Juvenile idiopathic arthritis (JIA) is the most common form of persistent arthritis in the pediatric population. According to the International League of Associations for Rheumatology, it is an umbrella term, describing the heterogeneous group of arthritis lasting for more than 6 weeks in children below the age of 16 years (Petty et al. 2004). Due to the lack of unequivocal clinical features or laboratory findings, many patients face a significant diagnostic delay, particularly pronounced in the most frequent disease subtype – oligoarthritis. Therefore, new diagnostic markers facilitating the establishment of the diagnosis at the early stages of the rheumatic process are urgently needed. The unmet needs of JIA patients were recently addressed by Pediatric Rheumatology International Trials Organization (PRINTO), which is currently working on a new classification of JIA, facilitating the establishment of the diagnosis and patients’ evaluation in this heterogeneous disease entity (Chen et al. 2023).
The hallmark of JIA pathogenesis is the uncontrolled proliferation of synoviocytes and immunocompetent cells infiltrating the sub-lining layer of the synovium, leading to pannus formation and in consequence intraarticular hypoxia, initiating pathological angiogenesis (Zaripova et al. 2021). As angiogenesis and inflammation are the major mechanisms leading to pannus formation, the key molecules participating in both processes are promising therapeutic targets. Although the role of vascular endothelial growth factor (VEGF) and its soluble receptors (Soluble receptors for vascular endothelial growth factor 1 (sVEGFR-1) and Soluble receptors for vascular endothelial growth factor 2 (sVEGFR-2) has been described in JIA (Świdrowska-Jaros and Smolewska 2018), the reports on novel angiogenesis markers in JIA are scarce.
Semaphorin 5A (SEMA5A), a member of the immune semaphorins family, is involved in various physiological and pathological processes, including both angiogenesis and immune response (Sadanandam et al. 2010). It enhances the inflammatory response by augmentation of T and natural killer (NK) cells proliferation, increase of the secretion of proinflammatory cytokines, and promotion of synoviocytes proliferation (Gras et al. 2014).
Although there are reports on SEMA5A overexpression in the serum, synovial membrane, and synovial fluid of rheumatoid arthritis (RA) patients (Gras et al. 2014), no study has assessed the impact of this protein on the pathogenesis of JIA.
Therefore, study aimed to compare the serum concentration of SEMA5A and VEGF in newly diagnosed JIA patients and sex-and-age-matched healthy controls.
Thirty-five consecutive patients below the age of 16 years with new-onset JIA and 35 age-and-sex-matched healthy controls were qualified for the study. The study group comprised children with all JIA subtypes except for systemic JIA, due to different disease pathogenesis. All children were treatment-naive. One patient and linked control were excluded from the study due to insufficient amount of biologic material obtained. Demographic, laboratory (erythrocyte sedimentation rate [ESR], C-reactive protein [CRP], rheumatoid factor [RF], anti-cyclic citrullinated peptide [anti-CCP], human leukocyte antigen B27 (HLA-B27) antigen, and antinuclear antibodies [ANA] titer), and clinical parameters (disease subtype, number of active and limited joints, and maximal level of inflammation in power-Doppler ultrasound [PDUS], childhood health assessment questionnaire [CHAQ] value, visual analog scale assessed by both patient and physician, and juvenile arthritis disease activity score including 71 joints [JADAS-71] value) were assessed at the study qualification visit, together with collection of the biological material (4.8 mL of full blood) that was stored in −80°C until laboratory analysis. In the control group, laboratory assessment was limited to inflammatory marker values. Clinical and ultrasonographic assessment was performed by experienced pediatric rheumatologist using Toshiba Aplio 400 (Canon Medical Systems Cooperation) ultrasound machine.
Medical University of Lodz Ethical Committee approval (no. RNN/124/23KE) was obtained before commencing the study, and informed written consents were acquired from patients’ legal representatives before enrollment. All the procedures included in this study were in accordance with the Helsinki Declaration.
The concentration of serum SEMA5A and VEGF-A was determined using the ELISA method according to the manufacturer’s protocol. ELISA Kit SEL924Hu (Cloud-Clone, Wuhan, China) was used for the assessment of SEMA5A concentration and ELISA Kit VEGF 650.080.096 (Diaclone, Besancon, France) for VEGF-A.
All statistical calculations were performed using IBM SPSS Statistics software 29.0.20 (International Business Machines Corporation). The Shapiro–Wilk test was used to assess the normality of variables. Continuous variables were compared using the Mann–Whitney U-test or Student’s t-test depending on the normality of the obtained variables. A chi-squared test was carried out to compare categorical variables. The Pearson’s test was used to check for correlation between variables. The Kruskal–Wallis test with post hoc Bonferroni correction was utilized for group comparisons. The values were expressed as mean ± standard deviation (SD) or median with interquartile range (IQR), depending on the data character.
