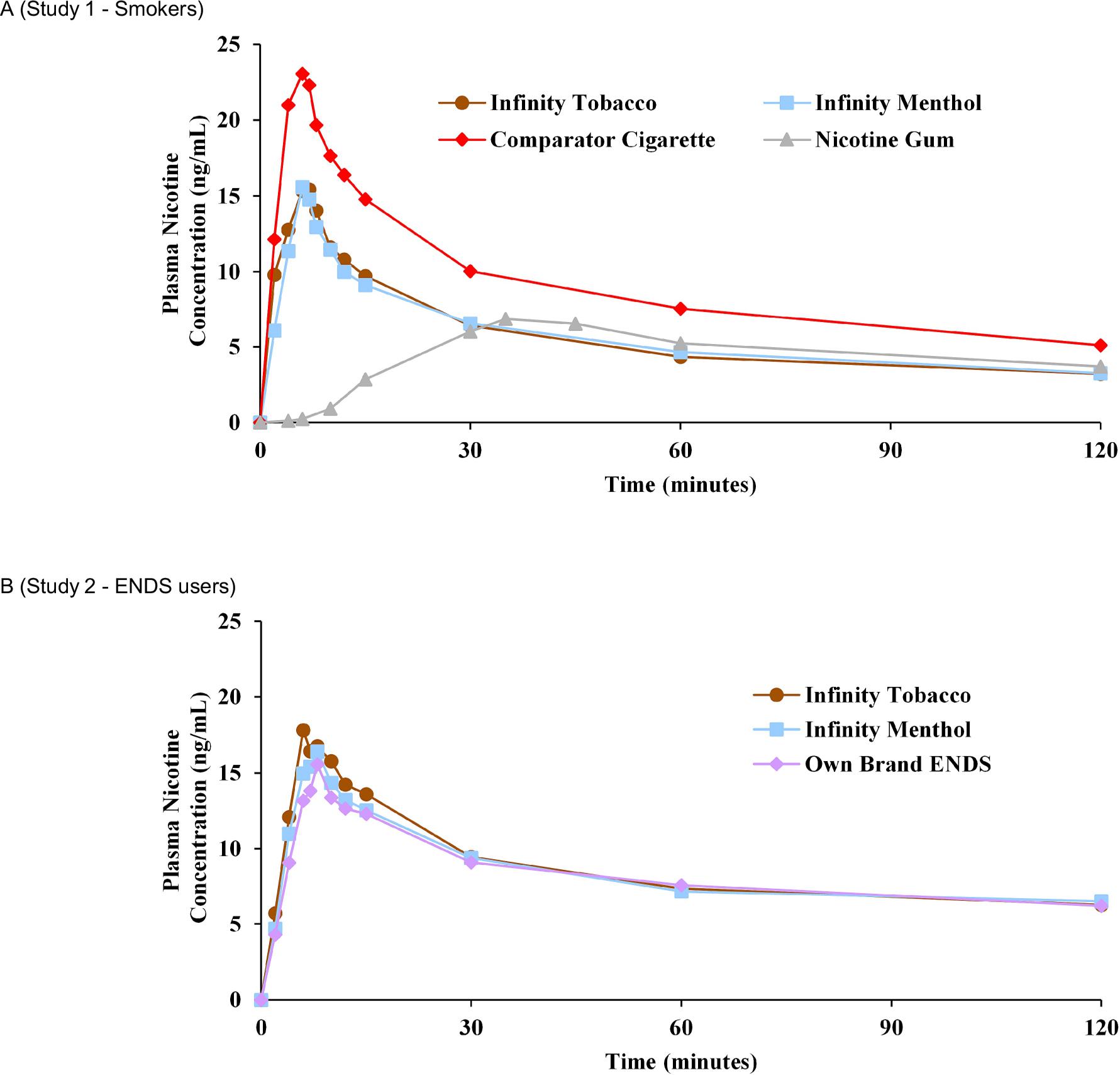
Mean baseline-adjusted plasma nicotine concentration-time profiles in (a) smokers (Study 1) and (b) ENDS users (Study 2). Error bars have been removed for clarity; for variability estimates refer to Table 2.
Baseline-adjusted plasma nicotine pharmacokinetic parameters by study and product.
| Parameter (units) | Study 1 - Smokers | Study 2 - ENDS Users | |||||
|---|---|---|---|---|---|---|---|
| Infinity Tobacco | Infinity Menthol | Usual brand cigarette | Nicotine gum | Infinity Tobacco | Infinity Menthol | Usual brand ENDS | |
| N | 35 a | 34 | 37 b | 37 c | 27 d | 25 e | 25 f |
| Cmax(ng/mL) | 18.5 (100.2%) | 16.6 (84.9%) | 27.0 (60.5%) | 7.5 (56.2%) | 21.2 (72.5%) | 18.2 (51.4%) | 16.8 (79.7%) |
| Tmax(min) | 6.0 (2.0, 15.0) | 6.0 (2.0, 120.0) | 7.0 (2.0, 12.0) | 35.0 (15.0,122.0) | 8.0 (4.0, 123.0) | 8.0 (4.0, 123.0) | 8.0 (4.0, 28.0) |
| AUC(0–15)(ng×min/mL) | 171.6 (88.3%) | 153.5 (80.2%) | 246.00 (50.6%) | 12.1 (102.3%) | 190.2 (64.4%) | 173.5 (51.5%) | 160.4 (66.2%) |
| AUC(0–120)(ng×min/mL) | 676.5 (76.2%) | 634.1 (76.8%) | 1074.8 (31.9%) | 530.7 (59.7%) | 1046.2 (54.5%) | 990.9 (52.0%) | 1008.1 (57.2%) |
Data are presented as means (CV) for Cmax, AUC(0–15) and AUC(0–120), and median (minimum, maximum) for Tmax.
