
In recent years, the role of endothelial dysfunction in the development of multiple pathologies such as hypertension, kidney failure, and cancer has been suggested (Rajendran et al. 2013). Fundamentally, the link between endothelium and disease pathogenesis is the most evident in the field of hematology and transplantation. Indeed, much research was conducted with regard to graft-versus-host disease (GvHD), both in preclinical and clinical research, confirming endothelium-related mechanisms involved in GvHD (Biedermann et al. 2002; Penack et al. 2010; Almici et al. 2014; Luft et al. 2017; Riesner et al. 2017). With promising results, researchers’ attention turned to other hematological pathologies such as lymphomas (Menzel et al. 2020; Park et al. 2022).
Overall, the interplay between the endothelium and disease could be attributed to the fact that endothelial cells (ECs) are the mediators of inflammation as they represent the first contact site for immune effector cells (Cordes et al. 2021). Additionally, ECs are also involved in angiogenesis and, therefore, contribute to tumor growth (Folkman 1995; Eelen et al. 2018). Endothelium status associated with these properties is termed “endothelial activation” and is triggered by various factors, including mechanical, immunological, and chemical injuries (Trepels et al. 2006). When damaged, ECs undergo phenotypic changes that result in increased expression of adhesion molecules and cytokines (Trepels et al. 2006). In turn, it leads to increased vascular permeability, promotes leukocyte migration, as well as creates a state of proinflammatory and procoagulant environment (Trepels et al. 2006). Notably, procedures involved in standard-of-care treatment for hematological diseases may induce a state of endothelial activation themselves. For instance, it can be triggered by chemo- or radiotherapy regimens or cytokines released by damaged tissues (Molema 2010; Palomo et al. 2010). Moreover, exposure to bacterial endotoxins may also contribute to endothelial activation (Palomo et al. 2010).
As the endothelial activation hypothesis gained researchers’ interest, it became inevitable to seek EC-related markers that could be utilized in clinics as predictors of patients’ survival or severity of adverse events. Numerous molecules such as angiopoietins, components of the coagulation pathway, or soluble cell-surface adhesion molecules are potential candidates (Page and Liles 2013). However, they are not routinely assessed in clinics. To address this need, Luft et al. (2017) introduced the Endothelial Activation and Stress Index (EASIX) score, which serves as a surrogate measurement of endothelial dysfunction. EASIX combines three routinely assessed parameters, namely, lactate dehydrogenase (LDH), creatinine, and platelet (PLT) count, which are readily accessible in every center (Luft et al. 2017; Mariotti et al. 2023). Each component of the EASIX score represents a distinctive characteristic of endothelial damage that can be measured in laboratory tests. LDH serum levels are associated directly with ECs that release this enzyme upon damage (Luft et al. 2017). PLT count represents a link between endothelial injury and clotting, whereas creatinine links endothelial dysfunction and its contribution to renal failure (Luft et al. 2017). Since its conception, EASIX has been studied and associated with survival outcomes and adverse events occurrence in malignancies such as large B-cell lymphoma (LBCL), myelodys-plastic neoplasms, multiple myeloma (MM), and allogeneic stem cell transplantation (Merz et al. 2019; Luft et al. 2020; Song et al. 2020; Thanhakun et al. 2023). Nevertheless, the EASIX score is not specific due to various confounding factors (Luft et al. 2017) and therefore validation of its utility is necessary for each proposed pathology.
Most recently, chimeric antigen receptor (CAR)-T cell therapy has revolutionized treatment outcomes in patients with relapsed or refractory hematological malignancies (Zhang et al. 2022). The treatment effects come at the cost of potentially life-threatening toxicities such as cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (Zhang et al. 2022). Pathogenesis of these adverse events is clearly attributable to endothelial activation (Hay et al. 2017; Gust et al. 2020). Therefore, it seems reasonable to implement the EASIX score as a prognostic factor of adverse events in CAR-T therapy. Indeed, the EASIX score has been tested as a prognostic factor for CRS occurrence in non-Hodgkin lymphoma patients treated with CAR-T cells and has been proposed as a valuable tool for prevention strategies (Greenbaum et al. 2020; Korell et al. 2022).
