
Tumor necrosis factor (TNF)-α is a dominant inflammatory mediator in the pathogenesis of rheumatoid arthritis (RA) (Weissmann 2006; McInnes and Schett 2011) and is highly expressed in RA synovial fluid. Studies showed that selective blocking of TNF-α alleviates the progression of RA symptoms (Brand et al. 2007; Simsek 2011). Pro-inflammatory TNF acts as an activator of macrophages as well as T and B lymphocytes (Gerriets et al. 2024). It inhibits regulatory T cells and enhances the production of inflammatory cytokines (interleukin-1 [IL]-1, IL-6) and adhesion molecules (intercellular adhesion molecule-1 [ICAM-1], E-selectin). It is also a potent apoptosis inducer. TNF-α rapidly induces the production of matrix metalloproteinases (Sakalyte et al. 2022), which directly contribute to the degradation of cartilage components, including collagen type II (Itoh 2017).
Vitamin D3 (cholecalciferol) is produced in the skin after exposure to sunlight, but it can also be found in certain fish, such as salmon and mackerel. Upon entering the circulation, vitamin D3 is bound to the vitamin D binding protein, which is transported to the liver in this complex. There, vitamin D undergoes hydroxylation to form 25-hydroxyvitamin D (25(OH)D), which is then carried to the kidney for the second hydroxylation to form 1,25-dihydroxyvitamin D (1,25[OH]2D): the hormonal form of vitamin D. The 1,25[OH]2D circulates until it reaches the target cell. Upon entering the cell, vitamin D binds to the vitamin D receptor (VDR) in the cytoplasm. This complex then enters the nucleus and heterodimerizes with the retinoic acid X receptor to increase the transcription of vitamin D-dependent genes (Khazai et al. 2008). Besides its crucial role in calcium and bone metabolism, vitamin D has also been reported to display protective effects against certain autoimmune diseases (Bogaczewicz et al. 2012; Feng et al. 2013; Christakos et al. 2016; Lemke et al. 2021), and it appears to have an anti-inflammatory effect similar to that of anti-TNF drugs. Vitamin D downregulates Th1 cell-mediated immune responses and inhibits the production of pro-inflammatory cytokines, such as TNF-α, interferon (IFN)-γ, IL-6, IL-17, or IL-23 (García-Carrasco and Romero 2015; Sassi et al. 2018). At the same time, the production of cytokines related to Th2 cells as well as anti-inflammatory cytokines is being promoted. These include, e.g., IL-4, IL-5, IL-10, and transforming growth factor-β (El-Fakhri et al. 2014; García-Carrasco and Romero 2015). Vitamin D acts as an immunosuppressant in different biological processes and influences the immune system through a variety of mechanisms. It is involved in numerous immunological interactions, genetic regulation of cytokine production, and VDR expression (Arnson et al. 2007).
It has been verified that RA is one of the human diseases sensitive to vitamin D deficiency, as deficiency is associated with RA susceptibility, higher disease activity, and disability scores (Punceviciene et al. 2021). Moreover, the low serum vitamin D concentration has been linked to genetic variability within the VDR (Sepulveda-Villegas et al. 2020). Previous studies are inconsistent, showing that VDR gene variants are associated with susceptibility to autoimmune connective tissue diseases (Latini et al. 2021), but, on the other hand, they are not linked to RA (Senosi et al. 2022). It seemed that the effect of polymorphisms on RA risk is population-dependent (Bagheri-Hosseinabadi et al. 2020). Despite this, we believe that an analysis of the potential association between VDR single nucleotide polymorphism (SNP) and RA patients treated with anti-TNFs regarding their clinical features may have a significant impact on the evaluation of treatment outcomes.
The study group consisted of 121 RA patients of Caucasian origin. All patients were diagnosed and subjected to anti-TNF therapy (adalimumab, etanercept, infliximab, golimumab, and certolizumab pegol) at the Department of Rheumatology and Internal Medicine, Wrocław Medical University, and the Department of Rheumatology and Connective Tissue, Jan Biziel University Hospital No. 2 in Bydgoszcz, Poland. Together with the RA patients, samples from 122 blood and marrow healthy donors were analyzed as a control group. The healthy individuals have not been diagnosed with any rheumatic or autoimmune disorder or with any other diseases. The inclusion criteria for patients were as follows: consent to participate in the study; confirmed RA based on the 2010 American College of Rheumatology/European League Against Rheumatism (EULAR) classification criteria; active form of the disease: disease activity score 28 (DAS28) >5.1; and age over 18. In turn, exclusion criteria consisted of pregnancy or breastfeeding; coexistence of other systemic diseases of connective tissue besides RA; clinically significant impairment of hepatic or renal function; alcohol abuse; infection with hepatotropic viruses; infections resistant to therapy; ongoing history of cancer if no cure was achieved; uncontrolled diabetes; and patient unwilling or unable to cooperate. Factors considered during the clinical evaluation were medical history, number of tender and swollen joints, pain intensity assessed by the patient on a 100 mm visual analog scale (VAS), and laboratory tests (erythrocyte sedimentation rate [ESR], C-reactive protein [CRP]). The parameters made it possible to determine improvement according to the criteria based on DAS28, suggested by the EULAR.
