
As one of the malignant tumors with high incidence and mortality rates globally, GC remains a significant challenge in the field of public health. According to the latest epidemiological data, there are significant differences in the incidence of GC across different regions, with particularly heavy burdens in high-incidence countries in Asia, such as China, Japan, and South Korea [1,2]. Although the overall incidence of GC is lower in the United States, there is a noticeable increase in incidence and mortality among non-white populations and new immigrants from high-incidence countries, closely associated with the high prevalence of Helicobacter pylori infection and its associated gastric mucosal lesions in these groups [1]. H. pylori infection is a major risk index for the development of GC. It gradually promotes the occurrence of GC through the initiation of precancerous lesions such as chronic gastritis, atrophic gastritis, intestinal metaplasia, and atypical hyperplasia [3,4]. Furthermore, recent years have shown an increasing incidence of GC among younger populations, which may reflect the involvement of various factors such as lifestyle, environmental factors, and autoimmune status, thereby increasing the complexity of GC prevention and control [5,6].
Early screening is a key strategy for reducing GC mortality and improving patient prognosis. Asian countries have confirmed the significant benefits of endoscopic monitoring in increasing the detection rates of early GC and reducing GC-related mortality [1]. For example, in the national cancer screening programs of Japan and South Korea, endoscopic screening has become a primary method, significantly improving the detection rates of early GC and facilitating timely treatment [7,8]. However, traditional screening methods have certain limitations, such as the invasiveness of endoscopic examinations, resource and personnel constraints, and insufficient patient compliance. Particularly in low-risk populations, the cost-effectiveness of screening is low, and the risk of missed diagnoses is more pronounced. Additionally, single serum biomarker tests, such as H. pylori-specific antibody tests and pepsinogen (PG), although having some risk stratification function, still have limited sensitivity and specificity in low-risk populations, posing a risk of missed diagnoses [9].
To address these issues, new GC screening scoring systems have emerged in recent years. These systems aim to construct comprehensive risk assessment models by integrating indicators such as age, gender, H. pylori infection status, and serum biomarker levels (e.g., PGI, PGII, and G-17) to achieve precise screening and risk stratification for GC and its precursors [10,11,12]. The validation of these GC screening scoring systems in different populations shows that they can effectively distinguish low, medium, and high-risk groups, improving the detection rates of GC and early lesions, thus enhancing screening efficiency [10,11]. However, GC screening in low-risk populations still faces many challenges. On one hand, the low incidence of GC in low-risk populations limits the sensitivity of screening, making it prone to missed or misdiagnosis. Furthermore, the complex mechanisms underlying GC involve factors such as changes in the immune microenvironment, making it difficult for a single scoring system to comprehensively reflect individual risk.
The mechanisms of missed diagnosis risk mainly include insufficient recognition of latent lesions by the scoring system; unidentified risk factors existing in low-risk populations; and the inherent sensitivity limitations of the screening tools themselves. For example, some GC patients may be classified as low-risk but have latent atrophy in their gastric mucosa. Moreover, the dynamic changes in H. pylori infection status, individual immune status, and genetic background also affect the predictive performance of the scoring system. Factors influencing missed diagnoses also include the technical level of endoscopic examinations, image recognition capabilities, and patient cooperation in clinical operations.
In summary, the epidemiological background of GC shows that it remains a significant health burden globally; early screening is crucial for reducing GC mortality. Although traditional screening methods are effective, they face resource limitations and risks of missed diagnoses. New GC screening scoring systems provide new ideas for risk stratification and precise screening through multi-indicator comprehensive assessments. However, the issue of missed diagnoses in low-risk populations remains prominent, with mechanisms involving the limitations of the scoring system itself and the complex pathogenesis of GC. Next, the study will focus on optimizing the sensitivity and specificity of scoring systems, integrating advanced imaging technologies and biomarkers to enhance the early detection rate of GC in low-risk populations, ultimately achieving individualized and precise GC screening strategies. This article aims to systematically review the mechanisms and influencing factors of missed diagnosis risk in low-risk populations using new GC screening scoring systems, providing a theoretical basis and reference for subsequent research and clinical practice.
A systematic literature search was conducted to identify relevant studies on GC screening scoring systems and missed diagnosis risk in low-risk populations. The following databases were searched: PubMed and Web of Science, covering the period from January 2019 to December 2025. The search strategy combined terms related to GC (“gastric cancer” OR “stomach cancer”), screening (“risk score” OR “risk assessment” OR “sensitivity and specificity”), and missed diagnosis (“missed diagnosis” OR “underdiagnosis” OR “screening failure”).
Inclusion criteria were (1) studies evaluating risk scoring systems for GC screening; (2) studies reporting missed diagnosis rates or related mechanisms in low-risk populations; (3) original research articles, systematic reviews, or meta-analyses; and (4) articles published in English. Exclusion criteria included case reports, conference abstracts, editorials, and studies focused solely on treatment or prognosis without relevance to screening.
Three independent authors screened titles and abstracts, followed by full-text assessment. Disagreements were resolved through discussion or consultation with a fourth author. The reference lists of included articles were manually searched for additional relevant studies. This methodology ensures a comprehensive and transparent approach to synthesizing the current evidence on missed diagnosis risks in GC screening scoring systems.
Multifactor risk models play a central role in the design of GC screening scoring systems. Their construction typically integrates various types of risk indicators, including clinical characteristics, endoscopic findings, biomarkers, lifestyle factors, and epidemiological factors. Clinical indicators such as age, gender, smoking history, dietary habits (high salt, preserved food intake), and family history have been confirmed to be closely related to the occurrence of GC and its precursors [12,13]. In terms of endoscopic findings, gastric mucosal atrophy, intestinal metaplasia, and changes in gastric mucosal color and texture are included in the risk assessment system. Some scoring systems also incorporate pathological staging standards such as OLGA/OLGIM to enhance the ability to identify precancerous lesions [11,14]. Regarding biomarkers, serological pepsinogen I (PGI), pepsinogen II (PGII), PGI/PGII ratio (PGR), gastrin-17 (G-17), and H. pylori infection status have been widely confirmed as objective indicators reflecting gastric mucosal status and cancer risk, significantly improving the accuracy of risk stratification [11,13]. Additionally, some novel models have introduced inflammatory response indicators, nutritional status scores, and molecular markers to achieve more refined risk prediction [15,16].
In terms of weight allocation of scoring indicators and statistical methods, mainstream models often use multivariate regression analysis (e.g., Logistic regression, Cox proportional hazards model), LASSO regression, and other statistical tools to select independent risk factors and determine their weight coefficients [17,18,19]. The setting of weights for each indicator is usually based on their contribution to the risk of GC occurrence (e.g., OR value and HR value), converted into scoring item values through regression coefficients to achieve quantification and classification. For example, some models use high-risk factors (such as age ≥ 60 years, H. pylori positive) as variables in the risk scoring system, while low-risk factors (such as regular vegetable intake) are treated as protective factors [13]. The ability of the scoring system to distinguish different risk populations is evaluated through receiver operating characteristic (ROC) curve analysis and area under the curve (AUC) value calculation [10,17].
It is important to note that the effectiveness of the scoring system depends not only on the sensitivity of individual indicators but also on the overall risk discrimination ability under the synergistic effect of multiple indicators. For instance, studies have shown that integrating serological indicators with clinical epidemiological characteristics and other multidimensional information can significantly improve the detection rate of early GC and precancerous lesions [10,11]. The application of such multifactor models may provide a theoretical basis and practical pathway for achieving individualized and precise GC screening in the future.
Overall, the design of a scientifically sound scoring system should be based on a large sample, multicenter data, utilizing rigorous statistical methods to select and weight various risk indicators, and continuously validating their effectiveness and generalizability through external cohorts. This not only helps optimize screening resource allocation but also reduces the risk of missed diagnoses in low-risk populations, enhancing the overall level of early diagnosis and treatment of GC.
In recent years, new scoring systems for GC screening and risk assessment have emerged, aimed at improving the detection rate of early GC and its precursors, optimizing resource allocation, and are particularly suitable for stratified management of high-risk and low-risk populations. These scoring systems are often based on multidimensional variables such as clinical epidemiological data, serological indicators, lifestyle, and genetic risk factors, and are constructed and validated using statistical modeling or machine learning methods.
Representative scoring systems include the New GC Screening scoring system (NGCS), the new ABC method, the OLGA/OLGIM staging system, and multifactor scoring tools based on serological indicators and lifestyle (Table 1). For example, the NGCS integrates indicators such as age, gender, serum H. pylori antibodies, PGI, PGII, PGI/II ratio, and gastrin-17 to stratify subjects into low, medium, and high-risk groups with scores ranging from 0 to 23. Multiple clinical studies have shown a good correlation between the NGCS and the OLGA/OLGIM histological staging systems (specific data range of correlation coefficients not detailed), effectively distinguishing the detection rates of GC and atrophic gastritis among different risk-level populations, with the detection rate in the high-risk group significantly higher than that in the low-risk group [11]. Notably, the application of the NGCS in high-incidence areas of China has shown extremely high cost-effectiveness, significantly increasing the detection rate of early GC and helping to save long-term healthcare resource expenditures [20]. Therefore, the stratified screening strategy based on the NGCS is not only suitable for high-risk areas but also provides a theoretical basis for individualized screening in low-risk areas.