Despite all the promising results, there is still little evidence of EASIX’s utility in the routine management of CAR-T patients. Moreover, as of March 2024, there is only one report on the prognostic value of EASIX for CAR-T therapy against MM. Therefore, we decided to assess the prognostic value of the EASIX score for the occurrence of severe CRS (grade 3 or higher) in patients receiving CAR-T cells in LBCL and MM (combined with light chain amyloidosis patients). Furthermore, we also characterize EASIX values based on factors such as lymphodepleting regimen, gender, or age in each cohort, and check for associations of these factors with CRS severity.
This retrospective cohort study comprised two cohorts of patients and relied exclusively on the data extracted from electronic medical records. The sample sizes were entirely dependent on the number of patients qualified for the CAR-T therapy. The study was conducted according to the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines (von Elm et al. 2008).
The first cohort (N = 69) consisted of patients treated with novel academic anti-B-cell maturation antigen (anti-BCMA) CAR-T therapy (NXC-201) against MM (N = 64) or light chain amyloidosis (N = 5) at the Department of Bone Marrow Transplantation and Cancer Immunotherapy, Hadassah Ein Karem Hospital, Jerusalem. CAR-T cells were administered in the following doses: 150 × 106 CAR-T cells (dose 1, N = 6), 450 × 106 CAR-T cells (dose 2, N = 7), and 800 × 106 CAR-T cells (dose 3, N = 56) (Asherie et al. 2023). All patients had been recruited and had fulfilled inclusion criteria for Phase 1 clinical trial NCT04720313. We have analyzed medical records collected from February 2021 to March 2023.
The second cohort (N = 65) included patients treated with anti-cluster of differentiation (CD)19 CAR-T therapy against LBCL, specifically tisagenlecleucel/tisa-cel (N = 55) and axicabtagen ciloleucel/axi-cel (N = 10) administered as standard-of-care treatment. Fifty-seven patients received the therapy at the Department of Bone Marrow Transplantation and Cancer Immunotherapy, Hadassah Ein Karem Hospital, Jerusalem (records from December 2019 to June 2023). Eight patients received the therapy (tisa-cel only) at the Department of Hematology, Transplantation and Internal Medicine, Medical University of Warsaw, Warsaw (records from December 2022 to October 2023).
The study was conducted in accordance with the Declaration of Helsinki. Institutional Review Board’s consent for the research was granted in each center (No. KB/132/2022 and No. HMO 0090-20).
Occurrence of CRS grade 3 or higher was considered as the primary endpoint. The secondary endpoint was the occurrence of CRS grade 2 or higher. The severity of CRS was determined according to the American Society for Transplantation and Cellular Therapy consensus criteria (Lee et al. 2019).
The EASIX score was defined as proposed by Luft et al. (2017): LDH (U/L) × creatinine (mg/dL)/PLTs × (109/L). For both cohorts, the EASIX score was calculated at four different time points before CAR-T infusion to assess its prognostic value. The choice of assessing different timepoints stemmed from the potential changes in EASIX parameters due to lymphodepletion’s impact on patients’ bodies. The timepoints were as follows:
pre-lymphodepletion (EASIX-pre) – defined as a time-point before administering lymphodepleting regimen (usually between days –8 and –6 before CAR-T infusion),
during-lymphodepletion (EASIX-ld) – defined as a time-point during lymphodepleting treatment (usually between days –5 and –3 before CAR-T infusion),
after-lymphodepletion (EASIX-gap) – defined as a time-point after lymphodepletion, but before CAR-T infusion (usually on days –2 or –1 before CAR-T infusion),
day 0 (EASIX-0) – defined as a timepoint immediately before CAR-T infusion.
Moreover, we decided to calculate simplified EASIX (s-EASIX) as proposed by Pennisi et al. (2021): LDH (U/L)/PLTs (×109/L) (the formula excludes creatinine and was hypothesized to provide better prediction of developing CRS). Calculations were performed for the identical time-points as for ordinary EASIX score and termed s-EASIX-pre, s-EASIX-ld, s-EASIX-gap, s-EASIX-0.
In addition to laboratory data necessary to calculate EASIX scores, we have collected the following data: age, gender, lymphodepletion regimen, and dose of CAR-T cells (in anti-BCMA cohort).