The day of the anti-TNF drug administration constitutes the beginning of the participants’ observation for this study (day 0). Clinical parameters and disease progression were then monitored and analyzed after 12 weeks (3 months) and 24 weeks (6 months) of the anti-TNF therapy. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Wrocław Medical University (identification code KB-751/2018).
SNPs in the VDR coding gene were chosen for the study based on their minor allele frequency (MAF, 1000 Genomes Project) above 10% in the European population, as well as potential clinical or biological impact. Here, SNP characteristics, such as introducing a change in RNA and/or amino acid sequence, potential splicing site, and/or miRNA binding site, were the most crucial factors for SNP selection. All necessary information mentioned above were collected based on the NCBI SNP database as well as literature. As a result, the following four polymorphic variants were selected for the current experiment: rs2228570, rs1544410, rs7975232, and rs731236.
The first of the chosen polymorphisms, rs2228570 (also named FokI after the restriction enzyme commonly utilized for its genotyping) (Gleba et al. 2022), is a thymine (T) to cytosine (C) substitution in exon 1 of the VDR gene. The presence of the mutated allele (C) causes the first methionine (Met) codon (ATG) of the coding sequence to be changed into one encoding threonine (Thr) (ACG). Consequently, the start of translation is located three codons downstream of the sequence (with the next Met codon) in the mutated variant compared to the wild type. The rs2228570 C protein isoform (three amino acids shorter than the original one) (Arai et al. 1997) was reported as 1.7-fold more active than the longer one (Uitterlinden et al. 2004). Therefore, individuals carrying the mutated C allele could potentially be more sensitive to changes in vitamin D levels. The rs2228570 polymorphism was also reported as a marker of familial RA, although experimental data are inconsistent (Goertz et al. 2003; Ranganathan 2009).
The second VDR gene polymorphism selected for this study was rs1544410 (also known as BsmI), which is an intronic guanine (G) to adenine (A) substitution. Based on recent experimental studies, it is hypothesized that this genetic variant may affect mRNA stability and generate an alteration in the splice site or a change in intron regulatory elements (Ruiz-Ballesteros et al. 2020). This could potentially have an impact on VDR protein activity and biological function, although the exact biological effect remains unclear. Experimental studies suggest that the rs1544410 polymorphism is related to lower bone mineral density (BMD) and higher bone turnover markers (Rass et al. 2006), which makes it an interesting study subject in diseases such as RA.
The two remaining SNPs included in the experiment were rs731236 (TaqI) and rs7975232 (ApaI). Those VRD genetic variants are localized in close proximity, so the same PCR primer sets are usually utilized to study them both (Maj et al. 2019; Gleba et al. 2022). The exonic rs731236 variant consists of a thymine (T) to cytosine (C) substitution. This silent mutation causes one isoleucine (Ile) codon (ATT) to be replaced by another isoleucine codon (ATC). As such, there is no change in the amino acid chain of the VDR protein (based on the NCBI SNP database, as of 14 April 2023: https://www.ncbi.nlm.nih.gov/snp/rs731236#variant_details). There are suspicions, however, that this SNP could affect mRNA stability or modify the binding with vitamin D-responsive elements located in the target genes (Latini et al. 2021). It was also reported to accelerate bone loss in women with RA (Gough et al. 1998). Meanwhile, the VDR gene polymorphism rs7975232 is an intronic cytosine (C) to adenine (A) substitution. This one is hypothesized to affect mRNA stability and gene expression (Mahto et al. 2018). As such, translation of the protein could be affected, potentially changing the efficiency of the receptor response to vitamin D. This could have an immense effect on the course of the disease and is worth further investigation.
Whole blood samples were collected into BD Vacutainer K2EDTA tubes (Becton, Dickinson, Franklin Lakes, NJ, USA) by experienced medical personnel at the Department of Rheumatology and Internal Medicine, Wrocław Medical University, and the Department of Rheumatology and Connective Tissue, Jan Biziel University Hospital No. 2 in Bydgoszcz, Poland. The biological material was transported to the Laboratory of Clinical Immunogenetics and Pharmacogenetics, Hirszfeld Institute of Immunology and Experimental Therapy, PAS, Wroclaw, Poland, for nucleic acid extraction and genotyping studies. The patient samples were stored at −20°C. At the time of DNA isolation, samples were thawed and brought to room temperature. The QIAmp DNA Blood Mini/Midi Kit (Qiagen, Hilden, Germany) was used following the manufacturer’s recommendations. For VDR SNPs detection, quantitative PCR was performed using the LightSNiP assay (TIB MOLBIOL, Berlin, Germany) and LightCycler FastStart DNA Master HybProbe (Roche Diagnostics GmbH, Mannheim, Germany) on the LightCycler 480 II Real-Time PCR Instrument (Roche Diagnostics GmbH, Basel, Switzerland). The reaction was performed according to the manufacturer’s instructions. The presence of VDR genetic variants was assessed by amplification and labeling with specific probes, followed by melting curve analysis.