Comparison of major novel scoring systems for gastric cancer screening
| Scoring system name | Core components/variables | Risk stratification | Performance (Sensitivity/Specificity) | Target population | Key characteristics regarding missed diagnosis risk |
|---|---|---|---|---|---|
| NGCS | Age, Sex, H. pylori antibody, Pepsinogen I/II, Gastrin-17 | Low, Intermediate, High | AUC ∼0.79 | Chinese population in high-risk regions | A small but non-negligible proportion 0.94% of gastric cancers are detected in the low-risk group |
| New ABC method | H. pylori antibody, Pepsinogen I/II ratio | Groups A, B, C, D | High Negative Predictive Value (NPV >97%) | Multi-ethnic populations | The missed diagnosis rate in the low-risk group (Group A) is very low but not zero |
| GC-RSS | Age, BMI, Smoking, Dietary habits, Family history, etc. (Questionnaire-based) | Risk Score/Percentile | AUC >0.70 | Urban residents | Relies on subjective recall; susceptible to missing occult lesions in individuals with atypical presentations |
| OLGA/OLGIM staging | Histological staging of atrophy (OLGA) and intestinal metaplasia (OLGIM) | Stages 0–IV | Correlates with cancer risk | Patients undergoing endoscopy with biopsy | The ‘low-risk’ stages (0–II) still carry a potential, albeit lower, risk of progression. Risk is dependent on biopsy sampling quality and interpretation |
In terms of sensitivity and specificity, several studies have compared the NGCS with the traditional new ABC method. Specifically, the studies found that the detection rate of GC in the high-risk group using the NGCS can reach 14.3%, while it is only 0.3% in the low-risk group, demonstrating good risk differentiation ability. The NGCS shows even higher detection rates for atrophic gastritis and GC in the medium-high risk group, and it is strongly correlated with the grading of endoscopic pathological results (Gamma coefficient analysis P < 0.01), with the area under the ROC curve (AUC) reaching 0.79, indicating its high discriminative efficacy in practical screening [10,21]. A multidimensional scoring system developed for urban residents (e.g., GC-risk scoring system III) achieved an AUC of 0.714 in external validation, demonstrating good screening capability [22]. The clinical validation results of these systems show that both sensitivity and specificity are at a high level, effectively screening high-risk individuals and reducing the missed diagnosis rate.
Some scoring systems also incorporate factors such as lifestyle, dietary habits, and medical history. For example, the GC-RSS (GC Risk Scoring System) includes nine indicators through questionnaire surveys, such as age, gender, BMI, family history, smoking, drinking, salty foods, and pickled foods, with AUCs exceeding 0.70 in multiple validation groups. By setting different risk cut-off values, it can effectively save endoscopy resources and improve screening efficiency [12]. In addition, some studies based on large sample prospective cohorts further propose that combining scoring systems for stratified screening can achieve individualized starting ages for screening, allowing low-risk populations to delay screening while recommending earlier endoscopy for high-risk populations, thereby optimizing resource allocation for screening [23].
In summary, these new scoring systems have undergone sufficient clinical validation in multi-center large samples in China and other high-incidence areas, demonstrating high sensitivity, specificity, and practical application value. With the introduction of more serological, genetic, and lifestyle factors, the stratification capability of the scoring systems is expected to be further enhanced. In the future, research on the mechanisms of missed diagnoses in low-risk populations will deeply explore their occurrence mechanisms while systematically analyzing influencing factors, which will provide strong support for improving screening strategies and reducing GC mortality.
The application of scoring systems in GC screening, especially between high-risk and low-risk populations, shows significant differences in risk stratification and screening effectiveness. High-risk populations are typically evaluated based on multiple factors such as age, sex, H. pylori infection, family history, dietary habits (e.g., high salt intake, consumption of pickled foods), and smoking history, forming risk scoring models. For instance, some studies have adopted a novel scoring system that includes variables such as age, sex, pepsinogen ratio, gastrin-17, and H. pylori infection, categorizing the population into low-, medium-, and high-risk groups, with the detection rate of GC in the high-risk group significantly higher than that in the low-risk group [10,13]. This stratification not only helps optimize the allocation of resources like endoscopes but also enhances the specificity and effectiveness of screening.
Regarding the practical application of scoring systems in low-risk populations, several studies have found that these systems can effectively identify true low-risk individuals, thereby reducing unnecessary invasive examinations. For example, the ABC method, which combines serological H. pylori antibody testing and pepsinogen detection, maintains a high negative predictive value (NPV) across different H. pylori CagA statuses and subpopulations, especially in the low-risk group (e.g., Group A, where both tests are negative), where the detection rate of GC and its precursors is extremely low, with an NPV reaching 97–100% [24]. Similarly, a novel scoring system developed for the Chinese population showed a 0% detection rate of GC in the low-risk group, significantly lower than that in the medium and high-risk groups [10,13]. This indicates that applying scoring systems in low-risk populations helps alleviate the burden of endoscopic examinations and improves the cost-effectiveness of screening.
However, it is worth noting that while the risk of missed diagnoses in low-risk populations is low, it is not zero. Some studies have reported a very small number of GC or precancerous lesions detected in the low-risk group [21]. This suggests that although scoring systems can significantly reduce the probability of missed diagnoses, they still need to be combined with epidemiological characteristics, follow-up strategies, and individualized assessments to ensure that high-risk individuals are not overlooked. In comparing different scoring systems, some novel systems had lower detection rates of precancerous lesions in low-risk groups than the traditional ABC method, but higher detection rates in medium-risk groups, indicating differences in sensitivity and specificity of various scoring tools in risk stratification, which provides a basis for optimizing screening strategies in low-risk populations [21]. Among these, key contributing factors to the risk of missed diagnosis in low-risk populations were shown in Table 2.
Key contributing factors to the risk of missed diagnosis in low-risk populations
| Factor category | Specific mechanisms | Representative references |
|---|---|---|
| Scoring system design flaws |
| [11,48,50] |
| Occult biological characteristics of GC |
| [24,26,28,32,35] |
| Insufficient sensitivity of biomarkers |
| [38,39,42,44] |
| Limitations in clinical screening practices |
| [52,53,55,59,60,61] |
| Deficiencies in screening strategy and system |
| [22,63,64,71] |
Overall, the application of GC screening scoring systems in high- and low-risk populations reflects the scientific and practical nature of risk stratification, yet their efficacy in low-risk populations is compromised by a residual rate of missed diagnoses. As delineated in Figure 1, these diagnostic failures are not stochastic but result from a deterministic interplay of model imperfections (e.g., suboptimal variable weighting), the covert pathogenesis of indolent tumors, and the finite sensitivity of current screening modalities. The forthcoming integration of big data analytics and artificial intelligence offers a transformative pathway to deconvolute this complexity, promising the development of next-generation screening tools with superior discriminative power for the precise early detection of GC.
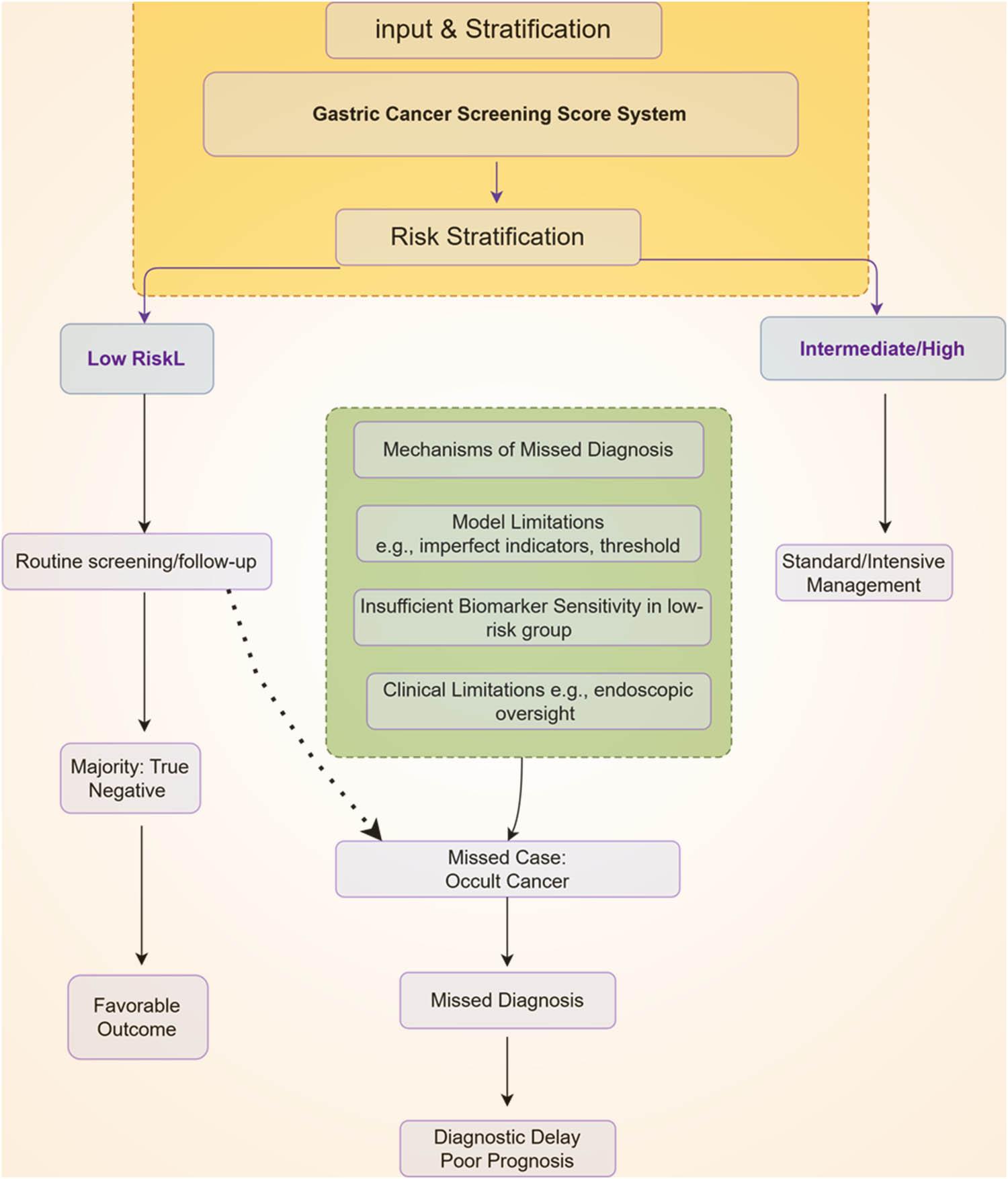
This schematic illustrates the application workflow of novel gastric cancer screening score systems and the risk mechanisms underlying missed diagnoses in low-risk populations. Following stratification by the scoring system, individuals assigned to the low-risk group undergo routine follow-up, among whom the vast majority are true negatives with favorable outcomes. However, due to multiple interconnected mechanisms – including inherent model design flaws, the occult biological characteristics of certain gastric cancers, insufficient sensitivity of biomarkers in this population, and limitations in clinical practice (delineated in the right panel) – a subset of occult cancers is misclassified into the low-risk group. This ultimately results in missed diagnosis, diagnostic delay, and worsened prognosis
The early lesions of GC in low-risk populations are characterized mainly by the diversity of pathological morphology and molecular features. The occurrence of GC typically goes through stages such as chronic inflammation, atrophic gastritis, intestinal metaplasia (GIM), atypical hyperplasia, and early carcinogenesis. For low-risk populations, the progression of early lesions like GIM is relatively slow, and the annual risk of progression to gastric adenocarcinoma is low (approximately 0.25–2.5%). However, some cases with high-risk pathological features (such as multifocality, extensive or incomplete GIM) still have a higher risk of carcinogenesis [25]. Furthermore, early lesions of GC in low-risk populations often present as hidden and asymptomatic, with small lesion size and high differentiation, making them difficult to identify through imaging and endoscopy, which increases the risk of missed diagnoses. Standardized biopsies and systematic mucosal sampling are crucial for detecting early lesions; however, in actual screening, they are often affected by factors such as operational standards, technical levels, and uneven distribution of lesions, further increasing the likelihood of missed diagnoses [26]. Due to the lack of typical clinical manifestations and visible mucosal abnormalities in GC among low-risk populations, the sensitivity of traditional screening methods is limited, necessitating the incorporation of molecular markers and novel risk scoring tools to enhance early identification rates (Table 3).