N = 34 for AUC(0–15) and AUC(0–120)
N = 36 for AUC(0–15) and AUC(0–120)
N = 35 for AUC(0–120)
N = 26 for AUC(0–15) and AUC(0–120)
N = 24 for AUC(0–15) and AUC(0–120)
N = 24 for AUC(0–15) and N = 23 for AUC(0–120)
Abbreviations:
area under the nicotine concentration-time curve calculated from time zero to 15 minutes; area under the nicotine concentration-time curve calculated from time zero to 120 minutes; confidence interval; maximum observed plasma concentration over the duration of the measurement interval after time zero; coefficient of variation; least square means; number of observations; time of maximum observed plasma nicotine concentration.
Statistical comparison of baseline-adjusted plasma nicotine pharmacokinetic parameters between Infinity Tobacco and Infinity Menthol and comparator products. Statistically significant p values are shown in bold text.
| Infinity Tobacco vs comparator | Infinity Menthol vs comparator | |||||
|---|---|---|---|---|---|---|
| Geometric LSmeans Ratio (%) | 90% CI (%) | p value | Geometric LSmeans Ratio (%) | 90% CI (%) | p value | |
| Usual brand cigarette (Study 1) | ||||||
| Cmax (ng/mL) | 48.3 | 35.74–65.19 | 0.0001 | 45.2 | 33.36–61.28 | < 0.0001 |
| AUC(0–15) (ng×min/mL) | 47.4 | 34.13–65.92 | 0.0003 | 44.5 | 31.99–61.86 | < 0.0001 |
| AUC(0–120) (ng×min/mL) | 45.5 | 34.95–59.20 | < 0.0001 | 43.0 | 33.02–56.03 | < 0.0001 |
| Tmax (min) | 0.8 (−0.5–2.5) | 0.00–1.50 | 0.0833 | 0.0 (−1.5–1.0) | −1.00–1.00 | 0.8504 |
| Nicotine gum (Study 1) | ||||||
| Cmax (ng/mL) | 185.6 | 137.31–250.99 | 0.0010 | 173.9 | 128.31–235.66 | 0.0032 |
| AUC(0–15) (ng×min/mL) | 1426.1 | 1027.58–1979.30 | < 0.0001 | 1337.5 | 964.61–1854.61 | < 0.0001 |
| AUC(0–120) (ng×min/mL) | 107.1 | 82.05–139.68 | 0.6715 | 101.2 | 77.55–132.16 | 0.9393 |
| Tmax (min) | −30.0 (−34.0–−26.0) | −33.00–−27.00 | < 0.0001 | −32.5 (−36.0–−27.0) | −34.00–−28.50 | < 0.0001 |
| Usual brand ENDS (Study 2) | ||||||
| Cmax (ng/mL) | 109.3 | 88.71–134.65 | 0.4784 | 109.4 | 88.45–135.20 | 0.4829 |
| AUC(0–15) (ng×min/mL) | 104.7 | 83.93–130.55 | 0.7295 | 107.5 | 86.08–134.23 | 0.5874 |
| AUC(0–120) (ng×min/mL) | 98.2 | 83.79–115.05 | 0.8466 | 103.2 | 87.98–121.08 | 0.7405 |
| Tmax (min) | 0.0 (−2.5–3.0) | −2.00–2.50 | 0.9053 | −0.5 (−3.0–5.5) | −2.50–3.00 | 0.7752 |
The mixed-effect model included product, sex, day and sequence as fixed effects, and subject as a random effect. For each geometric least-squares mean, the ln-transformed estimate of the least-squares mean was exponentiated. For Cmax and AUC, the ln-transformed estimate of the least-squares mean difference was exponentiated and multiplied by 100 to obtain the geometric mean ratio and corresponding 90% CI. For Tmax, statistical significance was assessed using Wilcoxon signed-rank test.
In ENDS users, the plasma nicotine concentration-time profiles were similar for Infinity Tobacco ENDS, Infinity Menthol ENDS, and usual brand ENDS (Figure 2B). Mean [CV] peak plasma nicotine concentrations (Cmax) were 21.2 [72.5%] ng/mL for Infinity Tobacco, 18.2 [51.4%] ng/mL for Infinity Menthol, and 16.8 [79.7%] ng/mL for usual brand ENDS (Table 2). Median Tmax values were 8 min for all ENDS products, and both AUC(0–15) and AUC(0–120) values were similar across the study ENDS products (Table 2). Statistical analyses (Table 3) showed no significant differences in any nicotine pharmacokinetic parameters between either of the Infinity ENDS flavors and usual brand ENDS.