Data regarding patients’ characteristics and clinical parameters were collected and statistically analyzed. To describe associations within investigated SNPs, genetic models were introduced. The genotypes were coded as a dominant homozygote (MM), a heterozygote (Mm), and a variant homozygote (mm). A dominant model compared MM vs. Mm + mm, whereas a recessive model compared MM + Mm vs. mm. An overdominant model was described as MM + mm vs. Mm. The comparisons between MM and Mm, and mm were included in a codominant model.
Data and clinical parameters collected during experiments were analyzed statistically with the R software version 4.0.3 (http://www.rproject.org, Accessed on June 13, 2022) and GraphPad Prism 7 for Windows (GraphPad Software, La Jolla, CA, USA). The GraphPad Prism 7 was also used to prepare the figures. Data normality was verified with the Shapiro–Wilk test. The quantitative data with normal distribution was presented as mean ± standard deviation (SD). Non-normally distributed data were shown as medians with interquartile ranges (IQRs). The chi-square or Fisher’s exact test was applied to compare genotypes and allele frequencies between the patient and control groups. The unpaired two-sample Wilcoxon test was introduced to identify associations between clinical parameters (such as CRP, DAS28, and VAS values) and genetic variants. Fisher’s exact test was used to analyze relationships between categorical data (e.g., treatment response) and genotypes. To analyze relationships between vitamin D3 levels and VDR polymorphic variants, the Kruskal–Wallis test followed by an unpaired two-sample Wilcoxon test or one-way ANOVA followed by a t-test were performed for non-parametric or parametric associations, respectively. Probability (p) values of 0.05 or lower were considered statistically significant. p-values after Bonferroni correction (pc) were calculated by multiplying 0.05 by the number of SNPs. Hardy–Weinberg equilibrium (HWE) was calculated manually using Microsoft Excel 2019 (version 16.0.10369.20032, Microsoft Corporation, Redmont, WA, USA).
The clinical data of RA patients are listed in Table 1. During anti-TNF therapy, the disease activity was significantly reduced from high (DAS28 >5.1) to low (DAS28 ≤3.2). In general, patients achieved good response to treatment.
Characteristics of the RA patients included in the study
| Number of patients | 121 |
|---|---|
| Age mean in years (±SD) | 52.2 (13.3) |
| Disease duration mean in years (±SD) | 13.6 (9.31) |
| Disease onset mean in years (±SD) | 38.6 (14.0) |
| Sex F/M (%) | 96/25 (79.3) |
| BMI mean (±SD) | 25.7 (4.69) |
| RF-positive patients (%) | 86.7 |
| Anti-CCP positive patients (%) | 82.4 |
| Anti-TNF drugs: | N (%) |
| Adalimumab | 41 (33.9) |
| Etanercept | 48 (39.7) |
| Certolizumab pegol | 19 (15.7) |
| Golimumab | 9 (7.44) |
| Infliximab | 4 (3.31) |
| Concomitant treatment at the start of biologic treatment | (%) |
| NSAIDs | 73.2 |
| MTX | 83.6 |
| Corticosteroids | 82.1 |
| Disease activity: | |
| DAS28 before treatment, mean (±SD) | 6.14 (0.713) |
| DAS28 after 6 months of treatment, mean (±SD) | 2.63 (0.939) |
Anti-CCP, anti-cyclic citrullinated peptide antibody; BMI, body mass index; CRP, C-reactive protein; DAS28, disease activity score 28; F, female; M, male; MTX, methotrexate; NSAIDs, non-steroidal anti-inflammatory drugs; RA, rheumatoid arthritis; RF, rheumatoid factor; SD, standard deviation; TNF, tumor necrosis factor.
No statistically significant differences in the distribution of VDR genotypes and alleles were found between healthy controls and RA patients (Table 2). The observed allele and genotype frequencies closely resembled those reported in the NCBI SNP database. The distributions of all SNP genotypes in the patient and control groups were consistent with HWE (p > 0.05).
VDR genotype and minor allele frequencies of RA patients and control group
| Genotypes | MAF | χ2 | χ2 p-value | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SNP | RA | Controls | RA | Controls | RA | Controls | RA | Controls | 1000 genomes project–CEU | RA | Controls | RA | Controls |
| rs1544410 | AA | AG | GG | 0.368 | 0.434 | 0.470 | 0.408 | 2.146 | 0.523 | 0.143 | |||
| 18 | 27 | 53 | 52 | 50 | 43 | ||||||||
| rs2228570 | CC | CT | TT | 0.438 | 0.422 | 0.429 | 0.006 | 0.417 | 0.937 | 0.518 | |||
| 38 | 39 | 60 | 63 | 23 | 20 | ||||||||
| rs731236 | CC | CT | TT | 0.360 | 0.409 | 0.400 | 0.869 | 2.920 | 0.351 | 0.087 | |||
| 18 | 15 | 51 | 65 | 52 | 36 | ||||||||
| rs7975232 | AA | AC | CC | 0.483 | 0.496 | 0.404 | 0.068 | 1.692 | 0.794 | 0.193 | |||
| 33 | 26 | 59 | 65 | 29 | 25 | ||||||||
χ2, chi-square; MAF, minor allele frequency; RA, rheumatoid arthritis; SNP, single nucleotide polymorphism; VDR, vitamin D receptor.