Future strategies and technological directions for mitigating missed diagnosis
| Strategic direction | Specific approaches/Technologies | Anticipated benefits/Outcomes |
|---|---|---|
| Optimization of scoring systems |
| Enhanced precision in identifying high-risk individuals within broadly classified low-risk cohorts |
| Integration of multimodal screening |
| Increased sensitivity for detecting early and occult lesions, leading to a higher early detection rate |
| Development of personalized screening pathways |
| Improved cost-effectiveness and resource allocation; reduced unnecessary procedures for true low-risk individuals |
| Implementation of multidisciplinary collaboration (MDT) |
| Improved diagnostic accuracy for borderline or complex cases through comprehensive review |
| Standardization of training and quality control |
| Minimization of operator-dependent errors and improvement in the overall quality and consistency of screening |
In terms of molecular marker expression, GC in low-risk populations exhibits significant heterogeneity. Studies have shown differences in molecular characteristics (such as HER2, MSI) between early-onset GC and late-onset GC [27]. For instance, early-onset GC (EOGC) often has a lower HER2 positivity rate and a smaller proportion of MMR defects, indicating that its molecular pathways differ from those of traditional late-onset GC. Patients with wild-type TP53 have poorer prognoses, suggesting that a single molecular marker may not comprehensively reflect the biological behavior of GC [28]. Molecular features related to the tumor microenvironment, such as tumor-associated neutrophils (TANs) and TGF-β signaling pathway activity, show significant differences between subtypes. These features not only affect tumor immune evasion and progression but also influence the sensitivity to immunotherapy [29,30]. The molecular phenotypes of some low-risk population patients overlap with high-risk subtypes, indicating that even under low-risk screening stratification, high-risk signals at the molecular level should be monitored.
The differences in molecular markers provide new insights for screening and risk stratification of GC in low-risk populations. Several studies have developed risk models based on multi-omics characteristics such as gene expression, lncRNA, proteomics, and metabolomics to predict the risk and prognosis of GC. These models integrate various molecular indicators (such as RNA-binding proteins, age-related genes) and clinical features to stratify risk within populations [31,32]. For example, the ABC method based on serum pepsinogen and H. pylori antibodies has shown high negative predictive values across different CagA subtypes and populations, effectively identifying true low-risk individuals and reducing unnecessary endoscopies [24]. However, the universality of a single molecular marker or scoring system across different populations and molecular subtypes requires further validation, and future efforts should focus on optimizing screening strategies through large-scale, multi-center, prospective studies.
In summary, GC in low-risk populations exhibits high heterogeneity at both pathological and molecular levels, making early lesions difficult to identify, with significant differences in molecular markers and existing screening methods posing risks of missed diagnoses. Future efforts should strengthen multi-omics integrative analysis, combining molecular markers and clinical scoring systems to enhance the identification capabilities and screening efficacy of early GC in low-risk populations.
The early development of GC in low-risk populations is highly concealed, characterized by the small size of tumors, lack of obvious clinical symptoms, and difficulty in detection through conventional imaging examinations. This characteristic greatly affects the effectiveness of early screening and diagnosis. Research has found that even among GC patients classified as early stage (such as cT1-2, cN0), a considerable proportion is found to have concealed peritoneal metastasis or cancer cell dissemination during laparoscopic staging and peritoneal cytology examinations. For example, a large sample prospective cohort study showed that approximately 17.9% of patients with early GC were diagnosed with peritoneal cancer lesions or positive cytology through laparoscopic examination. The study also revealed that these concealed metastases are significantly associated with patient prognosis [33]. Moreover, some early GC patients, even without lymph node metastasis, ultimately die due to tumor recurrence or distant metastasis, indicating a potential risk of misjudgment in traditional imaging and clinical staging [34]. The mechanisms of concealed progression of GC in low-risk populations involve multiple aspects, including the micro-clonal expansion of tumor cells, histological multi-directional differentiation tendencies, and even multi-directional differentiation and invasive capabilities under monoclonal origin. For instance, rare cases of early gastric sarcoma demonstrate that even when the tumor volume is small, and invasion is limited to the submucosa, local recurrence can still occur due to the presence of multi-directional differentiation components and germ cell-like cells [35]. This evidence suggests that the genetic and phenotypic diversity of tumor cells provides a biological basis for their concealed progression during the early development of GC. Combined with the above data, it is evident that even in low-risk populations or early stages, GC still has a high probability of achieving concealed extension through small lesions or special molecular subtypes, which poses higher demands for the sensitivity of screening technologies and interventions like molecular detection.
The tumor microenvironment and immune evasion mechanisms are key contributors to the early, clinically occult progression of GC. These processes operate synergistically to promote tumor advancement in a stealth manner. In particular, gastric carcinogenesis is frequently driven by chronic inflammatory conditions within the local microenvironment, most notably those induced by H. pylori infection. Such inflammatory settings do not merely represent a persistent immune response but actively facilitate tumor initiation and malignant progression [36,37]. Additionally, tumor cells can escape recognition and elimination by the immune system during the early stage through the expression of immune checkpoint molecules such as programmed death-ligand 1 (PD-L1), downregulation of antigen-presenting molecules, and secretion of immunosuppressive factors, thus achieving “immune invisibility.” Relevant studies show that changes in inflammatory biomarkers in the peripheral blood of early GC patients are not significant, indicating the limitations of inflammatory markers in early disease detection [38]. Meanwhile, the microenvironment of GC also includes tumor-associated fibroblasts, vascular endothelial cells, and various immunosuppressive cells, which together shape an ecological niche that supports the concealed growth and metastasis of tumors. Notably, the synergistic effect of chronic inflammation and immune suppression in the microenvironment not only increases the survival of tumor cells but also reduces the expression levels of early screening biomarkers, increasing the risk of misjudgment.
In low-risk populations, the mechanisms of concealed progression of GC are also closely related to molecular subtypes, tumor genetic variations, and epigenetic regulation. Recent histological and molecular biology studies have found that biallelic inactivation of tumor suppressor genes such as TP53 is a common event in the early occurrence of GC, and this genetic abnormality can drive cells to evolve highly genomic unstable and clonal advantage subgroups. Through long-term evolutionary experiments using human gastric organoid models, researchers found that TP53 deletion can lead to the gradual acquisition of structural variation characteristics such as polyploidy, chromosomal rearrangements, and copy number variations, and form concealed subclones with malignant transformation potential under microenvironmental selective pressure [39]. These subclones are difficult to identify early under clinical imaging or conventional histological examinations but possess strong survival and dissemination capabilities. Therefore, even in a low-risk context, specific molecular events may endow tumor cells with the ability for concealed progression and early metastasis (Figure 2).