In parallel with the rise in plasma nicotine levels during study product use, all study products elicited robust reductions in urge to smoke (Figure 3A) or urge to vape (Figure 3B). In smokers, the largest maximum reduction in urge to smoke, based on responses on a 100-mm VAS scale, was seen when subjects smoked one of their usual brand cigarettes (mean [CV] Emax_R was −60.5 [31.41%]; Table 4). Reductions in urge to smoke elicited by the use of either Infinity ENDS flavor were still substantial but approximately 10–20% lower than that elicited by cigarette smoking (mean [CV] was −49.2 [37.57%] for Infinity Tobacco ENDS and −53.0 [32.29%] for Infinity Menthol ENDS, and use of nicotine gum caused the lowest mean reduction in urge to smoke (−48.2 [33.83%]; Table 4). The area over the effect-time curve parameter AOE(0–15) followed a similar pattern to Emax_R, with cigarettes eliciting the biggest effect, Infinity ENDS use causing a lower effect, and nicotine gum eliciting the lowest effect. For AOE(0–120), cigarettes elicited the biggest effect and the values for Infinity Tobacco ENDS, Infinity Menthol ENDS, and nicotine gum, were comparable (Table 4). Regarding the speed of onset of urge reduction, the median TEmax_R value was lowest for Infinity Menthol ENDS (5 min), identical for Infinity Tobacco ENDS and usual brand cigarettes (10 min), and highest for nicotine gum (30 min; Table 4). Statistical analysis of Emax_R data (Table 5) showed that the reduction in urge to smoke was significantly greater (p < 0.05) for usual brand cigarettes than either of the two Infinity ENDS flavors, and also that there was no significant difference (p > 0.05) between either of the Infinity ENDS flavors and nicotine gum. For TEmax_R, there was no significant difference (p > 0.05) between either Infinity ENDS flavor and usual brand cigarettes, while the differences between both Infinity ENDS flavors and nicotine gum were statistically significant (p < 0.05; Table 5).
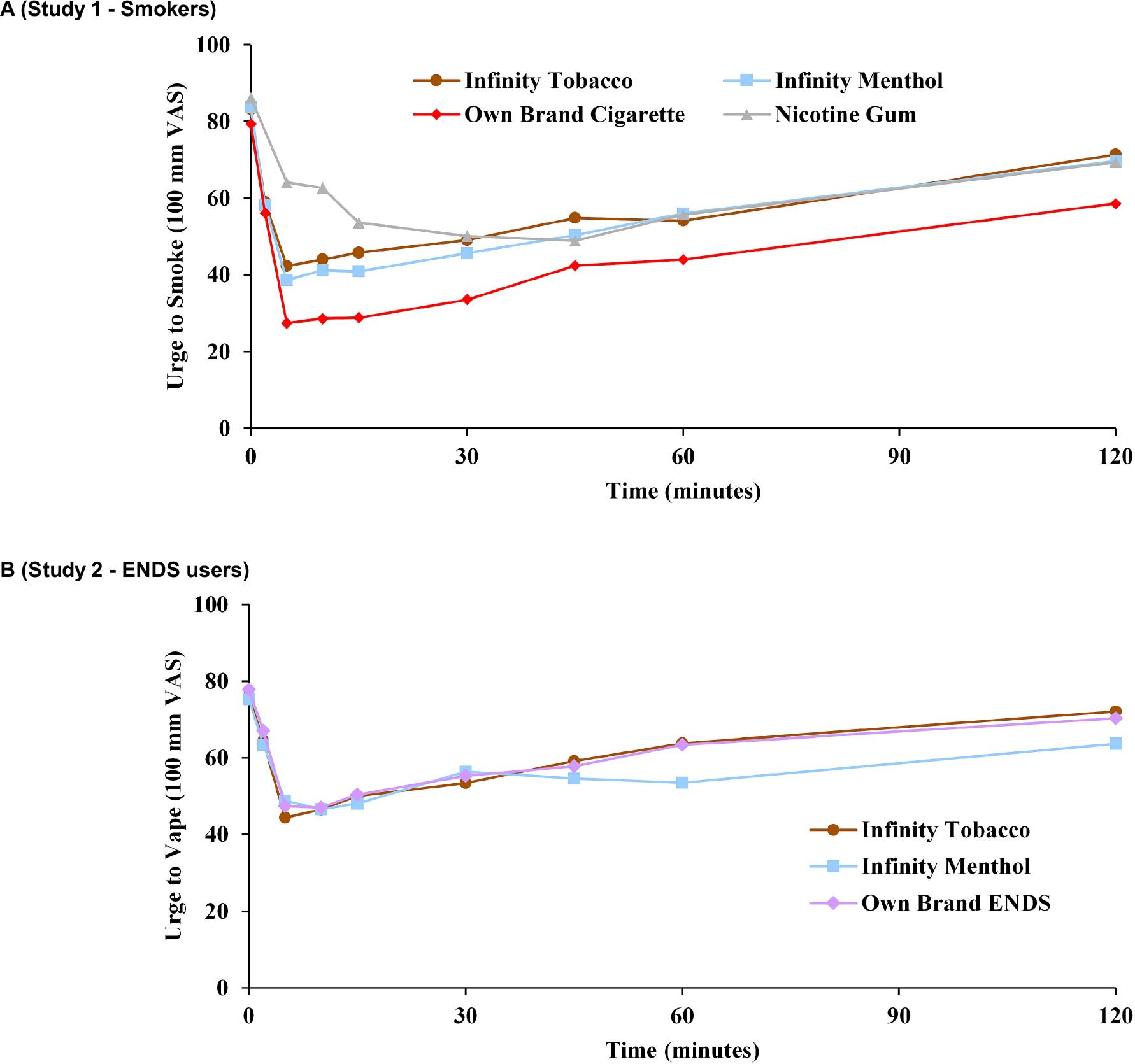
Mean urge to smoke/vape VAS scores over time profiles in (a) smokers (Study 1) and (b) ENDS users (Study 2). Error bars have been removed for clarity; for variability estimates refer to Table 4.