The age of diagnosis was found to be significantly higher in rs7975232 CC homozygous patients compared to A allele carriers (AA + AC vs. CC; mean: 36.87 vs. 43.93; p = 0.017) and the AA genotype (AA vs. CC; mean 35.94 vs. 43.93; p = 0.018).
We observed that CRP levels at baseline were lower in patients having rs1544410 AA genotype compared to G allele carriers (AA vs. AG + GG, p = 0.009, pc = 0.037). These results were confirmed in codominant models (AA vs. AG, p = 0.007, pc = 0.027; AA vs. GG, p = 0.034, pc = ns.).
Moreover, rs1544410 A allele was associated with lower VAS values after 3 months of treatment (AA + AG vs. GG, p = 0.009, pc = 0.034; AA + GG vs. AG, p = 0.038, pc = ns; AG vs. GG, p = 0.012, pc = 0.046) (Figure 1).
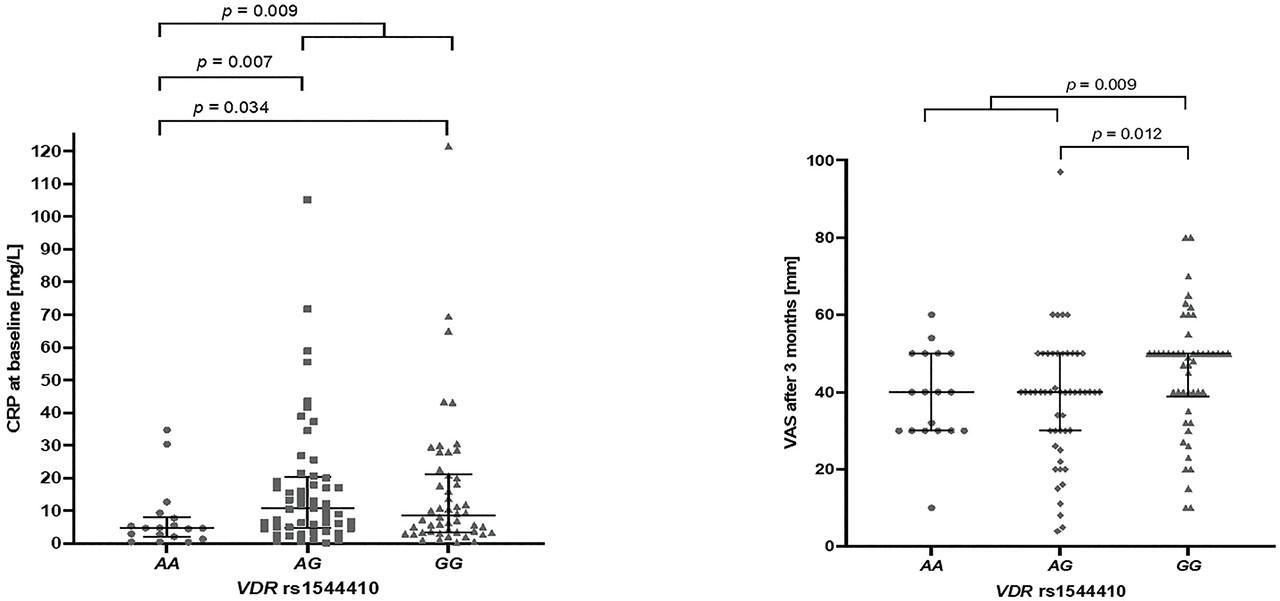
Differences in CRP and VAS parameters in relation to VDR rs1544410 genotypes (Mann–Whitney test). Data are presented as median with IQR. CRP, C-reactive protein; IQRs, interquartile ranges; VAS, visual analog scale; VDR, vitamin D receptor.
Similar findings were noted concerning rs731236 genetic variants. In this case, CC homozygosity was linked to lower CRP levels at baseline in a dominant model (CC vs. CT + TT, p = 0.009, pc = 0.037) as well as in codominant models (CC vs. CT, p = 0.006, pc = 0.026; CC vs. TT, p = 0.034, pc = ns). Statistically significant associations between higher VAS values after 3 months and the TT genetic variant were also observed in the codominant (CT vs. TT, p = 0.006, pc = 0.024) and recessive (CC + CT vs. TT, p = 0.005, pc = 0.018) models, as shown in Figure 2.