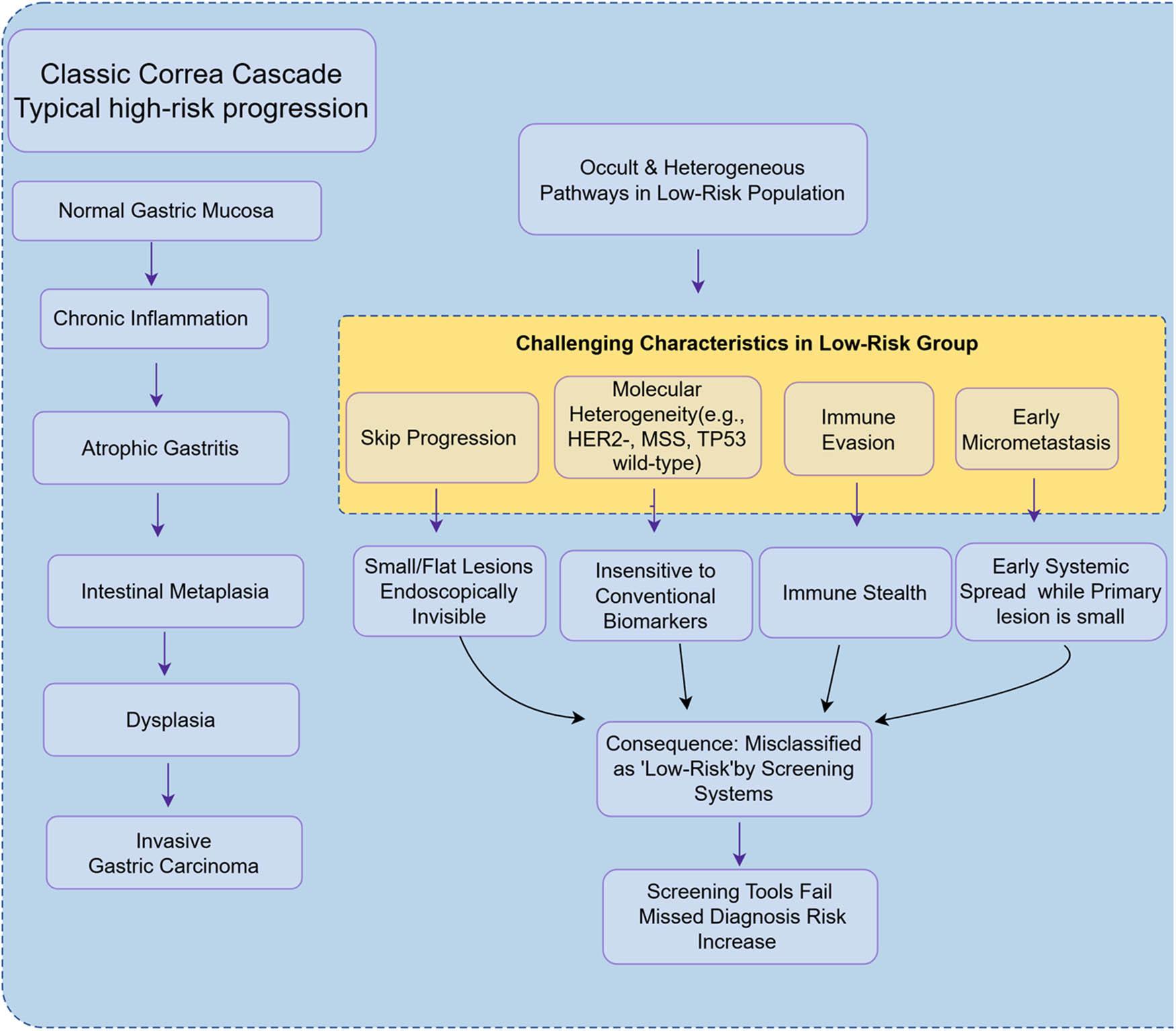
The occult biological characteristics of gastric cancer in low-risk populations and their challenges to screening. This figure contrasts the classic Correa cascade of gastric carcinogenesis (left) with the occult biological features observed in low-risk populations (right). In these individuals, gastric cancer may develop through atypical pathways, including skip progression, distinct molecular heterogeneity (e.g., HER2-negative, microsatellite stable [MSS], TP53 wild-type status), immune evasion, and early micrometastasis. These characteristics result in tumors that are endoscopically inconspicuous and exhibit low sensitivity to conventional serological biomarkers. Consequently, they are prone to being misclassified as ‘low-risk’ by existing screening score systems, significantly increasing the risk of missed diagnosis
The application of biomarkers in GC screening has provided new possibilities for early detection and risk stratification, but their sensitivity and practicality in low-risk populations still face many limitations. Traditional gastric cancer biomarkers such as serum pepsinogen, carcinoembryonic antigen (CEA), and carbohydrate antigens (such as CA19-9) have certain screening value in some high-risk populations, but their sensitivity and specificity are generally low in low-risk populations. For example, while the positive status of PG has some effect on identifying high-risk individuals for non-cardia gastric cancer, its sensitivity in low-risk populations is only 44.3%, with a specificity of 93.6%, indicating a high risk of missed diagnoses [40]. Additionally, combinations of serum biomarkers such as GastroPanel® have not effectively distinguished between low-risk and high-risk patients in practical applications, with both sensitivity and accuracy being unsatisfactory [41]. These results indicate that current biomarkers struggle to meet the demand for large-scale screening in low-risk populations, which can lead to missed diagnoses of some early cases.
In recent years, the exploration of novel biomarkers has become a research focus aimed at improving screening sensitivity in low-risk populations. Researchers have attempted to integrate multi-omics biomarkers at the molecular level, including liquid biopsies, ctDNA methylation, miRNA, lncRNA, and proteomics, for early detection of GC. For example, fecal DNA methylation markers (such as SDC2, TERT, RASSF2, etc.) have shown higher accuracy in gastric cancer screening than fecal occult blood testing, with combined detection sensitivity reaching 78.6% for stage I gastric cancer [42]. Salivary metabolomics biomarkers (such as cytochromes) show significant differences between GC patients and healthy controls [43]. Furthermore, the detection of circulating miRNAs (such as miR-21, miR-135b, etc.) and ctDNA methylation has shown promising early diagnostic capabilities in some studies [44,45]. The introduction of multiplex testing for these novel markers and artificial intelligence algorithms is expected to compensate for the shortcomings of individual biomarkers in sensitivity.
However, the application of novel biomarkers in low-risk populations still faces numerous challenges. First, many marker studies are still in the preliminary stages, with limited sample sizes and a lack of large-scale, multi-center prospective validation, and their screening performance across different populations and disease spectra has not been fully confirmed [46]. Second, some molecular markers exhibit significant expression differences across different GC subtypes, stages of disease, and populations, leading to noticeable fluctuations in sensitivity and specificity during practical application. Additionally, liquid biopsy markers like ctDNA still have limited sensitivity when detecting single targets; some GC subtypes show weak correlations with ctDNA, and there are issues related to off-target risks and non-standardized detection criteria [45,47]. In low-risk populations, background diseases, inflammation, and infections may also interfere with the expression of biomarkers, further reducing the accuracy of screening.
Currently, although new technologies such as multi-omics integration, machine learning, and AI modeling provide a theoretical basis for improving screening sensitivity in low-risk populations, the relevant literature has not specifically reported on the concrete challenges faced in clinical translation [46,47]. In practical screening, using multi-biomarker combined detection along with stratification based on epidemiological risk factors is expected to somewhat increase the detection rate in low-risk populations, but the risk of missed diagnoses cannot be overlooked. With technological advancements and the promotion of large-scale cohort studies, novel biomarkers are expected to gradually optimize GC screening strategies for low-risk populations in the future, but their actual sensitivity and risk of missed diagnoses still require careful evaluation at this stage.
In summary, the existing biomarkers show insufficient sensitivity in low-risk populations, making it difficult to effectively avoid the risk of missed diagnoses. Although the combined application of new molecular and multi-omics biomarkers shows potential for enhancing sensitivity, their clinical value in low-risk populations still needs to be further validated by large-sample, multi-center studies, and future attention should be paid to practical application issues such as detection standards, cost-effectiveness, and population heterogeneity.
The absence of key indicators or unreasonable weight distribution in scoring systems is one of the significant mechanisms behind the risk of missed diagnoses in GC screening. Currently, some novel scoring systems primarily stratify risk based on epidemiological and clinical characteristics (such as age, gender, and smoking history), but the inclusion of certain biomarkers closely related to GC occurrence or specific high-risk factors is still inadequate. For example, research shows that a newly developed GC screening scoring system based on Chinese conditions can effectively distinguish high-, medium-, and low-risk populations in practical applications, yet there is still a 0.94% detection rate of GC in the low-risk group, indicating that some true GC patients are categorized as low risk, potentially missing early diagnosis and treatment opportunities [10]. This phenomenon may partly result from the scoring system’s failure to adequately consider the weight distribution of certain key indicators during design or from overlooking some strongly concealed risk factors. Additionally, the applicability of some scoring systems across different populations is also limited; for instance, in contexts where there are differences in ethnicity, region, or underlying disease spectra, the importance of certain indicators may be overestimated or underestimated, leading to risk assessment results that deviate from reality.
The lack of specific indicators for low-risk populations is also a significant factor contributing to the risk of missed diagnoses. Although traditional scoring systems show high sensitivity and specificity in high-risk populations, existing models often lack targeted biological or molecular markers for low-risk populations. For example, some models rely solely on epidemiological characteristics and routine laboratory indicators without integrating tumor-related gene variations, molecular subtypes, or emerging immunological markers [48]. Furthermore, in practical applications, the weight settings of scoring systems are often based on research data from high-risk populations, neglecting the influence of atypical presentations or new risk factors in low-risk populations, creating blind spots in risk assessment for the low-risk group.
It is worth noting that some studies have attempted to enhance the precision of risk prediction models by introducing new technologies such as electronic health records (EHR) and machine learning. For example, research has developed a GC risk prediction model based on EHR, finding that, besides traditional factors, certain comorbidities (such as anemia and specific ethnicities) in low-risk populations are associated with GC risk [49]. If these low-risk population-specific indicators could be integrated into existing scoring systems, it could significantly enhance the sensitivity and coverage of screening. In fact, with advances in molecular biology and multi-omics technologies, future scoring systems are expected to achieve more precise identification of potential risks in low-risk populations by integrating multidimensional information such as genetic, protein, and immune characteristics.