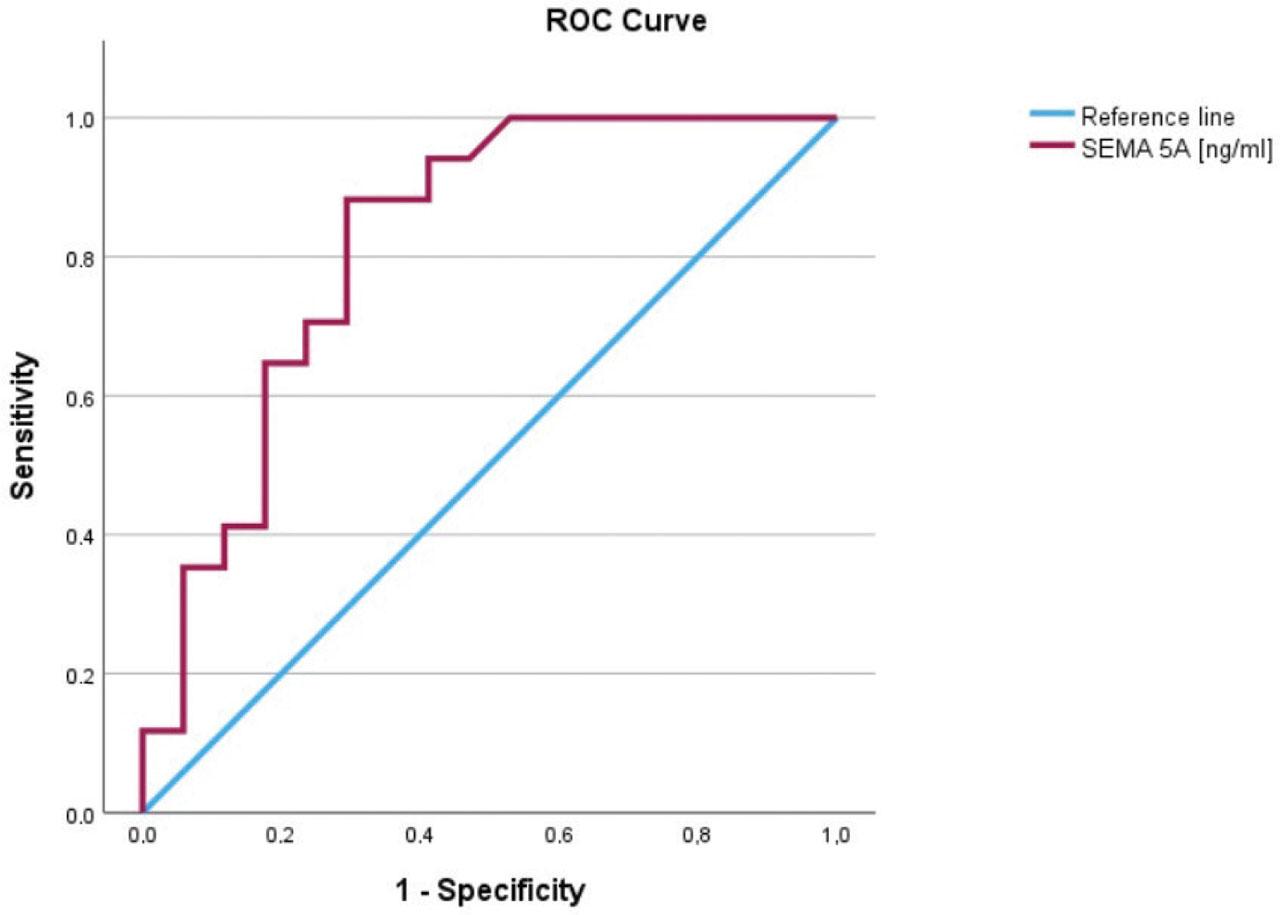
The receiver operating characteristic (ROC) curve was drawn for SEMA5A in the oligoarthritis subgroup, and the area under the curve (AUC) was computed to assess its diagnostic significance. p values <0.05 were considered significant.
Study and control groups comprised 34 patients: 17 boys and 17 girls, with the mean age of 9.75 ± 4.85 years in the study group and 9.89 ± 5.00 years in the control group (p = 0.90; Table 1).