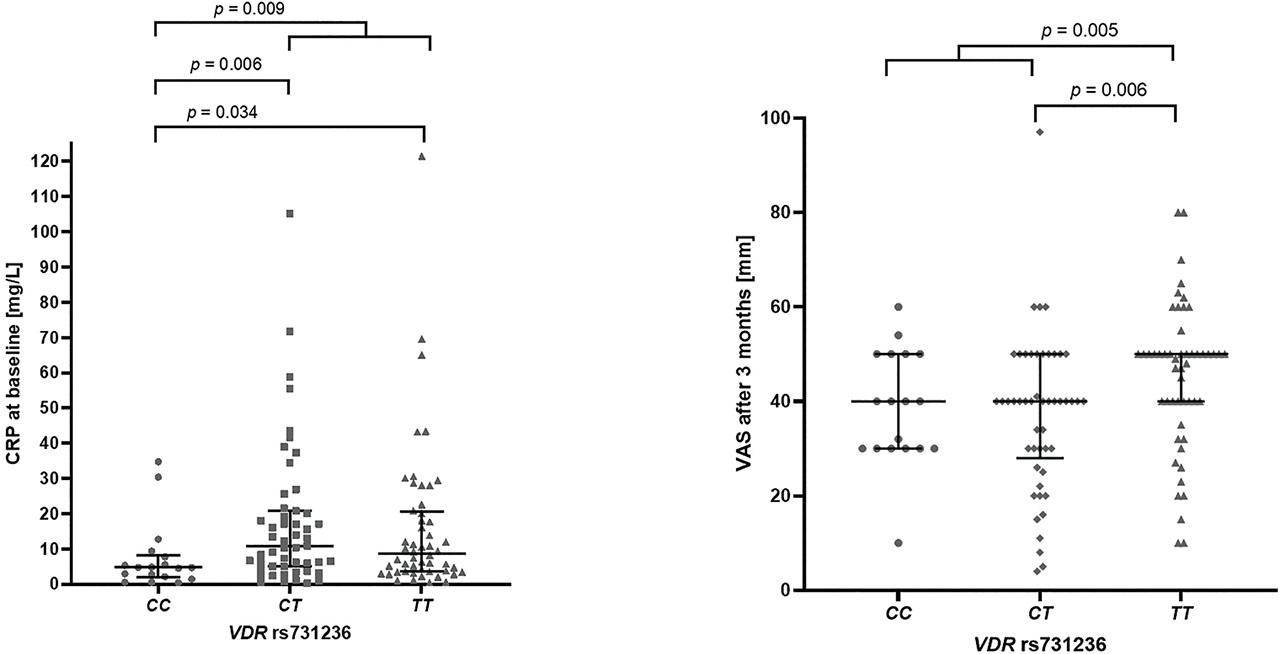
Differences in CRP and VAS parameters in relation to VDR rs731236 genotypes (Mann–Whitney test). Data are presented as median with IQR. CRP, C-reactive protein; IQRs, interquartile ranges; VAS, visual analog scale; VDR, vitamin D receptor.
Furthermore, in certain patients, the VDR rs2228570 polymorphism was related to VAS values after 3 months of therapy. Patients with the CC variant were described with lower values than those with the CT genotype (CC vs. CT, p = 0.031, pc = ns.) and the T allele (CC vs. CT + TT, p = 0.049, pc = ns.). No statistically significant relationships have been found between the parameters CRP and VAS and rs7975232. However, the rs7975232 CC homozygotes seemed to be related to higher DAS28 values after 6 months of treatment when compared to the AC genotype (AC vs. CC, p = 0.025) or those with the A variant (AA + AC vs. CC, p = 0.030). Both results were insignificant after the Bonferroni correction. Interestingly, the A allele was statistically more often observed among individuals who achieved remission (DAS28 = < 2.6) after 6 months of therapy, as shown by the dominant (AA + AC vs. CC, p = 0.004; Fisher’s exact test) and the codominant (AC vs. CC, p = 0.008; AA vs. CC, p = 0.016; Fisher’s exact test) models.
The subgroup of patients enrolled in this study had performed additional laboratory tests, including measurement of calcium, alkaline phosphatase, 25-hydroxyvitamin D3 (25(OH)D3), and thyroid-stimulating hormone (TSH) concentrations (Table 3).
Characteristics of patients’ subgroup
| Calcium (mg/dL) | Alkaline phosphatase (U/L) | Vitamin D3 (ng/mL) | TSH (ulU/mL) | |
|---|---|---|---|---|
| N | 56 | 64 | 54 | 64 |
| Minimum | 8.9 | 36 | 4.64 | 0.271 |
| Median | 9.7 | 74.5 | 23.67 | 1.201 |
| Maximum | 10.7 | 350 | 66 | 4.331 |
| IQR | 0.5 | 33.25 | 23.14 | 0.744 |
IQR, interquartile range; N, number of individuals; TSH, thyroid-stimulating hormone.
The 25(OH)D3 deficiency (<30 ng/mL) was recognized in 66.7% of RA patients (n = 36) despite the use of vitamin D supplements, occurring in 64.1% of patients.
The baseline vitamin D levels were varied between distinct rs2228570 and rs7975232 genotypes (Figure 3). Higher values were observed in rs2228570 CT heterozygotes compared to homozygotes in overdominant (CC + TT vs. CT, p = 0.004) and codominant models (CC vs. CT, p = 0.009) (Table 4). In turn, rs7975232 heterozygotes had lower levels than homozygous patients (AA + CC vs. AC, p = 0.003; AA vs. AC, p = 0.021; AC vs. CC, p = 0.009) (Table 5). Thus, vitamin D deficiency (<30 ng/mL) was more likely observed in rs2228570 homozygous patients (CC + TT vs. CT, p = 0.041; Fisher’s exact test) as well as rs7975232 heterozygotes (AA + CC vs. AC, p = 0.003; AA vs. AC, p = 0.031; AC vs. CC, p = 0.004; Fisher’s exact test).