Descriptive statistics for each cohort were summarized using standard statistical measures: number, frequency, mean, median, and range (minimum/maximum). The normality of data distribution was assessed using the Shapiro–Wilk test. If data were normally distributed, t-test for independent samples or analysis of variance (ANOVA) were used when applicable. If data were not normally distributed, the nonparametric U-Mann–Whitney test or Kruskal–Wallis test were used when applicable. Tests for associations were performed using Fisher’s exact test, whereas the strength of associations was assessed with Cramer’s V test. Univariable binary logistic regression with Firth correction was employed to assess the relationship between continuous variables and categorical dependent variables (CRS grade). This yielded odds ratios (ORs) with 95% confidence intervals (CIs). If the regression analysis yielded significant results, maximally selected rank statistic was implemented to determine cutoffs to categorize continuous predictor variables into two levels. After categorization, the predictor variable was included in a binary logistic regression model (with Firth correction) developed to predict severe CRS (grade 3 or higher). Bootstrap method (1000-iteration resampling) was used for internal validation of the model.
Importantly, log-transformed EASIX data was not used in the above-mentioned analyses as normality was not achieved following transformation (no benefit for statistical analysis). Furthermore, the readers may find untransformed EASIX values more suitable for clinical reference.
Statistical calculations were performed using IBM SPSS Statistics 28.0.0.0 (IBM Corp., Armonk, NY, USA, 2023) and R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria, 2023). SPSS was used as primary software, whereas R was employed for maximally selected rank statistic and logistic regression with Firth correction. In all analyses, a p-value <0.05 was considered significant with no corrections for multiple testing.
General characteristics of anti-BCMA (myeloma/light chain amyloidosis) and anti-CD19 (LBCL) CAR-T cohorts are provided in Table 1. There were no differences between the groups regarding distributions of age, gender, and lymphodepleting regimen. A larger proportion of patients in the anti-BCMA cohort developed more severe CRS compared to the anti-CD19 group (p < 0.001). Moreover, both EASIX and s-EASIX scores were higher in the anti-BCMA group before and during lymphodepletion. As both cohorts represented two distinct diseases and differed significantly in variables of the main interest, we further proceeded with analysis in each cohort separately.
Summary comparison of the cohorts
| Anti-BCMA N = 69 | Anti-CD19 N = 65 | p-value | |
|---|---|---|---|
| Age in years, median (range) | 68 (40–84) | 51.5 (29–89) | 0.915 |
| Gender, male/female, N | 36/33 | 30/35 | 0.495 |
| Lymphodepletion regimen, N (%) | 1 | ||
| Flu/CTX | 63 (91) | 59 (91) | |
| Bendamustine | 6 (9) | 6 (9) | |
| CRS grade, N (%) | <0.001 | ||
| 0 | 8 (12) | 27 (43) | |
| I | 18 (26) | 12 (18) | |
| II | 34 (49) | 12 (18) | |
| III | 9 (13) | 12 (18) | |
| IV | 0 (0) | 2 (3) | |
| EASIX score, median (range), N | |||
| EASIX-pre | 1.69 (0.2–65.5); 69 | 1.24 (0.13–887.16); 61 | 0.034 |
| EASIX-ld | 1.49 (0.2–63.5); 69 | 1.1 (0.12–625.42); 58 | 0.044 |
| EASIX-gap | 1.48 (0.19–103.66); 68 | 1.17 (0.15–171.4); 58 | 0.093 |
| EASIX-0 | 1.38 (0.28–123.43); 64 | 1.04 (0.23–94.92); 63 | 0.059 |
| s-EASIX score, mean (range), N | |||
| s-EASIX-pre | 2.05 (0.25–53.61); 69 | 1.28 (0.27–499.52); 61 | 0.032 |
| s-EASIX-ld | 1.87 (0.2–54.5); 69 | 1.3 (0.3–392.11); 58 | 0.029 |
| s-EASIX-gap | 1.89 (0.2–64.48); 68 | 1.34 (0.35–107.46); 58 | 0.086 |
| s-EASIX-0 | 1.82 (0.26–51.3); 64 | 1.15 (0.45–95.71); 63 | 0.054 |
BCMA, B-cell maturation antigen; CD, Cluster of differentiation; CRS, cytokine release syndrome; EASIX, Endothelial Activation and Stress Index; Flu/CTX, fludarabine/cyclophosphamide; N, number; s-EASIX, simplified EASIX.