During the development of the scoring system, the lack of sample representativeness is one of the core factors affecting the model’s generalization ability and the risk of missed diagnoses. Current GC risk prediction models mostly rely on clinical or epidemiological data from specific regions or high-risk populations, leading to certain limitations in the sample structure during the model design. For example, a review systematically summarized GC risk prediction models worldwide and found that the variable selection and sample sources of most models focused on high-risk factors such as age, H. pylori infection, and precancerous lesions, with samples mainly coming from high-incidence areas like East Asia. Although these variables have good identification capabilities for high-risk populations, the relevant literature does not clearly state their representativeness and applicability in low-risk populations [50]. This bias in sample representativeness may lead to missed diagnoses of some hidden or atypical cases when the scoring system is applied to low-risk populations, affecting the fairness and effectiveness of screening.
The relative scarcity of data from low-risk populations further exacerbates the model’s lack of generalization ability. Most GC screening and risk assessment studies often focus on high-incidence areas or populations with obvious risk factors, while low-risk populations, due to low incidence and difficulties in sample collection, are often marginalized during the model training and validation phases. A review of 28 original risk prediction models found that although the AUC values of the models could reach 0.989, the model variables mainly concentrated on high-risk features [50]. This results in a decrease in the sensitivity of the scoring system in low-risk populations and an increase in the risk of missed diagnoses. Additionally, the lack of large sample, multi-center data from low-risk populations makes it difficult for the model to capture potential atypical risk factors or subtypes within low-risk groups, further limiting the model’s extrapolation ability.
In terms of data sources, some studies have attempted to use national health insurance databases or large-scale health examination data to enhance sample diversity and the model’s universality. For example, South Korea’s national health insurance system database includes census data for individuals over 40 years old, and GC prediction models developed using machine learning methods have also achieved high AUCs (0.749–0.800) in independent external cohorts, demonstrating some degree of generalization ability [51]. However, even so, the proportion of low-risk populations in the overall sample remains limited, and the model’s predictive performance and risk of missed diagnoses for low-risk subgroups still need further validation. Given the circumstances, if more high-quality data from general or low-risk populations can be incorporated into model development and validation in the future, it will help improve the fairness and accuracy of the scoring system.
It is worth noting that sample bias during model development may also be influenced by data collection methods, research design, and variable selection. For instance, most risk prediction models prioritize high-risk factors during variable selection, neglecting the unique risk characteristics that may exist in low-risk populations. Additionally, sample collection is often limited to single centers or specific regions, lacking extensive validation across multiple centers and regions. Although some studies have attempted to supplement external validation or multi-center data, the relevant literature has not clearly pointed out the limited sample size and event numbers in low-risk populations or biases in the models [50]. Therefore, future model designs should pay more attention to the balance and diversity of sample structures, especially the adequate representation of low-risk populations.
In summary, the scoring system faces dual challenges of insufficient sample representativeness and data scarcity when developed and applied to low-risk populations, which directly impacts the model’s generalization ability and the risk of missed diagnoses. Model developers need to focus on the inclusion and analysis of low-risk population samples, promoting multi-center, large-sample cohort studies to provide a solid foundation for enhancing the applicability and accuracy of GC screening scoring systems across the entire population.
The threshold setting of the scoring system in GC screening directly affects the sensitivity and specificity of the screening, thus influencing the missed diagnosis risk in low-risk populations. Current studies show that if the threshold of the screening scoring system is set too high, it can reduce the false positive rate and improve specificity, but it will significantly lower sensitivity, leading to some actual patients not being identified in a timely manner, thereby increasing the risk of missed diagnoses. For example, in the immunohistochemical detection of TP53 mutations, research compared data with NGS and found that different antibodies and different threshold settings had a huge impact on sensitivity and specificity. Taking the SP5 antibody as an example, a 20% threshold setting can achieve 100% sensitivity and specificity [52]. This indicates that the threshold setting of the scoring system must fully consider sensitivity, especially in low-risk populations, to avoid sacrificing early detection opportunities in pursuit of high specificity.
There is a close relationship between adjustments to scoring thresholds and missed diagnosis rates. Both modeling and actual cohort studies have shown that small changes in thresholds can lead to significant changes in missed diagnosis rates. In a large-sample risk stratification study based in China, by categorizing individual risk scores into quantiles, it was found that the starting age for screening in low-risk populations could be appropriately postponed, while high-risk populations needed to start screening earlier. If the scoring threshold is set too high, it may affect the choice of the starting age for screening [23]. Further analysis suggests that by quantifying multiple risk factors, the scoring system can reasonably adjust thresholds to dynamically balance the risk of missed diagnoses and the risk of excessive screening. Especially in low-risk populations, moderately lowering the threshold can help increase the detection rate of early cases and improve screening effectiveness.
The setting of scoring thresholds should also be dynamically adjusted in conjunction with the epidemiological characteristics and disease spectrum of specific populations. Some studies point out that the optimal thresholds of the scoring system vary for different age groups, comorbidities, and genetic backgrounds. For example, in a simulation of GC screening strategies based on the level of comorbidities in China, researchers evaluated 378 different combinations of starting and ending ages and comorbidities through micro-simulation models [53]. This reflects that the reasonable setting of scoring system thresholds should fully consider population heterogeneity and actual risk distribution, avoiding the potential neglect of cases in low-risk populations due to a “one-size-fits-all” approach.
Overall, setting the thresholds of the scoring system too high will lead to a decrease in sensitivity, thereby increasing the risk of missed diagnoses in low-risk populations. Reasonable threshold adjustments should aim to maximize screening benefits and reduce missed diagnosis rates, dynamically optimizing based on population risk characteristics. In the future, it is recommended to conduct prospective validation and sensitivity analysis for different populations before actual screening to determine the optimal threshold range, thereby enhancing the overall accuracy and practicality of the new GC screening scoring system.
Differences in endoscopic operation techniques and their impact on the identification of early lesions
Endoscopic screening plays a core role in the early detection of GC, but differences in operational techniques directly affect the lesion identification rate. Research shows that the experience and training level of endoscopists significantly impact screening results. For example, in high-incidence countries, certification and continuous education for endoscopists have been used to improve GC endoscopic screening [7]. However, the uneven distribution of endoscopists and their technical levels across regions leads to a lower detection rate of early lesions in certain areas. Additionally, the configuration of endoscopic equipment and imaging technology also affects diagnostic accuracy. High-resolution endoscopy and image enhancement technologies (such as Narrow Band Imaging (NBI) and magnifying endoscopy) can improve the ability to identify subtle and hidden lesions [54]. Some studies have found that even with advanced equipment, if the operational process is not standardized or the observation is insufficient, early lesions may still be missed [22]. Therefore, improving the standardization of endoscopic techniques and ongoing technical training for endoscopists is a key step in reducing the risk of missed diagnoses and enhancing screening quality. Considering the reality of varying technical levels, promoting AI-assisted endoscopic diagnosis in the future may help partially bridge the impact of human operational differences on screening outcomes [55].
The concealment of lesions during endoscopy and the risk of misdiagnosis.
Early GC and precancerous lesions often present as subtle changes in mucosal color, texture, or vascular structures during endoscopy, with some lesions even completely covered by normal or non-neoplastic mucosa, making them easily overlooked or misdiagnosed. Although magnifying endoscopy combined with Narrow Band Imaging has improved the detection rate of small lesions, diagnostic blind spots still exist. Research shows that approximately 10% of early GCs are missed during endoscopic examinations, with these missed lesions often being differentiated adenocarcinomas, low-grade atypical hyperplasia, or lesions completely covered by non-neoplastic mucosa [56]. Additionally, lesions with surface structures very similar to normal mucosa, mixed-type or partially covered lesions, also tend to lead to misdiagnosis. Misdiagnosis may also arise from benign lesions such as inflammation, erosion, or ulcers that exhibit similar endoscopic features to early cancer, increasing diagnostic difficulty. In practice, endoscopists’ subjective judgment of suspicious lesions heavily relies on experience, and the lack of systematic diagnostic algorithms and standardized processes further increases the risk of misjudgment [54]. Therefore, incorporating multimodal imaging, standardized diagnostic processes, and precise biopsy strategies can help reduce the missed diagnoses and misjudgments of concealed lesions. With the promotion of AI-assisted diagnostic systems, it is expected that in the future, we can enhance the sensitivity of lesion identification while reducing the incidence of human misdiagnosis [55].
Imaging examinations serve as important tools for screening and staging GC. In recent years, with advancements in technologies such as CT, MRI, and endoscopy, their resolution and quantitative capabilities have significantly improved. However, there are still certain resolution limitations in the clinical application of imaging examinations, particularly in the detection of early GC or small lesions. Studies show that although new technologies like multi-phase contrast-enhanced CT and diffusion-weighted MRI can improve lesion detection rates, the “double-track sign” seen on CT in early GCs such as T1a occurs only in some patients and has limited sensitivity, which may lead to missed diagnoses in some low-risk patients [57]. Additionally, functional imaging techniques like Diffusion Kurtosis Imaging (DKI) have shown high diagnostic value in predicting responses to neoadjuvant chemotherapy [58]. Thus, despite continuous advancements in imaging technology, current spatial resolution and the ability to identify small or early lesions still fail to fully meet the needs of early GC screening.
In terms of pathological diagnosis, endoscopic biopsy remains the gold standard for confirming GC, but the limitations of pathological sampling are also significant reasons for missed and misdiagnosed cases. First, diagnosing GC presents certain challenges, necessitating the use of imaging and AI assistance to improve accuracy [59]. Second, the preparation and interpretation of pathological slides are subjective, and traditional pathological analysis is time-consuming and prone to errors [60]. In recent years, AI-assisted pathological image analysis has improved diagnostic efficiency and consistency, but it still has shortcomings in terms of dataset diversity and model generalization [60].
