
Figure 1

Figure 2

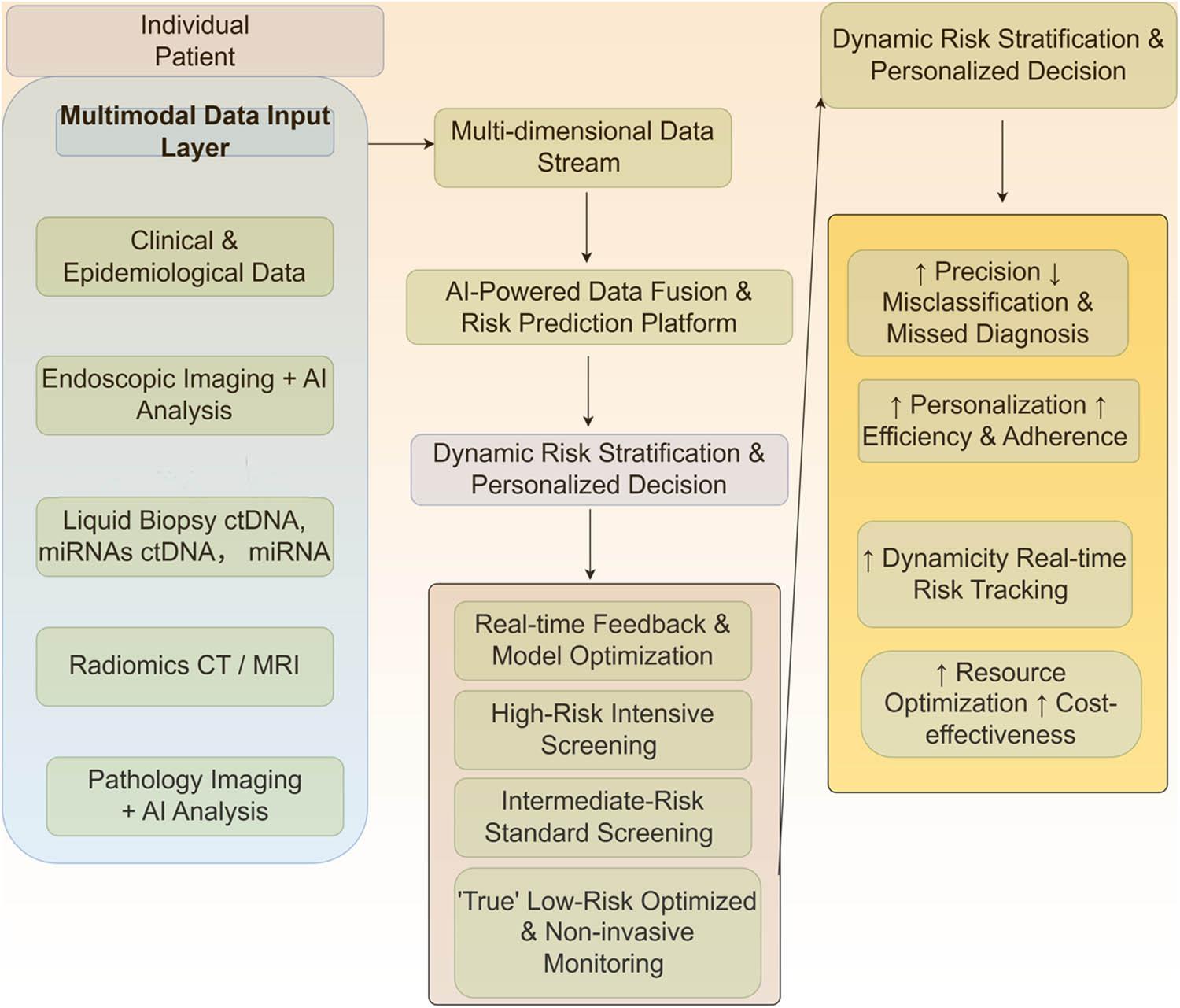
Figure 3
Comparison of major novel scoring systems for gastric cancer screening
| Scoring system name | Core components/variables | Risk stratification | Performance (Sensitivity/Specificity) | Target population | Key characteristics regarding missed diagnosis risk |
|---|---|---|---|---|---|
| NGCS | Age, Sex, H. pylori antibody, Pepsinogen I/II, Gastrin-17 | Low, Intermediate, High | AUC ∼0.79 | Chinese population in high-risk regions | A small but non-negligible proportion 0.94% of gastric cancers are detected in the low-risk group |
| New ABC method | H. pylori antibody, Pepsinogen I/II ratio | Groups A, B, C, D | High Negative Predictive Value (NPV >97%) | Multi-ethnic populations | The missed diagnosis rate in the low-risk group (Group A) is very low but not zero |
| GC-RSS | Age, BMI, Smoking, Dietary habits, Family history, etc. (Questionnaire-based) | Risk Score/Percentile | AUC >0.70 | Urban residents | Relies on subjective recall; susceptible to missing occult lesions in individuals with atypical presentations |
| OLGA/OLGIM staging | Histological staging of atrophy (OLGA) and intestinal metaplasia (OLGIM) | Stages 0–IV | Correlates with cancer risk | Patients undergoing endoscopy with biopsy | The ‘low-risk’ stages (0–II) still carry a potential, albeit lower, risk of progression. Risk is dependent on biopsy sampling quality and interpretation |
Key contributing factors to the risk of missed diagnosis in low-risk populations
| Factor category | Specific mechanisms | Representative references |
|---|---|---|
| Scoring system design flaws |
| [11,48,50] |
| Occult biological characteristics of GC |
| [24,26,28,32,35] |
| Insufficient sensitivity of biomarkers |
| [38,39,42,44] |
| Limitations in clinical screening practices |
| [52,53,55,59,60,61] |
| Deficiencies in screening strategy and system |
| [22,63,64,71] |
Future strategies and technological directions for mitigating missed diagnosis
| Strategic direction | Specific approaches/Technologies | Anticipated benefits/Outcomes |
|---|---|---|
| Optimization of scoring systems |
| Enhanced precision in identifying high-risk individuals within broadly classified low-risk cohorts |
| Integration of multimodal screening |
| Increased sensitivity for detecting early and occult lesions, leading to a higher early detection rate |
| Development of personalized screening pathways |
| Improved cost-effectiveness and resource allocation; reduced unnecessary procedures for true low-risk individuals |
| Implementation of multidisciplinary collaboration (MDT) |
| Improved diagnostic accuracy for borderline or complex cases through comprehensive review |
| Standardization of training and quality control |
| Minimization of operator-dependent errors and improvement in the overall quality and consistency of screening |