Total number of patients was 69, including 64 MM patients and 5 amyloid light-chain (AL) amyloidosis patients. CAR-T cells were administered in the following doses: 150 × 106 CAR-T cells (dose 1), 450 × 106 CAR-T cells (dose 2), and 800 × 106 CAR-T cells (dose 3). CRS of any grade occurred in 61 patients (88%), CRS of grade 3 or higher occurred in 9 patients (13%).
In the first step, we assessed the presence of any significant correlations or interdependencies among the independent variables. The following variables were examined: disease type, age, gender, lymphodepleting regimen, CAR-T cell dose, EASIX, and s-EASIX scores. We found a significant relationship between lymphodepleting regimen and EASIX scores at any timepoint (EASIX-pre: p = 0.025, EASIX-ld: p = 0.033, EASIX-gap: p = 0.008, EASIX-0: p = 0.007). Patients treated with bendamustine showed significantly higher EASIX scores than patients treated with fludarabine/cyclophosphamide (Flu/CTX) as depicted in Figure 1a. At the same time, s-EASIX scores differed only at one timepoint (day 0, p = 0.049). We also observed higher value of EASIX-gap and EASIX-0 in men (p = 0.038 and p = 0.016, respectively). There was no significant relationship between other independent variables.
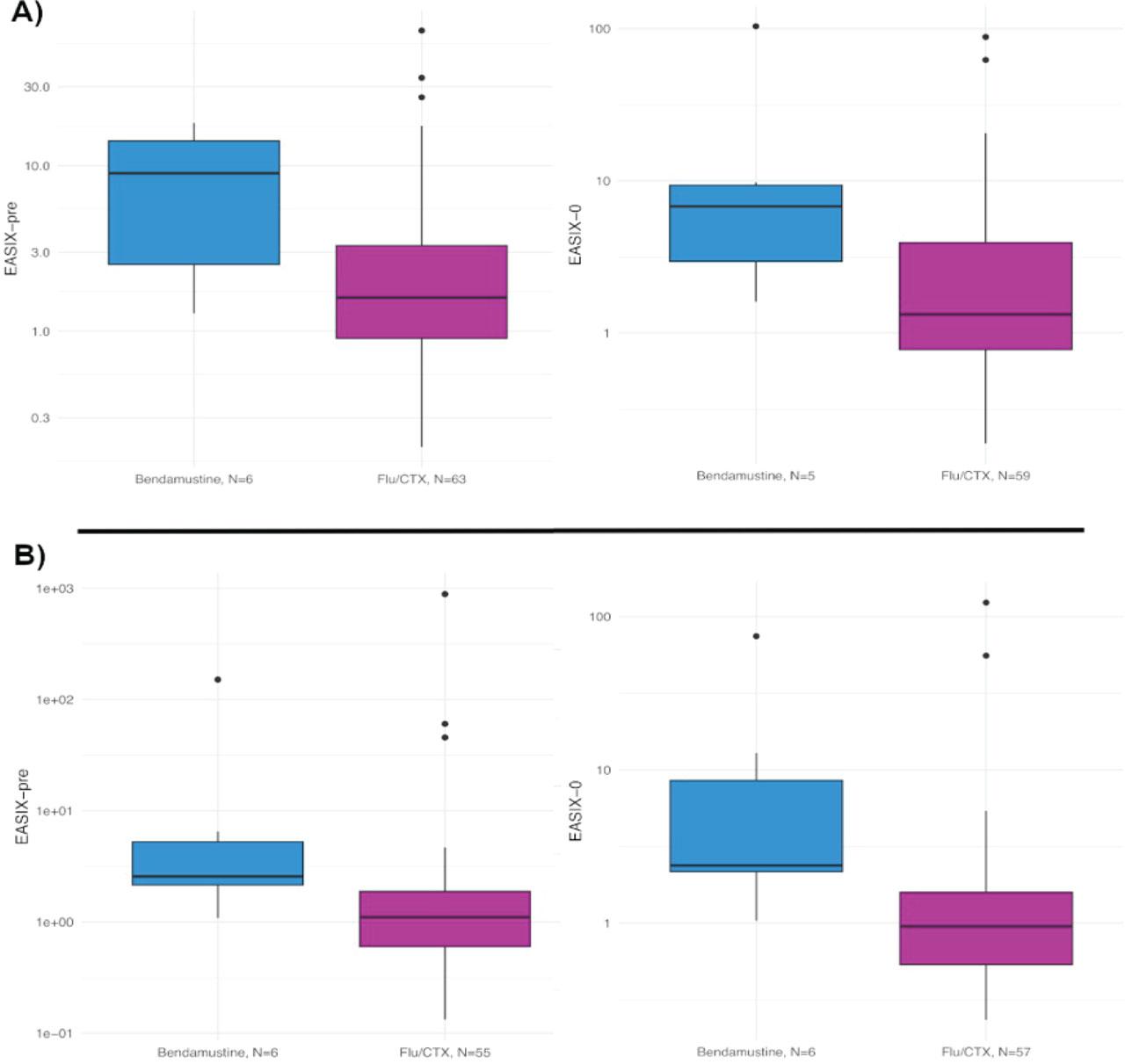
EASIX scores and lymphodepleting therapy. Patients treated with bendamustine show significantly higher EASIX values compared to Flu/CTX-treated individuals – pre-lymphodepletion and day 0 results. (A) MM/AL amyloidosis cohort and (B) LBCL cohort. AL, amyloid light-chain; EASIX, Endothelial Activation and Stress Index; Flu/CTX, fludarabine/cyclophosphamide; LBCL, large B-cell lymphoma; MM, multiple myeloma.
In the next step, we performed univariable analyses to check the relationship between CRS grade and independent variables. As the EASIX scores were significantly dependent on lymphodepleting regimen, we excluded bendamustine-treated patients (N = 6) to eliminate confounding in the analysis of EASIX’s predictive power. However, univariable binary logistic regression yielded no significant results either for EASIX or for s-EASIX at any timepoint (both for CRS ≥3 vs. grade 0–2 or CRS ≥2 vs. grade 0–1). Moreover, each component of the EASIX and s-EASIX scores showed no relationship with CRS severity (also after dose