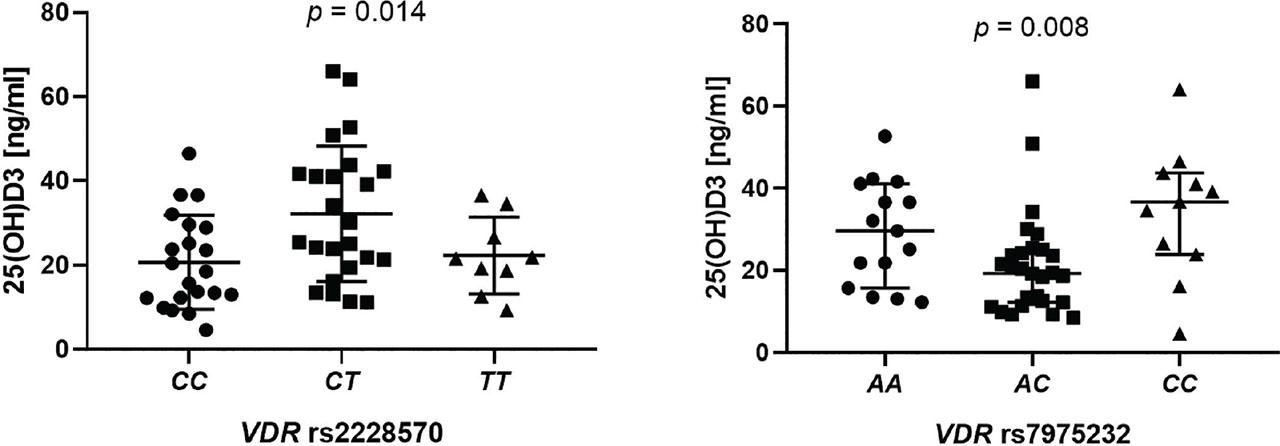
Differences in the levels of 25(OH)D3 level (ng/mL) according to the presence of VDR genotypes: rs2228570 (ordinary one-way ANOVA, p = 0.014) and rs797532 (Kruskal–Wallis test, p = 0.008). 25(OH)D3, 25-hydroxyvitamin D3; VDR, vitamin D receptor.
Relationships between VDR rs2228570 genetic variants and vitamin D levels in RA patients
| VDR rs2228570 | 25(OH)D3 conc. (ng/mL) | |
|---|---|---|
| Mean (±SD) | CC | 20.69 ± 11.12 |
| CT | 32.22 ± 16.06 | |
| TT | 22.33 ± 9.077 | |
| Median (IQR) | CC | 18.47 (16.98) |
| CT + TT | 25.08 (22.07) | |
| CC + CT | 23.88 (24.48) | |
| TT | 21.54 (14.92) | |
| p-values | CC vs. CT + TT | 0.028† |
| CC + CT vs. TT | 0.508† | |
| CC + TT vs. CT | 0.004‡ | |
| CC vs. CT | 0.009‡ | |
| CT vs. TT | 0.093‡ | |
| CC vs. TT | 0.701‡ |
Mann–Whitney test.
t-test.
25(OH)D3, 25-hydroxyvitamin D3; IQR, interquartile range; RA, rheumatoid arthritis; SD, standard deviation; VDR, vitamin D receptor.
statistically significant.
Relationships between VDR rs7975232 genetic variants and vitamin D levels in RA patients
| VDR rs7975232 | 25(OH)D3 conc. (ng/mL) | |
|---|---|---|
| Median (IQR) | AA | 29.6 (25.34) |
| AC + CC | 21.54 (21.2) | |
| AA + AC | 21.54 (17.02) | |
| CC | 36.68 (19.87) | |
| AA + CC | 33.33 (20.81) | |
| AC | 19.32 (12.56) | |
| Mann–Whitney test p-values | AA vs. AC + CC | 0.1703 |
| AA + AC vs. CC | 0.029 | |
| AA + CC vs. AC | 0.003 | |
| AA vs. AC | 0.021 | |
| AC vs. CC | 0.009 | |
| AA vs. CC | 0.324 |
25(OH)D3, 25-hydroxyvitamin D3; IQR, interquartile range; RA, rheumatoid arthritis; VDR, vitamin D receptor.
statistically significant.
None of the VDR polymorphic variants analyzed in this study were related to response to anti-TNF therapy after 3 months or 6 months of administration evaluated according to EULAR criteria (individual data not shown).