Clinical and laboratory characteristics of study and control groups
| Characteristic | Study group | Control group | p*value | |
|---|---|---|---|---|
| Gender | ||||
| Male (no.) | 17 | 17 | 1.0 | |
| Female (no.) | 17 | 17 | 1.0 | |
| Age (years) | 9.75 (±4.85) | 9.89 (±5.00) | 0.9 | |
| Disease subtype | ||||
| Oligoarticular (%) | 50 | n/a | ||
| Polyarticular seronegative (%) | 11.8 | n/a | ||
| Polyarticular seropositive (%) | 8.8 | n/a | ||
| ERA (%) | 23.6 | n/a | ||
| Psoriatic arthritis (%) | 5.8 | n/a | ||
| Median CRP value (mg/L) | 12.5 | 0.4 | <0.001 | |
| Median ESR value (mm/h) | 34 | 4 | <0.001 | |
| ANA positivity (%) | 88.21 | n/a | ||
| HLA-B27 positivity (%) | 35.23 | n/a | ||
| RF positivity (%) | 8.82 | n/a | ||
| Anti-CCP positivity (%) | 5.88 | n/a | ||
| Mean number of joints with active arthritis (no.) | 3.29 | n/a | ||
| Mean CHAQ value | 0.45 | n/a | ||
| Mean JADAS 71 value | 14.12 | n/a | ||
| Median/mean SEMA5A concentration (ng/mL) in all JIA | 2.04 | 1.34 | 0.002 | |
| In oligoarticular JIA | 1.76 (IQR 1.56) | 0.33 (IQR 1.33) | <0.001 | |
| In polyarticular seronegative JIA | 2.57 (±1.58) | 1.44 | 0.266 | |
| In polyarticular seropositive JIA | 7.57 (±5.26) | 1.61 (±0.54 ng/mL) | 0.123 | |
| In ERA JIA | 1.97 (IQR 1.67) | 1.45 (IQR 1.31) | 0.25 | |
| VEGF-A concentration (pg/mL) | 352.69 (IQR 454.64) | 163.13(IQR 154.54) | <0.01 | |
ANA, antinuclear antibodies; anti-CCP, anti-cyclic citrullinated peptide; CHAQ, Childhood Health Assessment Questionnaire; CRP, C-reactive protein; ERA, enthesitis-related arthritis; ESR, erythrocyte sedimentation rate; HLA, human leukocyte antigen; IQR, interquartile range; JADAS, juvenile idiopathic arthritis disease activity score; JIA, juvenile idiopathic arthritis; n/a,, not applicable; RF, rheumatoid factor; SEMA5A, semaphorin 5A.
In the study cohort, 17 patients (50%) met the diagnostic criteria of oligoarticular JIA, 3 patients (8.8%) were diagnosed with polyarticular seropositive JIA subtype, 4 patients (11.8%) with polyarticular seronegative JIA, 8 (23.6%) with enthesitis-related JIA, and 2 patients (5.8%) with psoriatic arthritis.
The values of basic inflammatory markers were significantly higher in the study group than in the control group, presenting median values 34 mm/h (IQR: 30) in the study group and 4.0 mm/h (IQR: 5) in the control group for ESR (p < 0.001) and 12.5 mg/L (IQR: 33.1) and 0.4 (IQR: 0.1) for CRP (p < 0.001).
The serum concentration of SEMA5A was elevated in JIA patients in comparison to healthy controls with the median value of 2.04 (IQR: 12.41) in JIA patients and 1.34 (IQR: 1.79) in healthy controls (p = 0.002). The difference was statistically significant in oligoarticular JIA, where median SEMA5A concentration equaled 1.76 ng/mL (IQR: 1.56) in comparison to 0.33 ng/mL (IQR: 1.34) in sex-and-age-matched healthy controls (p = 0.001; Figure 1).
Concentration of serum SEMA5A in JIA patients and healthy controls. JIA, juvenile idiopathic arthritis; SEMA5A, semaphorin 5A.
Moreover, it remained significant (p = 0.006) after excluding subjects who would not meet the criteria of the PRINTO-proposed new equivalent of oligoarticular JIA: early-onset ANA positive subtype. Subjects with polyarticular JIA presented higher concentrations of SEMA5A than healthy subjects: 7.57 ± 5.26 ng/mL vs. 1.61 ± 0.54 ng/mL (p = 0.123) for seropositive subtype and 2.57 ± 1.58 ng/mL vs. 1.44 ng/mL (p = 0.266) for the seronegative one. In the enthesitis-related arthritis (ERA) subtype of JIA, SEMA5A did not differ significantly between patients and healthy controls as well: 1.97 ng/mL (IQR: 1.67) vs. 1.45 ng/mL (IQR: 1.31), p = 0.248.