adjustment). Nevertheless, we found a significant non-random association between CAR-T dose and CRS-grade when CRS was categorized as ordinal variable (p = 0.002). Furthermore, the Cramer’s V test for association’s strength showed a significantly strong relationship between these variables (Cramer’s V = 0.419, p = 0.001). When applying dichotomous categorization of CRS the associations disappeared. Similarly, we also observed a significant non-random association between the lymphodepleting regimen and CRS grade (p = 0.013, higher CRS risk in Flu/CTX group). However, the strength of the relationship between variables (Cramer’s V = 0.328) turned out to be non-significant (p = 0.054). Finally, disease type, age, and gender were not associated with higher CRS grade. As no continuous variables showed significant association with severe CRS, no cutoff estimation was performed.
All patients in this group have been diagnosed with LBCL and treated with anti-CD19 CAR-T products. Total number of patients was 65, including 55 patients receiving tisa-cel and 10 patients receiving axi-cel. CRS of any grade occurred in 38 patients (58%), and CRS of grade 3 or higher occurred in 14 patients (22%).
Firstly, we assessed the presence of any significant correlations or interdependencies among the independent variables. The following variables were examined: CAR-T product, age, gender, lymphodepleting regimen, EASIX and s-EASIX scores. We found that patients treated with tisa-cel were older than patients who received axicel (p = 0.01). Except for the age variable, we did not find any significant differences between tisa-cel and axi-cel subgroups regarding the distribution of gender, lymphodepleting regimen. Again, we observed a significant relationship between lymphodepleting regimen and EASIX scores (Figure 1b). EASIX scores were higher in the bendamustine subgroup and differed significantly from scores in the Flu/CTX group at each timepoint (EASIX-pre: p = 0.012, EASIX-ld: p = 0.019, EASIX-gap: p = 0.002, EASIX-0: p = 0.005). S-EASIX scores differed at two timepoints (s-EASIX-gap: p = 0.021, s-EASIX-0: p = 0.028). We also observed significantly higher EASIX values in men (EASIX-pre: p = 0.006, EASIX-ld: p = 0.046, EASIX-gap: p = 0.007, EASIX-0: 0.037). There was no significant relationship between other independent variables.