Subjective effects questionnaires by study and product.
| Study 1 - Smokers | Study 2 - ENDS Users | ||||||
|---|---|---|---|---|---|---|---|
| Infinity Tobacco | Infinity Menthol | Usual brand cigarette | Nicotine gum | Infinity Tobacco | Infinity Menthol | Usual brand ENDS | |
| Urge to smoke/vape [mean (SD)] a | |||||||
| N | 38 | 38 b | 38 | 37 | 29 c | 28 d | 25 |
| Emax_R | −49.2 (37.57) | −53.0 (32.29) | −60.5 (31.41) | −48.2 (33.83) | −41.9 (28.32) | −36.8 (29.20) | −43.2 (29.52) |
| TEmax_R | 10.0 (2, 60) | 5.0 (2, 120) | 10.0 (2, 120) | 30.0 (5, 120) | 5.0 (2, 60) | 10.0 (2, 120) | 5.0 (2, 120) |
| AOE(0–15) | −8.3 (8.57) | −9.3 (6.84) | −10.4 (7.22) | −4.8 (5.58) | −6.1 (5.98) | −5.6 (6.61) | −5.8 (5.76) d |
| AOE(0–120) | −52.2 (72.28) | −56.5 (49.92) | −69.1 (65.39) | −54.0 (48.46) | −28.1 (49.20) | −38.4 (54.30) | −32.8 (39.34) |
| Modified product evaluation scale [mean (SD)] | |||||||
| N | 39 | 39 | 38 | 36 | 29 | 28 | 26 |
| Satisfaction | 3.5 (1.43) | 3.8 (1.62) | 5.2 (1.63) | 2.9 (1.19) | 3.8 (1.78) | 4.6 (1.58) | 4.5 (1.86) |
| Psychological reward | 3.1 (1.38) | 3.3 (1.26) | 4.1 (1.46) | 2.5 (1.10) | 3.2 (1.54) | 3.7 (1.68) | 3.6 (1.76) |
| Aversion | 1.4 (0.46) | 1.6 (0.63) | 1.4 (0.67) | 1.8 (0.96) | 1.7 (1.00) | 1.7 (1.35) | 1.7 (0.85) |
| Relief | 4.2 (1.44) | 4.3 (1.45) | 5.6 (1.20) | 3.5 (1.49) | 4.2 (1.48) | 4.8 (1.35) | 4.2 (1.64) |
| Concerned for dependence | 1.9 (1.48) | 1.9 (1.34) | 3.6 (2.25) | 1.5 (0.81) | 2.4 (1.70) | 2.3 (2.09) | 2.2 (1.58) |
| Product liking [mean (SD)] | |||||||
| N | 38 | 38 | 38 | 37 | 29 | 28 | 25 |
| Emax | 56.2 (32.40) | 59.6 (35.59) | 89.2 (17.15) | 47.3 (29.64) | 63.8 (32.91) | 77.5 (23.95) | 74.4 (25.49) |
| Future intent to use | |||||||
| N | 39 | 39 | 38 | 36 | 29 | 28 | 26 |
| Mean (SD) | 53.2 (33.26) | 51.8 (37.32) | 81.7 (24.69) | 37.6 (34.15) | 55.6 (36.27) | 76.5 (28.19) | 68.8 (32.99) |
| Frequency Counts | |||||||
| 0–49, n (%) | 13 (33.3) | 14 (35.9) | 4 (10.5) | 17 (43.6) | 11 (37.9) | 5 (17.2) | 7 (26.9) |
| 50, n (%) | 5 (12.8) | 3 (7.7) | 0 (0) | 2 (5.1) | 2 (6.9) | 2 (6.9) | 1 (3.8) |
| 51–100, n (%) | 21 (53.8) | 22 (56.4) | 34 (89.5) | 17 (43.6) | 16 (55.2) | 21 (72.4) | 18 (69.2) |
Data for TEmax_R values are presented as median (minimum, maximum).