It is worth noting that the limitations of imaging and pathological diagnosis are particularly pronounced in low-risk populations. The imaging characteristics of GC in low-risk populations pose differential diagnosis challenges with benign lesions such as gastritis [57]. Furthermore, there is a lack of unified standards for certain imaging and pathological indicators across different hospitals, equipment, and operators, increasing diagnostic variability and uncertainty. In the future, with the integrated application of multimodal imaging, panoramic digital pathology, and AI deep learning technologies, there is hope to enhance the detection rates and diagnostic accuracy of small lesions, but further research and optimization are needed for their promotion and standardization in low-risk populations.
In summary, while imaging and pathological diagnosis currently play an irreplaceable role in GC screening and classification, their resolution and sampling limitations are significant mechanisms contributing to the risk of missed diagnoses in low-risk populations. Future technological innovations and multi-center standardized collaborations are expected to gradually address these shortcomings, providing more accurate and comprehensive support for early GC screening in low-risk populations.
The experience and training level of physicians play a crucial role in the screening process for GC. Inexperienced physicians are prone to misjudgments during endoscopic examinations, leading to missed diagnoses of early GC or high-risk lesions. For example, a retrospective cohort study on GC patients showed that despite most patients having two or more risk factors for GC, only 27.5% underwent endoscopic screening prior to diagnosis. More importantly, the follow-up endoscopic examination rate for known high-risk lesions was extremely low, at only 14.3%[61]. This reflects a significant deficiency in physicians’ ability to identify and manage high-risk populations in clinical practice, which may partly relate to insufficient experience in endoscopic diagnosis and related knowledge.
During endoscopic procedures, the diagnostic skills of physicians directly affect the detection rate of lesions. Studies have shown that early GC, especially synchronous multiple early GC (SMEGC), is often overlooked due to small lesion size and subtle morphology (such as flat or depressed types). A prospective study involving 271 early GC patients found that the preoperative miss rate for SMEGC was as high as 43.2%, whereas incorporating a systematic gastric screening during endoscopic submucosal dissection (ESD) could reduce the miss rate by 24.3%[62]. This indicates that experienced endoscopists can effectively reduce blind spots and improve the detection rate of early and multiple lesions through standardized, multi-step operational protocols. Comprehensive research results indicate that in teams of experienced and systematically trained physicians, the detection capability for GC, particularly high-risk and subtle lesions, is significantly enhanced, further emphasizing the necessity of training and standardized procedures.
Standardized training not only includes the improvement of operational skills but also involves systematic learning about high-risk areas for GC, common lesion morphologies, and pathogenesis. Literature indicates that GC is commonly found in areas such as the gastric antrum and lesser curvature and that H. pylori-related atrophic changes often expand from these areas to the gastric body, making lesions in these regions more likely to be missed [63]. Therefore, physicians need to be familiar with the high-incidence areas of GC and the endoscopic manifestations of early lesions, and combine these with a systematic screening process to focus their examinations on critical areas during actual procedures. It is noteworthy that some high-risk populations, such as elderly patients and those with severe atrophic gastritis, are more likely to exhibit multiple and subtle lesions, placing higher demands on physicians’ diagnostic sensitivity and observational detail.
Additionally, with advancements in technology and the continuous application of new auxiliary tools, physicians need to keep updating their relevant knowledge and skills. The use of high-resolution endoscopy, virtual chromoendoscopy, and other new technologies enables experienced physicians to more accurately identify high-risk lesions [22]. However, the effective application of these technologies also relies on systematic training and the accumulation of practical experience. Physicians lacking standardized training and ongoing education may not fully leverage the diagnostic advantages of advanced equipment, thereby impacting the overall quality and efficiency of screening.
In summary, the experience and training level of physicians are directly related to the accuracy and miss rate of GC screening. Strengthening standardized training, continuous skill enhancement, and the implementation of standard operating procedures are key steps in improving the early detection rate of GC and reducing the risk of missed diagnoses. In the future, with the continuous application of new technologies, there will be higher demands on physicians’ professional competencies and training systems, making the ongoing optimization of training content and assessment standards an important guarantee for improving the quality of GC screening.
In low-risk populations, the screening interval for GC is often quite long, which directly increases the risk of missed diagnoses. Multiple studies through modeling simulations and actual follow-ups have found a negative correlation between screening frequency and the missed diagnosis rate. Taking China as an example, an economic and effectiveness evaluation of different screening frequencies using a Markov model showed that, regardless of the age at initial screening, screening every two years is the most cost-effective strategy. Especially in high-incidence areas or among older populations, screening every two years is the optimal strategy; whereas in low-incidence areas or low-risk populations, it is recommended to screen every five years to improve cost-effectiveness [64]. If the screening interval is further extended, it may lead to early lesions developing into advanced cancer; at the same time, it would also miss the best intervention timing. Considering the epidemiological context of different countries and regions, optimizing screening frequency is of significant importance in reducing the risk of missed diagnoses for GC. It is worth noting that in practice, certain populations exhibit inadequate screening compliance, such as low screening participation rates and untimely follow-ups [65].
The lack of a robust follow-up mechanism is also an important factor influencing missed diagnoses in low-risk populations. Even when initial screening results are negative, some individuals still have the potential to develop GC in the subsequent years. Without a systematic follow-up plan and risk reassessment mechanism, early lesions can easily be overlooked. Long-term cohort studies in South Korea analyzed the compliance and influencing factors of GC screening [65]. Additionally, the inadequacy of the follow-up mechanism is reflected in poor information feedback, low patient compliance, and inadequate follow-up reminders and tracking measures, leading to some high-risk transitions not being timely identified and intervened.
From the perspectives of health economics and public health management, reasonable screening frequency and improved follow-up mechanisms not only help reduce the overall burden of GC but also enhance the early diagnosis rate and survival rate. Existing research shows that there are differences in the cost-effectiveness of different frequencies of endoscopic screening for upper gastrointestinal cancers [66]. In low-risk populations, if precise stratified management can be achieved through big data and artificial intelligence, and if the follow-up mechanism can be upgraded intelligently, it is expected to further enhance the overall effectiveness of the screening system.
In summary, the long screening intervals and inadequate follow-up mechanisms in low-risk populations are key mechanisms leading to an increased risk of missed diagnoses. Therefore, optimizing screening frequency, strengthening follow-up management, and improving patient compliance and health awareness are core measures to reduce the missed diagnosis rate of GC and achieve early detection and intervention.
Currently, the GC screening strategies for low-risk populations mainly rely on demographic factors such as age, gender, and region, neglecting the differences among individuals in terms of genetics, environmental exposure, lifestyle, and underlying diseases. This “one-size-fits-all” screening model fails to adequately consider the heterogeneity within low-risk populations, leading to some truly high-risk individuals being misclassified as low-risk, potentially increasing the risk of missed diagnoses. For example, although the overall incidence rate in low-risk populations is low, there are individuals within this group who have risk factors such as family history, H. pylori infection, smoking, and obesity [67]. Moreover, the general population has low knowledge and compliance regarding GC screening, with major barriers being asymptomatic conditions and concerns about discomfort [68].
In recent years, several studies have emphasized the importance of establishing individualized risk assessment models for optimizing GC screening strategies. The traditional definition of screening age (e.g., starting at 50) has been shown to be inadequate in covering all high-risk individuals, while multi-factor risk scoring systems can more scientifically stratify the population. For instance, a large-scale prospective study in China integrated eight risk factors – age, gender, H. pylori infection, family history, previous gastric disease history, smoking, and alcohol consumption – to develop a personalized screening starting age calculator. The results showed that the screening starting age for low-risk populations could be postponed to 58 years, while high-risk populations should be screened by 46 years, significantly enhancing the effectiveness and resource utilization of screening [23]. Similarly, studies abroad have constructed predictive models that include clinical, demographic, and laboratory parameters, validating their effectiveness in screening risk stratification across different populations [69]. The introduction of these models not only aids in accurately identifying individuals who truly need early screening but also reduces unnecessary interventions in low-risk populations, improving the overall cost-effectiveness of screening [70].
It is noteworthy that some studies have incorporated genetic susceptibility into the risk assessment framework. Systematic reviews have shown significant associations between specific gene polymorphisms (e.g., MUC1, PSCA, TNF-α, etc.) and GC risk, with differences in genetic backgrounds among populations also influencing disease susceptibility. Therefore, future risk models are expected to integrate genetic information for more precise individualized screening [71]. Currently, online tools are already assisting in risk assessment and screening decision-making, promoting GC screening towards a more precise and effective individualized direction [23].
In conclusion, the individual differences within low-risk populations are overlooked by existing screening strategies, leading to uneven allocation of screening resources and an increased risk of missed diagnoses. Establishing and promoting multi-factor-based individualized risk assessment models is an important direction for enhancing the effectiveness of GC screening, reducing the missed diagnosis rate, and achieving precise prevention. Future efforts should focus on further improving the external validation of risk models and promoting their application in clinical practice to achieve more precise and effective individualized GC screening.
In the process of GC screening and diagnosis, collaboration among multidisciplinary teams, including gastroenterology, pathology, and imaging, is crucial. However, in real clinical practice, there are often barriers to collaboration between these disciplines, leading to information silos and fragmented diagnostic and treatment processes. For example, if gastroenterologists fail to timely share the endoscopic images and preliminary diagnostic information obtained during screening with pathology and imaging experts, it can easily result in diagnostic delays or misjudgments, especially in low-risk populations where the risk of missed diagnoses is higher. In fact, early screening and precise classification of GC rely on comprehensive judgments from multiple disciplines; independent operations by a single discipline are difficult to meet the needs of complex cases [72].