The concentration of VEGF-A was significantly higher in JIA patients than in healthy individuals, reaching the median value of 352.69 pg/mL (IQR: 454.64) in JIA and 163.13 pg/mL (IQR: 154.54) in healthy controls.
Furthermore, we observed a statistically significant strong correlation between the concentration of SEMA5A and VEGF-A (r = 0.807, p < 0.001), despite a lack of correlation between ESR (r = 0.249, p = 0.156) and CRP values (r = 0.095, p = 0.594). There was no correlation between the number of affected joints (r = 0.001, p = 0.988), CHAQ value (r = 0.052, p = 0.770), and JADAS-71 value (r = 0.127, p = 0.475). SEMA5A concentration differed significantly between subgroups of different maximal PDUS activity, reaching a median concentration of 1.76 ng/mL (IQR: 1.54) in the PDUS 1 subgroup, 1.87 ng/mL (IQR: 1.32) in the PDUS 2 subgroup, and 2.46 ng/mL (IQR: 4.42) in the PDUS 3 subgroup (p = 0.018).
SEMA5A differed significantly between JIA-affected girls and their healthy controls (p < 0.001) but not in JIA-affected boys (p = 0.375). There was no association with SEMA5A concentration and the age of the patient (p = 0.058) or presence of HLA-B27 antigen (p = 0.892).
SEMA5A had 75% specificity and 82% sensitivity as a diagnostic marker of oligoarticular JIA for a cut-off level of 0.625 ng/mL with AUC: 0.818 (95% CI: 0.672–0.965; Figure 1 in Supplementary Materials).
Pathological immune response and angiogenesis are the vital components of pannus formation, the key to understand JIA pathogenesis, and therefore a promising target of novel treatment strategies. SEMA5A is a crucial protein in both processes, aggravating angiogenesis via promoting endothelial cell proliferation by activating Met tyrosine kinases (Sadanandam et al. 2010) and enhancing the secretion of proinflammatory cytokines. The role of SEMA5A in immune response has been described by Gras et al. (2014), who reported the protein ability to strongly activate inflammatory T cell and NK cell responses leading to increased secretion of proinflammatory cytokines, including Tumor necrosis factor α (TNF-α), interleukin (IL)-1, IL-6, and IL-8, typically associated with the pathogenesis of both RA and JIA. Moreover, SEMA5A promotes the fibroblast-like synoviocytes pathogenicity by activating phosphoinositide 3-kinase/protein kinase B/mammalian target of rapamycin kinase (PI3K/AKT/mTOR) signaling pathway and inhibiting ferroptosis (Cheng et al. 2022), additionally promoting their proliferation through its unique thrombospondin type-1 domain, facilitating pannus formation, and aggravating joint destruction in the course of RA (Xiao et al. 2021) (Figure 2). The potential of SEMA5A as a target of innovative treatment has been recently described by Qin et al. (2023), who generated SYD12-12, a fully human SEMA5A blocking antibody, effectively inhibiting angiogenesis, synovial hyperplasia, and pannus formation and improving the Treg/Th17 cells imbalance in the collagen-induced arthritis mice model.
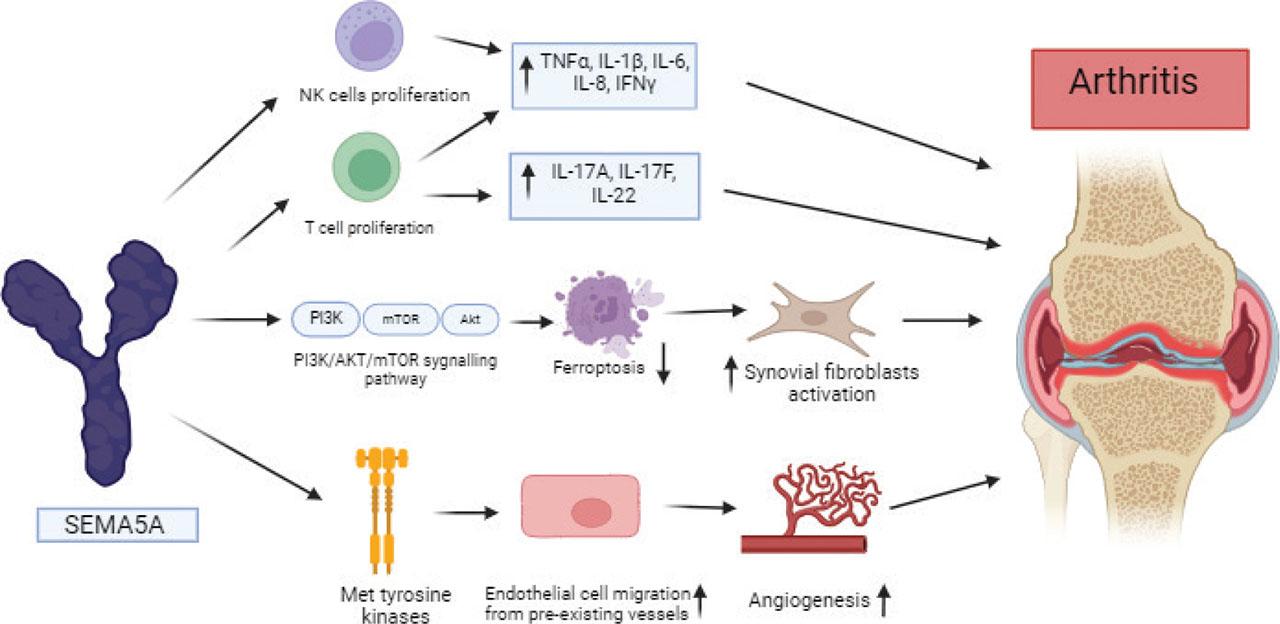
SEMA5A promotes inflammation via different pathways. It increases the proliferation of T and NK cells, leading to higher secretion of proinflammatory cytokines. SEMA5A stimulation leads to activation of synovial fibroblasts by downregulating apoptosis via the PI3K/AKT/mTOR pathway. Moreover, it stimulates angiogenesis by increasing endothelial cell migration from preexisting vessels via activation of Met tyrosine kinases. Created using Biorender (www.biorender.com). AKT, protein kinase B; IFN, interferon; IL, interleukin; mTOR, mammalian target of rapamycin kinase; NK, natural killer; PI3K, phosphoinositide 3-kinase; SEMA5A, semaphorin 5A; TNF, tumor necrosis factor.