N = 37 for AOE(0–15)
N = 28 for AOE(0–15)
N = 26 for AOE(0–15)
Abbreviations:
area over the effect-time curve relative to pre-product use from time zero to the relevant time point; maximum effect among all the post-product use assessments over the duration of the measurement interval; maximum reduction post-product use from pre-product use score over the duration of the measurement interval; number of observations; standard deviation; time of the maximum reduction in response over the duration of the measurement interval.
Statistical comparisons of subjective effects measures between Infinity Tobacco and Infinity Menthol and comparator products. Statistically significant p values are shown in bold text.
| Infinity Tobacco vs comparator | Infinity Menthol vs comparator | |||||
|---|---|---|---|---|---|---|
| Difference | 95% CI (%) | p value | Difference | 95% CI (%) | p value | |
| Usual brand cigarette (Study 1) | ||||||
| Urge to smoke Emax_R | 13.4 (5.35) a | 2.7–24.0 | 0.0142 | 11.8 (5.34) a | 1.2–22.3 | 0.0300 |
| Urge to smoke TEmax_R | 0.0 (−6.5–5.0) b | −4.00–4.00 | 1.0000 | 0.0 (−8.0–12.5) b | −6.00–5.00 | 0.9920 |
| mPES Satisfaction | −1.6 (0.29) a | −2.2–−1.1 | <0.0001 | −1.4 (0.29) a | −1.9–−0.8 | <0.0001 |
| mPES Psychological reward | −0.9 (0.22) a | −1.4–−0.5 | <0.0001 | −0.7 (0.22) a | −1.2–−0.3 | 0.0018 |
| mPES Relief | −1.4 (0.26) a | −1.9–−0.9 | <0.0001 | −1.3 (0.26) a | −1.9–−0.8 | <0.0001 |
| mPES Aversion | 0.3 (−0.50–0.63) c | −0.25 – 0.50 | 0.3075 | 0.2 (0.119) d | −0.04 – 0.44 | 0.1045 |
| mPES Concern for dependence | −1.6 (0.30) d | −2.25–−1.02 | <0.0001 | −1.7 (0.30) d | −2.26–−1.06 | <0.0001 |
| Product liking | −23.00 (−58.00–−12.00) c | −49.00–−15.00 | <0.0001 | −22.00(−61.00–−5.00) c | −33.00–−8.00 | <0.0001 |
| Future intent to use | −27.6 (6.66) d | −41.12–−14.15 | 0.0002 | −23.0 (−49.00–−1.00) c | −34.00–−4.00 | 0.0012 |
| Nicotine gum (Study 1) | ||||||
| Urge to smoke Emax_R | −6.0 (5.39) a | −16.6–4.7 | 0.2725 | −7.6 (5.36) a | −18.2–3.1 | 0.1611 |
| Urge to smoke TEmax_R | −22.5 (−39.0–−10.0)b | −32.50–−14.00 | <0.0001 | −17.5 (−34.0–−4.0) b | −28.00–−7.50 | 0.0006 |
| mPES Satisfaction | 0.6 (0.29) a | 0.1–1.2 | 0.0336 | 0.9 (0.29) a | 0.3–1.5 | 0.0026 |
| mPES Psychological reward | 0.6 (0.23) a | 0.1–1.0 | 0.0169 | 0.8 (0.23) a | 0.3–1.2 | 0.0009 |
| mPES Relief | 0.7 (0.27) a | 0.2–1.3 | 0.0070 | 0.8 (0.27) a | 0.3–1.3 | 0.0040 |
| mPES Aversion | −0.3 (−1.13–0.25) c | −0.75–0.25 | 0.1516 | −0.2 (0.180) d | −0.56–0.17 | 0.2912 |
| mPES Concern for dependence | 1.0 (1.00–3.00) c | −1.00–4.00 | 0.0923 | 1.0 (0.00 – 2.00) c | 1.00–2.00 | 0.0768 |
| Product liking | 9.08 (5.875) d | −2.843–21.010 | 0.1311 | 11.81 (6.603) d | −1.580–25.202 | 0.0821 |
| Future intent to use | 16.9 (8.42) d | −0.17–34.05 | 0.0522 | 15.1 (8.86) d | −2.90–33.12 | 0.0972 |
| Usual brand ENDS (Study 2) | ||||||
| Urge to vape Emax_R | −0.8 (4.22) a | −9.3–7.7 | 0.8451 | 2.6 (4.24) a | −5.9–11.1 | 0.5427 |
| Urge to vape TEmax_R | 0.0 (−5.0–15.0) b | −4.00–14.00 | 0.8434 | 4.0 (−1.5–13.0) b | −1.50–12.50 | 0.1706 |
| mPES Satisfaction | −0.8 (0.33) a | −1.4–−0.1 | 0.0238 | 0.0 (0.34) a | −0.6–0.7 | 0.9421 |
| mPES Psychological reward | −0.40 (−1.20–0.40) c | −1.200–0.400 | 0.3833 | 0.20 (−0.60–0.80) c | −0.600–0.800 | 0.8145 |
| mPES Relief | 0.01 (0.313) d | −0.636–0.652 | 0.9806 | 0.20 (−0.80–1.00) c | −0.400–0.800 | 0.6776 |
| mPES Aversion | 0.05 (0.272) d | −0.512–0.608 | 0.8610 | −0.25 (−0.75–0.63) c | −0.750–0.500 | 0.8238 |
| mPES Concern for dependence | −0.15 (0.336) d | −0.846–0.538 | 0.6510 | −1.00 (−2.50–2.00) c | −3.000–3.000 | 0.3877 |
| Product liking Emax | −11.9 (6.85) a | −25.6–1.9 | 0.0885 | 1.8 (6.89) a | −12.0–15.6 | 0.7946 |
| Future intent to use | −13.5 (6.82) d | −27.58–0.50 | 0.0581 | 3.0 (−3.00–11.00) c | −3.00–11.00 | 0.8318 |
LSmeans difference (standard error), 95% confidence interval, and p value from the linear mixed-effects model that included product, sex, day and sequence as fixed effects, and subject as a random effect.