The latest clinical guidelines for GC in South Korea emphasize that the collaboration of multidisciplinary teams, including surgical oncology, gastroenterology, endoscopy, medical oncology, abdominal radiology, pathology, nuclear medicine, radiation therapy, and guideline methodology experts, is fundamental to developing high-quality diagnostic and treatment recommendations. The update process of these guidelines involved repeated discussions and consensus-building through interdisciplinary groups, ensuring the scientific and systematic nature of screening, diagnosis, staging, and treatment at each stage. This demonstrates that the organic integration of multidisciplinary teams not only enhances the authority of the guidelines but also provides standardized and streamlined operational pathways for clinical practice [72]. In low-risk populations, the absence of such multidisciplinary cooperation significantly increases the risk of missed diagnoses due to incomplete diagnostic information and inconsistent judgment criteria.
Moreover, during the guideline formulation process, a systematic review and grading assessment were conducted for each recommendation, taking into account the level of evidence, benefits, risks, and clinical feasibility. The involvement of multidisciplinary teams makes the suggestions more clinically applicable and operational. Notably, the guideline structure specifically includes chapters on screening and diagnosis that cover endoscopy, pathology, imaging, and nuclear medicine, along with accompanying flowcharts to help clinicians quickly access multidisciplinary resources in their actual work, achieving efficient integration of information flow [72]. This model suggests that the optimization direction of the GC screening system in the future should place greater emphasis on building multidisciplinary diagnostic teams and promoting the normalization of interdisciplinary communication and collaboration mechanisms.
However, currently, some medical institutions in China have not yet established a comprehensive multidisciplinary collaboration platform in the application of GC screening scoring systems, leading to each discipline, such as gastroenterology, pathology, and imaging, operating independently, lacking regular consultation and case discussion mechanisms. This not only affects the scientific application of the screening scoring system but also limits the precise identification of difficult cases and the effective control of missed diagnosis risks. As clinical guidelines gradually shift towards a multidisciplinary collaboration model, promoting the construction of comprehensive diagnostic teams will become a key factor in improving the quality of GC screening and reducing the risk of missed diagnoses.
In summary, insufficient multidisciplinary collaboration has become an important factor affecting the sensitivity of the new GC screening scoring system in low-risk populations. In the future, efforts should be made to strengthen collaboration and information sharing among multidisciplinary teams, including gastroenterology, pathology, and imaging, and to improve comprehensive diagnostic processes, thereby effectively enhancing the capability to prevent and control missed diagnoses of GC in low-risk populations.
Artificial Intelligence (AI) and big data technologies are gradually becoming significant driving forces in the field of GC screening, demonstrating remarkable advantages in image recognition and risk prediction. AI relies on algorithms such as deep learning and convolutional neural networks to automatically identify early GC or precancerous lesions in medical images such as endoscopic and pathological slices, significantly enhancing the sensitivity and accuracy of screenings. For example, AI-assisted endoscopic image analysis systems generally achieve an accuracy rate exceeding 80% in early GC detection, with some systems showing sensitivity and accuracy superior to that of endoscopists [73,74]. Furthermore, AI can assist endoscopists in standardizing operations during real-time detection, reducing missed diagnoses and misjudgments, and it holds unique value in training beginners and standardizing operations [74]. In practical applications, AI systems can effectively detect GC lesions and point out low-quality images, enhancing diagnostic efficiency and accuracy [75]. As high-quality, large-scale medical image data accumulates, the training and iteration of AI models will become more precise, promoting the transition of GC screening from “experience-dependent” to a “data-driven” intelligent stage. It is noteworthy that the performance of AI in GC screening is limited by the diversity and quality of training data; thus, the convergence of big data from multiple centers, devices, and ethnicities, as well as algorithm optimization, will be key directions for enhancing the generalization capability of AI-assisted screening in the future [76].
In terms of risk prediction, big data-driven scoring systems provide new ideas for the refined management of low-risk populations. By integrating multi-source heterogeneous data such as electronic health records, molecular subtypes, imaging genomics, and genomics, AI demonstrates potential in multi-omics data analysis and precision medicine [77,78]. For instance, the clinical patient similarity network (cPSN) for GC, constructed based on big data analysis, utilizes unsupervised learning models to classify patients into subgroups; the clinical characteristics and prognoses of different subgroups vary significantly, aiding in the precise identification of high-risk individuals and optimizing follow-up strategies [77]. Additionally, AI-developed hierarchical screening models that integrate multimodal data (such as tongue image information and consultation data) exhibit higher accuracy and precision in predicting the risk of precancerous lesions compared to traditional methods [79]. Big data not only provide rich training resources for AI models but also lay the foundation for the continuous optimization and dynamic updating of scoring systems, enabling screening tools to adapt promptly to population characteristics and epidemiological changes.
The deep integration of AI and big data technologies is driving a transformation in GC screening models. From the integrated analysis of large-scale clinical data to the joint modeling of multimodal imaging and molecular data, AI-assisted scoring systems are expected to achieve more efficient and personalized screening decisions in low-risk populations. In the future, with ongoing advancements in data standardization, model interpretability, and multi-center validation, AI and big data will play increasingly central roles in GC screening, risk prediction, and precision prevention and control systems. This trend will provide solid technical support for reducing missed diagnosis risks in low-risk populations and enhancing screening efficacy.
In recent years, molecular subtype technology has made significant progress in GC research, particularly in revealing the heterogeneity of low-risk populations for GC. Single-cell sequencing technology allows for an in-depth analysis of the tumor immune microenvironment, uncovering the roles of different immune cell populations in tumor occurrence, progression, and resistance. For example, through the analysis of single-cell RNA sequencing data from metastatic GC, researchers found that tumor-associated neutrophils play a significant role in tumor heterogeneity and prognosis assessment. Based on neutrophil-related genes, GC can be divided into two molecular subtypes with different immune microenvironment characteristics. Researchers established a six-gene prognostic risk model that exhibited stable predictive capabilities in both internal and external cohorts [29]. This indicates that molecular subtypes can not only reveal biological differences within low-risk GC patient groups but also provide a theoretical basis for further refining screening targets.
The construction of precise screening strategies relies on the effective integration of molecular subtype results. By combining tumor molecular characteristics, gene expression profiles, and clinical phenotypes, researchers can formulate more personalized screening plans. For instance, utilizing molecular subtypes and risk models can identify low-risk patients who are more likely to respond favorably to immunotherapy, thereby optimizing resource allocation and reducing excessive screening. Recent studies have also screened small-molecule drugs targeting key prognostic genes through molecular docking methods, providing new directions for precision prevention and intervention [29]. In practical applications, molecular subtype results can assist doctors in determining which low-risk populations belong to an “insidious high-risk” subtype, indicating that they may require more frequent or in-depth follow-ups.
Moreover, with the application of cutting-edge technologies such as next-generation sequencing and organoids, the molecular subtypes of GC are becoming increasingly refined. Patient-derived organoids and xenograft models provide powerful tools for gene evolution, drug screening, and personalized medicine research. These models not only help identify new biomarkers but also facilitate prospective drug screening and efficacy prediction, thus promoting the iterative upgrading of precision screening strategies [80]. By integrating molecular subtypes, clinical characteristics, and drug response information, dynamic risk assessment and personalized screening for low-risk populations are expected to be realized in the future.
The concept of precision medicine has gradually permeated all aspects of GC screening and prevention. The clinical application of immune checkpoint inhibitors and targeted therapies, such as BRAF and HER2, has propelled the deep integration of molecular subtypes with precision treatment. An increasing number of clinical trials are exploring combination treatment strategies guided by molecular subtypes in hopes of improving patient survival rates while reducing treatment side effects [80]. As molecular subtype technology becomes more widespread and costs decrease, precision screening is expected to become an important means of preventing and controlling GC in low-risk populations.
In summary, molecular subtype technology provides a scientific basis for screening low-risk GC populations, and the continuous improvement of precision medicine strategies will further enhance the sensitivity and specificity of screenings, providing a solid guarantee for reducing missed diagnosis risks and achieving personalized prevention and control.
In recent years, the field of GC screening has gradually emphasized the combined application of multimodal screening technologies, integrating various methods such as endoscopy, imaging examinations, and molecular marker detection. Traditional GC screening methods primarily rely on endoscopy, which has a high detection rate for early lesions. However, issues such as its invasive nature, low patient compliance, and high costs limit its widespread adoption among low-risk populations. Imaging examinations such as ultrasound, CT, and MRI can serve as auxiliary tools in GC screening, particularly valuable for assessing gastric wall structure and determining tumor staging. However, the sensitivity of a single imaging modality for early GC or small lesions is limited, making it difficult to independently undertake screening tasks [81].
Molecular marker detection, especially novel molecular markers such as circulating tumor DNA, DNA methylation, and non-coding RNA in the blood, has shown high sensitivity and specificity in recent years for early GC screening. Relevant studies indicate that ctDNA and its methylation status can reflect the genetic and epigenetic characteristics of tumors, providing possibilities for non-invasive detection [45,47,79]. Additionally, techniques such as breath analysis, serum proteomics, and metabolomics are being gradually integrated into the screening system to enhance the capability of identifying early lesions [82,83,84].
The multimodal screening model emphasizes the organic integration of various methods such as endoscopy, imaging, and molecular markers. For example, artificial intelligence-assisted multimodal screening models can integrate tongue diagnosis and inquiry information to achieve stratified prediction of GC and precancerous lesions, providing personalized recommendations for endoscopy [79]. Related studies show that multimodal artificial intelligence models have an AUC of up to 0.74–0.82 in screening for precancerous lesions, significantly outperforming single modalities, and demonstrating stable performance in external validation cohorts. This model not only improves screening accuracy but also optimizes endoscopic resource allocation, alleviating the examination burden on low-risk populations. Notably, the combination of AI and multi-omics data is expected to further enhance screening sensitivity and specificity, bridging the gap of traditional methods in detecting early lesions [85,86].