In the next phase of the LBCL cohort analysis, we examined the relationship between independent variables and CRS severity. None of the categorical variables had a significant association with CRS severity (either for CRS ≥3 vs. grade 0–2 or CRS ≥2 vs. grade 0–1). Only EASIX and s-EASIX scores measured before lymphodepletion showed significant relationship with severe CRS grade ≥3 (OR = 1.06, 95% CI: 1.01–1.41, p = 0.027 and OR = 1.05, 95% CI: 1.01–1.29, p = 0.026, respectively).
On the contrary, no significant relationship with CRS grade ≥2 was detected. Moreover, each component of the EASIX and s-EASIX scores showed no relationship with CRS severity. Importantly, for the analysis of EASIX scores, we excluded bendamustine-treated patients (N = 6) to minimize confounding as they had elevated EASIX scores compared to Flu/CTX-treated individuals. The total number of patients after this adjustment equaled 59. We did not make any adjustments for gender due to sample size limitations. The gender variable was therefore included in the multivariable model assessed in the final step of the analysis.
Subsequently, we implemented maximally selected rank statistics technique to receive a cutoff value for EASIX-pre and s-EASIX-pre that accounts for maximally accurate CRS prediction. The test yielded estimated cutoff value of 1.835 for EASIX-pre score and 2.134 for s-EASIX-pre. Then, we employed two separate multivariable binary logistic regression models (with Firth correction) with CRS grade ≥3 as dependent variable. In the first model, predictor variables were categorical EASIX-pre (below and above the cutoff value of 1.835) and gender. In the second model, predictor variables were categorical s-EASIX-pre (below and above the cutoff value of 2.134) and gender. In the first model, EASIX-pre cutoff > = 1.835 associated with 4.59-fold increased OR of severe CRS (95% CI: 1.13–21.84, p = 0.033), whereas gender was not associated with the severity of CRS for women compared to men (p = 0.083). In the second model, s-EASIX-pre cutoff > = 2.134 associated with 4.13-fold increased OR of severe CRS (95% CI: 1.01–17.93, p = 0.01), whereas gender variable yielded non-significant result (p = 0.37). Figure 2 illustrates the distribution of CRS grades after categorization of the EASIX-pre and the s-EASIX-pre scores with the cutoffs. However, after internal validation with bootstrapping (number of resampling iterations = 1000) the significance was lost both for the EASIX-pre cutoff (95% CI: 0.98–21.4) and for s-EASIX-pre cutoff (95% CI: 0.73–23.26).
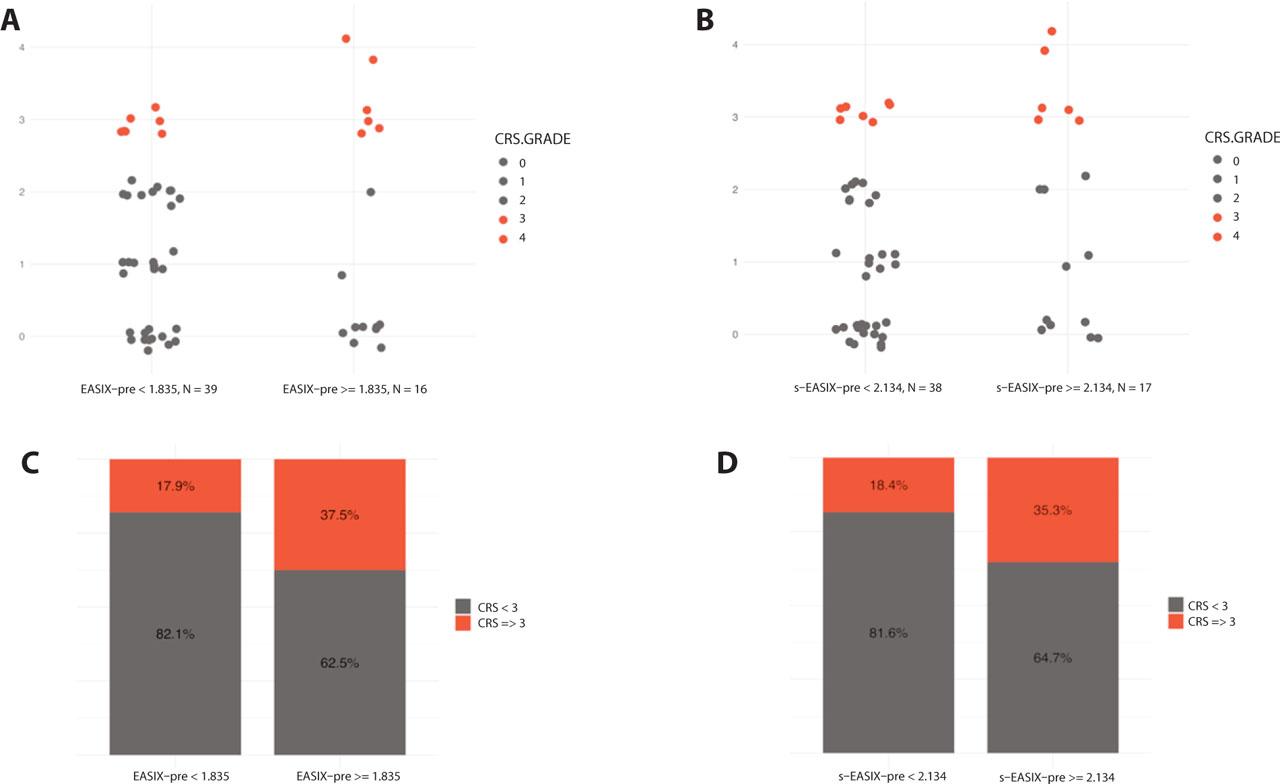