Median of the paired difference (quartile 1–quartile 3) and 95% confidence interval from the Hodges-Lehmann test for paired differences and p value from the Wilcoxon signed-rank test.
The sign test was used to assess the difference between the two products, with the median of the paired difference (quartile 1–quartile 3), 95 % confidence interval, andp value presented.
A paired t-test was used to assess the difference between the two products, with the mean difference (standard error), 95% confidence interval, and p value presented.
Abbreviations:
confidence interval; maximum effect among all the post-product use assessments over the duration of the measurement interval; maximum reduction post-product use from pre-product use score over the duration of the measurement interval; mPES modified Product Evaluation Scale; number of observations; standard deviation; time of the maximum reduction in response over the duration of the measurement interval.
In the ENDS users, the magnitude of the mean [CV] maximum reduction in urge to vape (Emax_R) was similar across study products, ranging from 36.8 [29.20%] for Infinity Menthol ENDS to 43.2 [29.52%] for subjects’ usual brand ENDS (Table 4). TEmax_R, AOE(0–15) and AOE(0–120) were also similar across the study products in the ENDS users. Statistical analyses showed no significant differences (p > 0.05) when comparing either of the Infinity ENDS flavors with usual brand ENDS for both Emax_R and TEmax_R (Table 5).
In smokers, mean composite subscale mPES scores for satisfaction, psychological reward and relief, and the single-item score for being concerned about dependence, were highest for subjects’ usual brand cigarettes, lower for both Infinity ENDS flavors, and lowest for nicotine gum (Table 4). These differences in composite scores were statistically significant for the comparisons between Infinity Tobacco ENDS and Infinity Menthol ENDS and both usual brand cigarettes and nicotine gum (Table 5). For the concerned about dependence single item, differences were statistically significant between both Infinity Tobacco ENDS and Infinity Menthol ENDS and usual brand cigarettes, but not between either Infinity ENDS flavor and nicotine gum (Table 5). For the composite mPES score for aversion, nicotine gum was rated as the most aversive and with lower aversion reported for both the Infinity ENDS flavors and usual brand cigarettes (Table 4). However, none of the between-product comparisons for aversion were statistically significant (Table 5).
In the ENDS users, mean composite scores for both satisfaction and psychological reward were similar for Infinity Menthol ENDS and usual brand ENDS, and lower for Infinity Tobacco ENDS (Table 4). These differences were statistically significant for satisfaction for the comparison between Infinity Tobacco ENDS and usual brand ENDS, but not statistically significant between Infinity Menthol ENDS and usual brand ENDS (Table 5). Differences in psychological reward scores were not statistically significant between either Infinity Tobacco or Infinity Menthol ENDS and usual brand ENDS (Table 5). For the relief composite mPES score, mean values were similar for Infinity Tobacco ENDS and usual brand ENDS, and higher for Infinity Menthol ENDS (Table 4), though the differences were not significantly different between either Infinity ENDS flavor and usual brand ENDS (Table 5). Single-item scores for being concerned about dependence and the composite aversion scores were similar for all study products were slightly higher than the mean score for nicotine gum (Table 4). For psychological reward, aversion, relief, and concerned about dependence, there were no significant differences between either Infinity Tobacco ENDS or Infinity Menthol ENDS and usual brand ENDS (Table 5).
In smokers, mean maximum product liking (PL) VAS scores were highest for usual brand cigarettes, lower and comparable for both the Infinity ENDS flavors, and lowest for nicotine gum (Table 4). The differences between either Infinity ENDS flavor and usual brand cigarettes were statistically significant, but there was no significant difference in maximum PL between either Infinity ENDS flavor and nicotine gum (Table 5). In ENDS users, mean maximum PL was highest for Infinity Menthol ENDS, slightly lower for usual brand ENDS, and lowest for Infinity Tobacco ENDS (Table 4). However, the were no statistically significant differences between either Infinity ENDS flavor and usual brand ENDS (Table 5).
In cigarette smokers, mean FIU scores were highest for subjects’ usual brand cigarettes, lower and comparable for both Infinity Tobacco ENDS and Infinity Menthol ENDS, and lowest for nicotine gum (Table 4). Differences were statistically significant between both Infinity ENDS flavors, and subjects’ usual brand cigarettes, but not nicotine gum (Table 5). In ENDS users, mean FIU scores were highest for Infinity Menthol ENDS, lower for usual brand ENDS, and lowest for Infinity Tobacco ENDS (Table 4). However, there were no significant differences in FIU scores between either Infinity ENDS flavor and usual brand ENDS (Table 5).