TNF-α is one of the key factors in RA, affecting its course, severity, and progression, and treatment with inhibitors for this cytokine is among the most effective therapies for the disease. Vitamin D downregulates TNF-α-mediated pro-inflammatory effects, especially in macrophages and T cells of RA patients (Ruefli-Brasse et al. 2003). Furthermore, low vitamin D levels increase the tender joint count and DAS28 (Patel et al. 2007). An in vitro study on a human cell line demonstrated that different TNF-α concentrations combined with vitamin D supplementation significantly increase the apoptosis of RA fibroblast-like synoviocytes (Gu et al. 2016). Also, elevated concentrations of TNF-α intensified the pro-apoptotic effect of vitamin D, and the VDR mediated this mechanism. Vitamin D is of great interest in the current RA research, and thus, we decided to study the role of polymorphisms in the VDR gene and their effects on the disease course and outcomes during treatment with TNF-α inhibitors.
Vitamin D intake was found to lower the risk of developing RA in a prospective 11-year study of over 29,000 women in a cohort, aged 55–69 years, without a history of RA (Merlino et al. 2004). A higher intake of vitamin D was associated with a lower risk for RA. Findings from other research groups (Cutolo et al. 2011; Gatenby et al. 2013) that low serum vitamin D levels are associated with an earlier RA onset and more active disease support this notion. Other studies describe further important results: the prevalence of vitamin D deficiency was found to be 30%–63% in patients with RA, serum vitamin D levels negatively correlated with RA activity, and vitamin D supplementation was beneficial for RA treatment (Song et al. 2012; Feng et al. 2013). Moreover, it was found that vitamin D levels are significantly different in RA patients from distinct European countries, with higher concentrations in Spain compared to Poland (Vojinovic et al. 2017). Our study also reported a 25(OH)D3 deficiency (<30 ng/mL) in 66.7% of patients despite the intake of vitamin D supplementation. Still, the beneficial effects of vitamin D supplementation in experimental models are not necessarily replicable in clinical practice. The use of vitamin D in the therapy of autoimmune diseases is still being investigated. Importantly, vitamin D signaling inhibits the NF-κB, MAPK, and JAK/STAT pathways, which are targets for drug development in RA (Tarner et al. 2007). For example, treatment with increasing dosages of vitamin D (in the form of 1,25[OH]2D) intensifies the effects of etanercept, an anti-TNF drug used in clinical practice (Dankers et al. 2016). Also, a combined treatment with 1,25[OH]2D, dexamethasone, and etanercept was shown to have an additive effect compared to therapy with etanercept alone. Treatment with vitamin D and calcipotriol (vitamin D hypocalcemic analog) tended to reduce the levels of most pro-inflammatory mediators in stimulated synovial stromal cells of patients with RA or osteoarthritis (Huovinen et al. 2023). The combination of calcipotriol and dexamethasone further reduced secretion of IL-6, IFN-γ, basic fibroblast growth factor (FGF), and vascular endothelial growth factor (VEGF) when compared to therapy with calcipotriol or dexamethasone alone.
VDR plays the role of a transcription factor and is located in various organs and tissues (Uhlén et al. 2015). Importantly, VDR was found in the rheumatoid synovium and areas of cartilage erosion in human RA (Jeffery et al. 2016; Aslam et al. 2019). Also, it is localized not only in the lining and the subliming layers but also in the vascular endothelium of synovial tissue in RA (Huovinen et al. 2023). In a study based on a mouse model, a combination of VDR disruption and a TNF-α transgene caused spontaneous development of arthritis (Zwerina et al. 2011). This experimental result showed the importance of the VDR in the suppression of inflammation—at least in mice. There are also reports showing that vitamin D supplementation may be associated with a lower risk of disease development and lower disease activity (Merlino et al. 2004; Patel et al. 2007). It is not surprising that vitamin D supplementation and VDR genotypes exhibit such effects considering that the central pathological feature in RA is joint and bone destruction.
In this study, we investigated the relationships between four VDR polymorphisms— rs1544410 (BsmI), rs2228570 (FokI), rs731236 (TaqI), and rs7975232 (ApaI)—and disease susceptibility and progression in RA patients treated with anti-TNF medication. The function of these VDR genetic variants is not yet fully understood, and their effects on VDR function or gene transcription are unclear. There is evidence associating those variants with autoimmune diseases such as multiple sclerosis (Fukazawa et al. 1999) and type I diabetes mellitus (McDermott et al. 1997; Pani et al. 2000). Furthermore, VDR polymorphisms seem to also impact bone turnover (Morrison et al. 1992) and bone density (Morrison et al. 1994; Sainz et al. 1997). We found no difference in the frequency of any VDR polymorphic variants studied between RA patients and controls. Similarly, no such relations were shown by other study groups (Gough et al. 1998; Lee et al. 2001). However, in the Egyptian population, the ApaI, BsmI, and TaqI polymorphisms may contribute to RA susceptibility (Saad et al. 2015). Two case–control studies found no significant evidence regarding FokI genetic susceptibility (Mosaad et al. 2014; Saad et al. 2015). Another study showed that the FokI variant increased RA risk (Despotović et al. 2021). Also, the contribution of TaqI and FokI polymorphisms in RA development was observed in the study by Tizaoui and Hamzaoui (2015). None of the studied polymorphisms were found to be related to RA susceptibility. However, RA patients carrying the rs7975232 A allele were characterized by significantly lower age of diagnosis when compared to individuals with the CC genotype. Also, other researchers reported that the VDR rs7975232 genotypes were found to be associated with RA onset (Mukhtar et al. 2019).