Association between categorized EASIX-pre/s-EASIX-pre scores and CRS grade. (A) Jitter plot depicting the distribution of the individual CRS grade cases, divided into two groups based on EASIX-pre cutoff of 1.835. Patients with higher EASIX-pre scores (equal or above the cutoff) are more likely to experience CRS grade ≥3 (OR = 4.59, 95% CI: 1.13–21.84, p = 0.033). (B) Jitter plot depicting the distribution of the individual CRS grade cases, divided into two groups based on s-EASIX-pre cutoff of 2.134. Patients with higher s-EASIX-pre scores (equal or above the cutoff) are more likely to experience CRS grade ≥3 (OR = 4.13, 95% CI: 1.01–17.93, p = 0.01). (C) Bar chart depicting percentage of CRS grade ≥3 based on EASIX-pre cutoff of 1.835. (D) Bar chart depicting percentage of CRS grade ≥3 based on s-EASIX-pre cutoff of 2.134. CRS, cytokine release syndrome; EASIX, Endothelial Activation and Stress Index; s-EASIX, simplified EASIX.
CAR-T cell therapy has become a standard-of-care for relapsed/refractory hematological diseases, including LBCL and MM. Along with its rapid commercialization, challenges associated with adverse event management remain the everyday routine of clinicians worldwide (Zhang et al. 2022; Tomasik et al. 2023). As the endothelial contribution to CRS became an appealing explanation of its pathogenesis, we found it sensible to assess the utility of the EASIX score as a CRS predictor. Due to its simplicity, it can be easily implemented in every center, and therefore it requires adequate validation that provides objective reports on EASIX’s performance with real-world data.
Until now, in the MM setting, the EASIX score was described as a prognostic factor for poorer overall survival (OS) in newly diagnosed patients (Song et al. 2020). Our findings suggest that the EASIX and s-EASIX scores may not have prognostic value when applied to MM/AL amyloidosis CAR-T patients as regression analyses yielded no significant results. This means that the increase in either EASIX or s-EASIX scores did not increase the odds of developing more severe CRS. Similar concerns were raised by Lee et al. (2024) who examined pre-lymphodepletion EASIX scores combined with ferritin and found no significant associations with CRS grades in CAR-T MM patients. Given the lack of relationship in our cohort, confirmation of potential prognostic value of the EASIX and s-EASIX scores may be impossible or would require large cohorts. Importantly, the effect size may be very small, and therefore of questionable clinical value. Apart from the assessment of the EASIX scores, we found that a bendamustine-based lymphodepletion regimen was associated with lower CRS grades. Interestingly, this relationship has not been confirmed in myeloma (Sidana et al. 2023). Therefore, our finding provides new insights into the impact of the lymphodepleting regimen on CRS development.