The comprehensive application of multimodal screening positively impacts the reduction of missed diagnosis rates. Multiple studies have shown that molecular marker detection plays a significant role in the diagnosis, prognosis, and treatment guidance of GC [87,88]. Furthermore, the introduction of new technologies such as liquid biopsy and AI-assisted analysis has made multimodal screening not only more convenient and acceptable but also provides an economically viable solution for large-scale population screening. As the multimodal screening system continues to improve, its application among low-risk populations is expected to become a key direction for future early GC screening.
Overall, multimodal screening technology, through the integration of multidimensional information from endoscopy, imaging, and molecular markers, can significantly enhance the sensitivity and specificity of early GC screening and reduce the risk of missed diagnoses in low-risk populations. In the future, with the further development of artificial intelligence and multi-omics technologies, the multimodal screening system is expected to achieve more precise and individualized risk stratification and screening strategies, providing a solid foundation for the early detection and intervention of GC. Building upon this concept of multimodal integration, we propose a future paradigm for precision screening driven by artificial intelligence, as illustrated in Figure 3. This framework aims to achieve dynamic and individualized risk stratification, optimize the allocation of screening resources, and systematically reduce the risk of missed diagnoses.
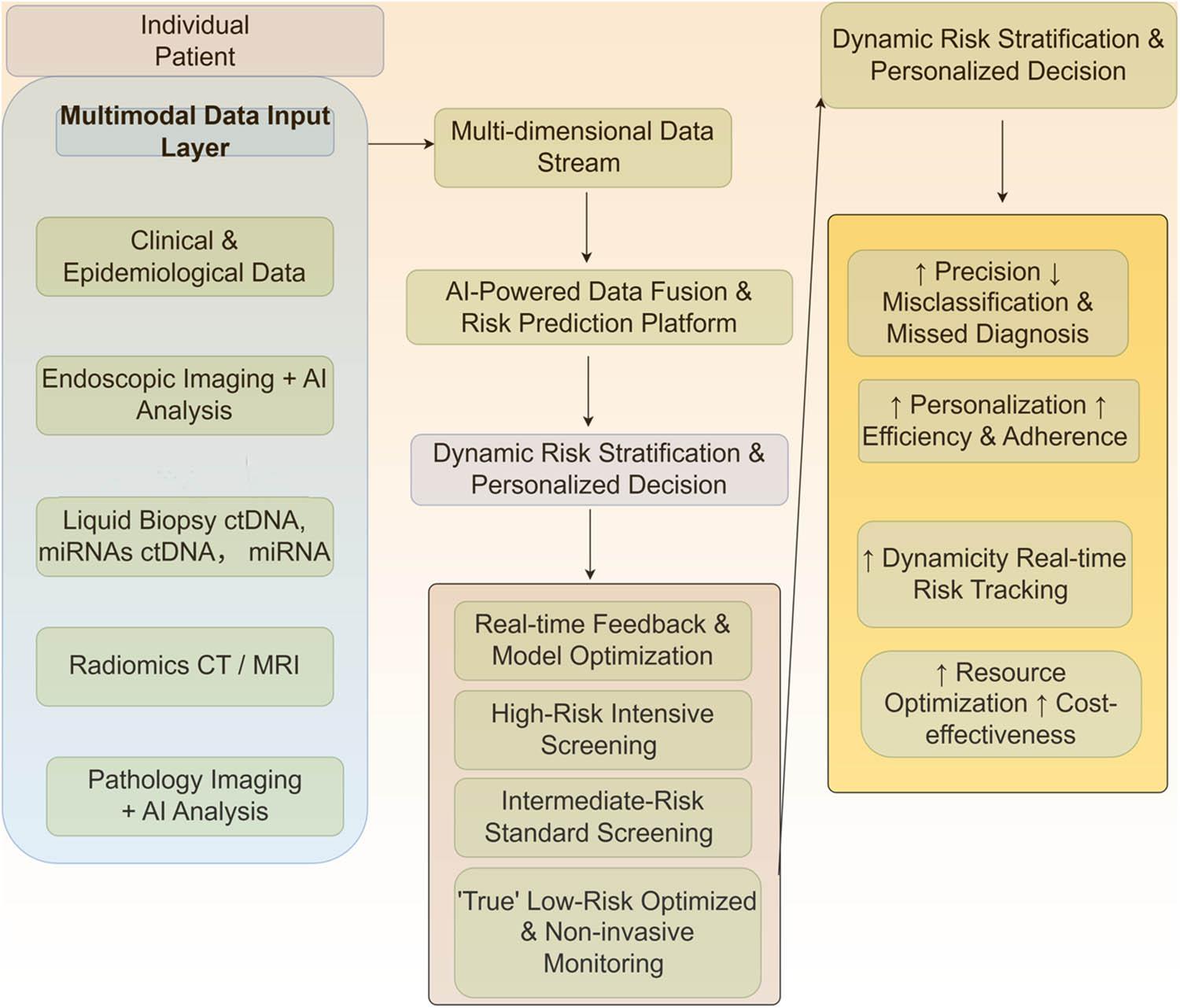
A paradigm for precision gastric cancer screening integrating multimodal data and artificial intelligence. Schematic illustration of a proposed future paradigm for precision gastric cancer screening, leveraging multimodal data integration and AI. This framework involves the comprehensive collection of multidimensional data, including clinical and epidemiological information, endoscopic imaging with AI-assisted analysis, liquid biopsy (e.g., ctDNA, miRNAs), radiomics from CT/MRI, and pathological imaging with AI diagnostics. These data streams are fused and analyzed by an AI-powered platform to generate a dynamic and individualized risk stratification. This enables personalized screening decisions: individuals at high risk are directed to intensive screening protocols, those at intermediate risk receive standard screening, and those confirmed as “true” low-risk through multimodal validation are assigned to optimized, non-invasive monitoring strategies. This closed-loop, intelligent system facilitates real-time feedback and model refinement, aiming to enhance screening precision and efficiency, optimize healthcare resource allocation, and systematically reduce the risk of missed diagnoses
Regarding the issue of missed diagnoses in the new GC screening scoring system among low-risk populations, it is evident from various current research findings that the fundamental reason lies in the interplay of multiple factors. As a seasoned review expert in the medical field, I believe that a deep understanding and balance of different research perspectives are essential for advancing scientific progress and clinical application in this area.
Firstly, deficiencies in the design of the scoring system are the core factors leading to missed diagnoses. Most existing scoring systems are primarily developed based on clinical characteristics and biomarkers of high-risk populations, making it difficult to adequately cover the hidden and diverse pathological molecular characteristics in low-risk populations. Some studies emphasize the specific molecular subtypes and pathological manifestations of GC in low-risk populations, such as the micro-lesions and molecular heterogeneity of early GC, which exceed the detection scope of traditional scoring systems, resulting in inaccurate risk assessments. Therefore, future optimizations of the scoring system must more deeply incorporate new molecular and pathological indicators from low-risk populations to achieve refined and personalized risk identification.
Second, differences in technical levels and experience in clinical operations significantly impact the missed diagnosis rate as well. Some studies point out that the standardization of endoscopic techniques and procedures is inadequate, and the uneven training of medical personnel makes it difficult to detect early lesions in a timely manner. In this regard, it is necessary to strengthen the formulation and promotion of operational standards, enhance the professional skills of healthcare personnel, especially in applying high-sensitivity detection techniques in low-risk population screenings, thereby reducing the occurrence of human errors.
Moreover, the inadequacies of the screening strategies themselves also reveal limitations. Currently, there is a heavy reliance on single indicators or simple scoring, lacking multidimensional and multimodal comprehensive assessment methods. With the development of artificial intelligence, big data, and molecular typing technologies, multidisciplinary collaboration and integration of various technologies have become trends. Many studies support the construction of more comprehensive screening models by integrating clinical data, imaging features, biomarkers, and genomic information. This not only aids in accurately identifying high-risk individuals within low-risk populations but also enables personalized screening plans, improving screening efficiency and accuracy.
Based on the above analysis, future development directions should focus on the following aspects: first, improving the research on the molecular pathological characteristics of GC in low-risk populations to enrich the screening indicator system; second, promoting the standardization of clinical operations and professional training for healthcare personnel to reduce errors caused by technical differences; third, constructing an intelligent screening platform based on multimodal data fusion to achieve dynamic follow-up and risk assessment; fourth, facilitating multidisciplinary collaboration to integrate resources from gastroenterology, pathology, molecular biology, and data science, forming a closed-loop management system.
In summary, the issue of missed diagnoses in the new GC screening scoring system among low-risk populations is a complex and multilayered challenge that involves not only technical shortcomings but also the standardization of clinical practices and strategic innovations. As experts, we should approach existing research findings with a scientifically rigorous attitude, balancing the merits and drawbacks of different viewpoints, promoting interdisciplinary integration and technological innovation, and ultimately achieving early, precise screening and effective intervention for GC in low-risk populations, thereby significantly reducing the overall incidence and mortality rates of GC and improving public health levels.
Basang Zhuoma, Pengfei Shao, and Wei Li designed the study and checked the literature; Pengfei Shao and Yurong Xie did manuscript preparation and wrote the manuscript. Yibi Ranhen and CiYang prepared and edited the manuscript. All the authors read through the whole manuscript.
Pengfei Shao https://orcid.org/0009-0000-0001-5534-1206
Yurong Xie https://orcid.org/0009-0009-4400-7937
Yibi Ranhen https://orcid.org/000-0003-2119-3297
Ci Yang https://orcid.org/0009-0006-1888-2533
Basang Zhuoma https://orcid.org/0009-0003-3339-2258
This work was supported by the National Key Clinical Specialty Construction Project (Department of Gastroenterology (Lhasa People’s Hospital) and Medical Aid‑Xizang Project (XZ2002ZR-ZY18(Z)).
The authors have no potential conflicts of interest to declare.