The study products were well-tolerated under the conditions of use during the studies. Use of both Infinity ENDS flavors and combustible cigarettes caused transient and minor increases in physiologic endpoints (systolic and diastolic BP and HR), during the PK Sessions. The effects on systolic BP and HR were similar between subject’s usual brand cigarettes and both Infinity ENDS flavors, and lower for nicotine gum, while the effects on systolic blood pressure and heart rate were similar between subject’s usual brand ENDS and both Infinity ENDS flavors. In both studies, all physiologic endpoint parameters remained within normal ranges.
Regarding AEs, 21 cigarette smokers (51.2%) experienced a total of 40 product use emergent adverse events (PEAEs), of which 33 were considered product related (categorized as possibly, probably, or likely). The incidence of subjects with product related PEAEs was highest for Infinity Menthol ENDS and nicotine gum (both 20.5%), followed by usual brand cigarettes (13.2%) and then Infinity Tobacco ENDS (2.6%).
Eleven ENDS users (37.9%) experienced a total of 25 PEAEs, with 19 considered as product-related. The incidence of subjects with product-related PEAEs was highest for Infinity Tobacco (ENDS 20.7%) followed by Infinity Menthol ENDS (17.2%) and subjects’ usual brand ENDS (7.1%).
In both studies, the most common PEAEs were classified as nervous system disorders (e.g., headache, dizziness, presyncope) or gastrointestinal disorders (e.g., nausea). There were no serious or severe PEAEs during either study. No subject in either study was withdrawn or discontinued the study because of a PEAE.
Central to assessing the ability of a novel ENDS product to support smokers to switch away from harmful cigarette smoking is an assessment of its abuse liability. While there is no documented and agreed approach to assessing the abuse liability of ENDS products, it is generally considered that assessing the pharmacological effects of the product, i.e., its ability to deliver nicotine, and its subjective properties in areas such as satisfaction, liking, and intent to use, can be integrated to provide an abuse liability assessment (27, 30) and also to provide an overall assessment of the ability of a product to help smokers switch (43, 49, 50). In the study described in this paper assessing nicotine pharmacokinetics and subjective effects in smokers, nicotine delivery from two flavors (tobacco and menthol) of the Infinity ENDS was found to be substantial but lower than that from combustible cigarettes, and higher and more rapid than that from nicotine gum. Due to the general view that the faster absorption (shorter Tmax) or greater amounts of nicotine (Cmax and/or AUC) gives rise to a higher abuse liability potential (31, 32), this suggests that the Infinity ENDS has a lower abuse liability than cigarettes but a higher abuse liability than nicotine gum. This finding is supported by the subjective effects data in domains such as satisfaction, psychological reward, relief, product liking, and future intent to use, which, similar to nicotine delivery, also showed effects intermediate to those of combustible cigarettes and nicotine gum. Taken together, this intermediate abuse liability suggests that the Infinity ENDS has strong potential for helping smokers switch away from cigarette smoking and is likely greater than that of nicotine gum.
These conclusions are in accordance with other findings reported in the literature. STILES et al. (35, 37) reported findings from 2 studies similar to Study 1 described in this paper in which nicotine pharmacokinetics and subjective effects of the Vuse Solo ENDS were assessed in smokers. In these studies, nicotine delivery in subjects using either tobacco- or menthol-flavored ENDS were remarkably similar, as was the case in Study 1, and lower than that seen when subjects smoked combustible cigarettes. A comparison with nicotine gum was also made in these studies (35, 37) and although Cmax was similar for the nicotine gum compared with the Vuse Solo ENDS, Tmax was significantly shorter for the ENDS products. STILES et al. also demonstrated that use of the Vuse Solo ENDS reduced urges to smoke and elicited liking and intent to use again, which in all cases was not to the same degree as cigarette smoking (35, 37) but was higher than nicotine gum. A more recent study assessing nicotine pharmacokinetics and subjective effects during use of a newer tobacco-flavored variant of the Vuse Solo ENDS also reported abuse liability as intermediate between combustible cigarettes and nicotine gum (44). The newer Vuse Solo ENDS variant also reduced urges to smoke and elicited subjective effects of product liking and intent to use again, though as in both the previous studies on Vuse Solo ENDS (35, 37), and this study on the Infinity ENDS, these effects were lower than those elicited by cigarette smoking and greater than those seen during nicotine gum use (44).