Contrary to anti-BCMA CAR-T therapies, reports on EASIX prognostic values are more common in LBCL. Similarly to MM, higher EASIX scores were associated with poorer OS in newly diagnosed patients (Park et al. 2022). Several teams addressed the use of the EASIX score for CRS prediction in CAR-T patients directly. Korell et al. (2022) published very promising results stating that the EASIX score measured before lymphodepletion gave significant OR (OR = 1.72, 95% CI: 1.26–2.46) for the prediction of grade ≥3 CRS/neurotoxicity. In the same study, the s-EASIX score calculated before lymphodepletion also gave significant results for grade ≥3 CRS/neurotoxicity (OR = 1.63, p = 0.004) (Korell et al. 2022). Moreover, the researchers estimated EASIX-pre cutoff values of 4.67 that are associated with 4.3-fold increased OR of severe CRS (Korell et al. 2022). Similar claims have been reported by Greenbaum et al. (2020, 2021) and Pennisi et al. (2021). Encouraged by the abovementioned findings, we evaluated prognostic values of EASIX and s-EASIX in patients treated against LBCL with tisa-cel (N = 55) or axi-cel (N = 10). Univariable binary logistic regression provided significant results for EASIX and s-EASIX scores before lymphodepletion (OR = 1.06, OR = 1.05, respectively), which means that the increase in either EASIX or s-EASIX scores increases the odds of developing severe CRS.
However, despite the result being in accordance with previously published papers, the OR is relatively small, which implies that EASIX and s-EASIX scores may not be powerful predictors of CRS. Nevertheless, we calculated the cutoffs of EASIX-pre and s-EASIX-pre scores that could constitute a reference value for the clinicians and estimate the ORs of severe CRS for patients being in high/low EASIX category. Subsequently, we estimated predictive power of this categorization with multivariable binary logistic models. The tests yielded cutoff of 1.835 for EASIX-pre that was associated with 4.59-fold increased OR of severe CRS, whereas s-EASIX-pre cutoff equaled 2.134 and was associated with 4.13-fold increased OR of severe CRS. Impact of gender turned out to be non-significant. The abovementioned results are partially in accordance with Korell et al. (2022) who reported similar odd ratios (OR = 4.3) but with higher cutoff value (4.67) for EASIX-pre score. However, we must point out that after internal validation with bootstrapping (number of resampling iterations = 1000) the significance of the results was lost both for the EASIX-pre cutoff and s-EASIX-pre cutoff. Perhaps this could be attributed to a small sample size, and we cannot deny that with larger cohorts, significance would appear also in validation process.
It is important to emphasize the potential shortcomings of our study. First and foremost, the sample size is rather small in both MM/amyloidosis and LBCL cohorts, whereas regression models require large groups. Moreover, the anti-BCMA analysis was based on patients receiving academic CAR-T product, not the commercially available ones. Therefore, we must be careful, when extrapolating the findings on anti-BCMA CAR-T cells in general. Hence, despite the results showing no predictive power of EASIX and s-EASIX scores in the MM/AL amyloidosis cohort, one should interpret the study output with caution. Other reports, especially on commercially available CAR-T cells, are necessary to validate our results.
In this multicenter retrospective study, we demonstrate that EASIX and s-EASIX scores should be employed with caution when concerning their utility in CRS prediction. Along with other researchers, we found the significant prognostic value of the EASIX and s-EASIX scores (before lymphodepletion) for CRS grade ≥3 in the LBCL CAR-T cohort. On the contrary, these scores seem to have no value in the prediction of CRS in MM/amyloidosis CAR-T patients.
Additionally, we provide new insights into the understanding of the relation between lymphodepleting regimen and CRS severity.