It has been known that vitamin D has immunomodulatory properties; thus, possible associations between VDR gene polymorphisms and the course of RA have been investigated. Lee et al. (2001) found that bone loss in females (but not in males) is influenced by the presence of the rs731236 TT genotype compared to the CC genotype. Here, the bone loss in women was 4.9%–9.6% (depending on the bone loss site) for the TT homozygotes, while only 0.1%–3.9% for the CC genotype carriers (Lee et al. 2001). It is an interesting observation, taking into account that RA occurs more often in females. Rass et al. (2006) reported lower BMD in RA patients carrying the rs1544410 A allele compared to GG homozygotes. Their results suggest that the A variant could be a marker for increased osteoclastic activity and consequently greater bone resorption and bone loss (Rass et al. 2006). In addition, some of the clinical parameters studied seemed related to VRD genetic variants. Experiments by other study groups showed that although patients with arthritis may have normal serum vitamin D levels, VDR gene polymorphism may restrict vitamin D from performing its anti-inflammatory role by altering the 1,25[OH]2D binding sites (Mukhtar et al. 2019). Polymorphic variants of the VDR may enhance the anti-inflammatory properties of the anti-TNF drugs. This was reflected in the treatment efficacy described in our study. The literature data showed that BsmI GG and AG genotypes, as well as FokI CC and CT variants, were associated with high RA activity (Idriss et al. 2020). Interestingly, we observed that CRP levels at baseline were higher in patients carrying the rs1544410 (BsmI) G allele compared to the AA genotype. The VDR rs2228570 (FokI) CT variant was related to higher VAS values after 3 months of therapy than the CC genotype. We also found the VDR rs7975232 (ApaI) polymorphism to be related with disease progression. RA patients treated with TNF-α inhibitors had significantly lower DAS28 values after 24 weeks of treatment when carrying the rs7975232 A allele compared to the CC homozygotes.
Regarding vitamin D levels, a recent study suggests that VDR ApaI gene polymorphisms influence protein concentration, showing significantly higher serum levels in RA patients with the CC (aa) genotype (Ahmad et al. 2024). Another author reported that the C allele (F) within the FokI polymorphism increased vitamin D levels (AbdElneam et al. 2023). Our results indicate the role of rs2228570 (FokI) and rs7975232 (ApaI) genetic variants in modulating vitamin D levels. The results revealed that patients with the rs2228570 CC genotype had lower vitamin D3 levels than those with the T allele. Also, vitamin D3 levels were significantly lower in rs7975232 A allele carriers compared to CC homozygotes. An association between vitamin D levels and rs2228570 variants was seen in another autoimmune disease, type 1 diabetes mellitus. In this case, the TT genotype carriers presented statistically greater levels of 25(OH)D3 (Ferraz et al. 2022; Mostafa et al. 2024).
It is known that FokI is a functioning site of the VDR gene and determines the length of proteins. The shorter VDR form, encoded by the C allele, is more active and effectively binds 1,25(OH)2D3 when compared to the T allele (Whitfield et al. 2001). The same VDR polymorphism was also found to affect TNF-α levels in another type of arthritis, knee osteoarthritis (Hassan et al. 2022). A significantly higher mean level of TNF-α was found in the synovial fluid of patients with VDR rs7975232 CC or AC genotypes compared to AA homozygotes. A similar observation was also made for the VDR rs731236 polymorphism, where the CC genotype exhibited significantly higher mean levels of TNF-α in synovial fluid than CT heterozygotes. Furthermore, a significant increase in circulating and synovial fluid levels of TNF-α was observed concerning disease severity (Hassan et al. 2022). It is important to note that knee osteoarthritis is caused by mechanical injury of the tissue, so increased levels of TNF-α are an effect rather than the cause. Our study did not provide evidence that one of the investigated VDR polymorphisms affected anti-TNF treatment outcomes in RA patients. In line with this observation, other researchers reported that the rs2228570 SNP was not associated with response in juvenile idiopathic arthritis patients undergoing treatment with etanercept (Bašić et al. 2019), which is a predominant TNF inhibitor in our group. However, our previous results showed that the VDR rs2228570 A variant, as compared to CC genotype, was more common in patients who achieved remission and in those with Bath Ankylosing Spondylitis Disease Activity Index improvement ≥75% after 6 months of anti-TNF therapy (Bugaj et al. 2022). This variant was also more frequently observed in RA individuals who achieved remission in this study. Despite the strength in the group homogeneity of the Polish RA patients and the demonstration of significant associations, this study has some limitations. Our results should be implicated in a larger population. We also suggest that further investigations into the effects of VDR polymorphisms could be useful to widen our understanding of RA development.
In summary, our data suggest that VDR polymorphisms, especially rs2228570 and rs7975232, together with vitamin D level should be considered when examining the factors associated with RA. Genotyping of rs7975232 might be useful in the evaluation of disease onset and disease activity in RA patients treated with TNF inhibitors. Consequently, it may have an impact on clinical decisions.