In addition, GOLDENSON et al. reported data from 2 abuse liability studies assessing the impact of e-liquid nicotine concentration (41) and flavor (40) on nicotine pharmacokinetics and subjective effects in smokers using the JUUL ENDS. In both studies, combustible cigarettes and nicotine gum were used as comparator products. Generally speaking, the abuse liability of JUUL ENDS was found to be between that of combustible cigarette smoking and nicotine gum use. Abuse liability was influenced by the e-liquid nicotine concentration with the abuse liability of a 5% nicotine e-liquid higher than that of a 3% e-liquid (41). Both nicotine concentrations did however give rise to robust nicotine delivery (similar to Infinity ENDS, Cmax was approximately two thirds that of the Cmax from combustible cigarettes for 5% nicotine in JUUL ENDS) and elicited positive subjective effects such as liking, intent to use again, satisfaction, enjoyment, and relief. In the second study (40) and similar to the study reported in this paper, e-liquid flavor was found to have little impact on abuse liability since both nicotine delivery and subjective effects were similar regardless of the e-liquid flavor used. Of importance, both the JUUL study (40) and our assessment of the Infinity ENDS described evidence for a continuum of abuse liability, with combustible cigarettes > ENDS > nicotine gum.
It is worthwhile placing the findings of the current study assessing the abuse liability of the Infinity ENDS into the broader public context. The overall impact of an ENDS product in population-level public health is driven by two main factors; its ability to support smoking in switching away from harmful cigarette smoking, and whether it creates an initiation or addiction risk for nicotine non-users (14, 51, 52). As described above, the data from Study 1 concerning nicotine delivery and subjective effects among smokers suggest strong potential for Infinity ENDS to displace cigarettes in current smokers. It is noteworthy in this regard that for the JUUL ENDS, higher nicotine delivery due to higher e-liquid nicotine concentrations (41, 43) is associated with higher switching rates (53). The counterbalance to this positive public health impact is the potential for a negative impact caused by the initiation of sustained use by nicotine non-users (51). The lower abuse liability of the Infinity ENDS compared with combustible cigarettes suggests that it is less likely to induce strong dependence or addiction than combustible cigarettes which deliver nicotine very effectively and are extremely harmful to health. In this regard, the comments made by FDA in the awarding of a marketing order under the PMTA program for Vuse Solo ENDS are notable. In the Technical Project Lead Review of the Vuse Solo PMTA (54), regarding the potential for initiation FDA stated that “The nicotine levels may pose an addiction risk for non-tobacco users; however, the risk is no higher than other currently available tobacco products due to relatively low abuse liability of the new products” and further that “the comparably low abuse liability of the new products relative to combusted cigarettes suggests initiation and sustained use of the new products among tobacco non-users is likely to be lower than initiation and sustained use of tobacco products with greater abuse liability (e.g., combusted cigarettes)”. Overall, the findings from Study 1 support the potential for a positive role of the Infinity ENDS in tobacco harm reduction, by providing an acceptable alternative to combustible cigarettes among current smokers while presenting a low initiation/addiction risk among nicotine non-users. Among current ENDS users in Study 2, the data described in this paper demonstrate comparable nicotine delivery and generally similar subjective effects, and therefore abuse liability, as subjects’ usual brand ENDS. This suggests that the Infinity ENDS could provide a suitable substitute for the ENDS that users currently use, and therefore support continued ENDS use while presenting no higher degree of abuse liability. Since the vast majority of ENDS users are either ex-smokers or dual users (55, 56), this could be important in maintaining either partial or complete switching and preventing relapse back to cigarette smoking. This is likely to add to the potential overall public health benefit of the Infinity ENDS. It is also notable that nicotine delivery in the ENDS users in Study 2 were higher than that in smokers in Study 1, although no between-study statistical comparisons were made. This reinforces the notion that ENDS users may change their use behavior over time as they transition from cigarette smoking to accustomed ENDS use (57), and is similar to the previously-reported difference in nicotine delivery between naïve and experienced ENDS users (58). The studies and the findings described in this paper must be viewed in terms of both strengths and limitations. A major strength of both studies is our rigorous assessment of the abuse liability of the Infinity ENDS in comparison either to both cigarettes and nicotine gum (Study 1) or subjects’ usual brand ENDS (Study 2), which were conducted in accordance with consensus standards for nicotine product abuse liability assessments. A further strength was the use of confinement of study subjects at the clinic site throughout the assessment period in order to ensure complete compliance with the study protocol. Limitations include assessment only of a single type of ENDS product, and as such our findings may not be generalizable to other ENDS products either in development or currently marketed. In addition, subjects had a relatively short period of time (8 h) to become acclimated to the test products - a longer acclimation time may have resulted in greater nicotine uptake during the PK session. However, this was also a design feature intended to simulate a brief initial consumer use experience period during which a smoker or ENDS user may determine whether they might continue to use the product.
In summary, we demonstrate through rigorous assessment of nicotine pharmacokinetics and subjective effects that the abuse liability of two flavors of the Infinity ENDS is lower than that of combustible cigarettes but higher than that of nicotine gum, and similar to that of other ENDS products. This supports a potential positive role in tobacco harm reduction, by providing smokers with a satisfying alternative to cigarette smoking which could support their switching away from cigarette smoking to a degree better than the support provided by nicotine gum. Furthermore, our findings in ENDS users support the idea that the Infinity ENDS would be an acceptable substitute for the ENDS products they currently use and may contribute to continued ENDS use and relapse prevention. Finally, the determined lower abuse liability of the Infinity ENDS compared with combustible cigarettes supports that it presents a lower initiation/addiction risk among nicotine non-users than currently marketed tobacco products.