Despite the convincing data on the role of SEMA5A in the inflammatory process in the course of RA, to our knowledge and extensive review, no study has addressed the topic of SEMA5A involvement in the course of JIA.
In comparison to RA, JIA is a heterogeneous disease, consisting of several subtypes with different clinical and immunological profiles. This ambiguous character of the disease has been recently addressed by PRINTO, which is currently working on a new JIA classification, reflecting not only the clinical but also a different immunological profile of the disease subtypes. Oligoarticular JIA, which is the most frequent disease manifestation, may be associated only with vague laboratory abnormalities, resulting in the delayed diagnosis and inadequate treatment in the early, crucial phase of the inflammatory process, making the “treat-to-target” treatment strategy inaccessible. Therefore, laboratory markers distinguishing between JIA and healthy subjects not only in the most inflammatory-active disease subtypes as polyarticular seropositive JIA but also in oligoarticular JIA are urgently needed.
In this study, we proved that SEMA5A is involved in the inflammatory process in the course of JIA and may be useful as the disease marker and potentially a target of future treatment. The concentrations of SEMA5A were elevated in all disease subtypes where pathological pannus formation in the key mechanism: polyarticular seropositive JIA (7.57 ± 5.26 ng/mL vs. 1.61 ± 0.54 ng/mL [p = 0.123], polyarticular seronegative JIA (2.57 ± 1.58 ng/mL vs. 1.44 ng/mL [p = 0.266], and oligoarticular JIA 1.76 ng/mL [IQR: 1.56] vs. 0.33 ng/mL [IQR: 1.34], p = 0.001). The lack of statistically significant difference in SEMA5A concentration in polyarticular JIA may be the result of small sample size (n = 3 in polyarticular seropositive JIA) as those disease subtypes appear less frequently than oligoarticular JIA. Given the strong correlation of SEMA5A with anti-CCP and RF levels obtained in previous studies on RA patients (Gras et al. 2014), the topic of SEMA5A concentrations in polyarticular seropositive JIA is a project of high importance, which we aim to address in future studies.
In this study, we also observed a high correlation of SEMA5A with VEGF concentration (r = 0.807, p < 0.001) and a significant difference in SEMA5A concentration in patients with different synovial membrane PDUS activities, indicating the important role of SEMA5A in pathological angiogenesis during the pannus formation.
Although results of this study are promising and open a new perspective on the role of SEMA5A in the pathogenesis of JIA, we acknowledge the limitations of this study. As in the single-center pilot study, the main limitation is the relatively small number of patients included and the fact that they come from the same population. Thus, as JIA is a rare disease, repeating this study in international cohorts is encouraged to verify our findings.
SEMA5A is a promising marker of JIA and a potential therapeutic subject. Future studies are needed to address the exact place of this protein in the pathogenesis of the disease and address the issue of SEMA5A concentration in polyarticular seropositive JIA.