
Chronic periapical periodontitis, a common disease in dental field, often emerges and develops due to untimely treatment of acute pulpitis, which in turn triggers chronic inflammation of periapical tissues [1]. If left untreated, the condition may lead to pain, impaired oral function, and even irreversible structural damage to the affected teeth, significantly affecting patients’ quality of life. Therefore, it is of important significance to carry out in-depth study on the treatment and outcome of chronic periapical periodontitis.
As the preferred therapeutic method for chronic periapical periodontitis at present, root canal treatment focuses on the complete removal of infectious substances from root canals via mechanical and chemical means, thereby facilitating the healing as well as the repair of periapical tissues [2]. However, treatment success in root canal therapy and the changes in periapical radiograph signs after treatment are directly related to the prognosis of patients [3]. As medical imaging techniques have advanced rapidly in recent years, radiographs now play a progressively more significant role in diagnosing oral diseases and monitoring their treatment. In cases of chronic periapical periodontitis, pre- and post-treatment periapical radiographs provide a direct visual indication of lesions in periapical tissues, such as decrease of transmission area and clarification of boundaries, providing a crucial basis for evaluating the treatment effect and prognosis [4,5].
However, despite the clinical relevance of radiographic evaluation, existing studies have mainly focused on long-term healing rates or general prognostic factors, while the value of early radiographic changes as quantitative predictors of treatment outcome has been insufficiently explored [6,7]. Moreover, few studies have incorporated early radiographic measurements into predictive models, leaving a gap in the development of practical tools for early risk assessment [8]. Given the clinical need for timely identification of patients at risk for delayed healing or treatment failure, research addressing early radiographic predictors is both necessary and clinically valuable.
This study aimed to evaluate the changes in periapical radiograph signs before and after root canal treatment in patients suffering from chronic periapical periodontitis and to explore the relationship between these radiographic changes and treatment prognosis. It is expected to further reveal the specific mechanism of root canal treatment for chronic periapical periodontitis, optimize the treatment scheme, elevate the success rate of treatment, and offer clinicians strong support in judging prognosis and formulating individualized treatment plans. Meanwhile, this study will provide new ideas and directions for the basic research and clinical treatment of chronic periapical periodontitis.
This study was designed as a retrospective observational cohort study. All data were obtained from the electronic medical record system and imaging database of our hospital.
This study got approval from the ethics committee of our hospital (No. JN. No20210432c0040912[113]). A total of 100 patients (100 teeth in total) diagnosed with chronic periapical periodontitis and received root canal-based management between June 2021 and June 2023 were screened. Patients were consecutively enrolled according to the predefined criteria to minimize selection bias. During the study period, all eligible patients who met the criteria and completed a minimum 12-month radiographic follow-up were included.
Inclusion criteria included: (1) patients diagnosed with chronic periapical periodontitis according to the criteria in cariology and endodontology and confirmed by radiography [9], (2) those with definite clinical indications for root canal treatment, (3) those whose diseased teeth had fully developed root, (4) those receiving root canal-based management for the first time at our hospital, and (5) those with complete clinical data and radiographic records with ≥12-month follow-up.
The following exclusion criteria were executed: (1) patients with suspected vertical carnassial teeth, (2) those with combined periodontic–endodontic lesions, (3) those with the bending root of the diseased teeth, (4) those with severe periodontal tissue lesions, or (5) those with systemic conditions known to significantly impair wound healing, including uncontrolled diabetes mellitus, autoimmune diseases (such as systemic lupus erythematosus, rheumatoid arthritis), and hematological disorders (such as severe anemia, leukemias). Conversely, patients with medically controlled chronic conditions (such as well-controlled type 2 diabetes or hypertension) were not excluded because such conditions do not substantially affect periapical healing under effective management.
Patients received microscopic root canal treatment under standardized protocols. Specifically, periapical radiographs were obtained before treatment to fully understand the extent of periapical lesions, anatomical morphology of root, and other conditions of the diseased teeth. Rubber dams were used to insulate the diseased teeth from moisture, the pulp cavity was routinely prepared, and the root canals were probed and unblocked. Next, the pulp cavity was soaked and rinsed in 3% sodium hypochlorite (Chengdu Kelong Chemical Reagent Co., Ltd., China), and the root canals were ultrasonically vibrated, dried, and sealed with drugs. After that, the tooth apexes were filled with warm gutta-percha through vertical compression, and the crowns were filled with resin (Filtek™ Z350 XT, 3 M ESPE, USA) or inlays (Lava™ Ultimate, 3 M ESPE, USA). Postoperatively, radiographs were taken.
A medical diagnostic X-ray apparatus (X-ray system: KaVo FOCUS™, KaVo Dental GmbH, Biberach, Germany) was employed to capture the periapical radiographs, with the voltage, current, and exposure time set at 60 kV, 7 mA, and 0.2 s, respectively. In brief, a digital imaging plate (PSP plate, Dürr Dental AG, Bietigheim-Bissingen, Germany) was fixed at 20 cm in front of the X-ray tube for photography. Moreover, the periapical radiograph signs of the patients were recorded before treatment and at 3, 6, and 12 months following treatment, including the maximum horizontal diameter (X) and maximum vertical diameter (Y) of periapical shadows, together with the maximum horizontal length (L) and maximum vertical height (H) of alveolar bone resorption.
(1) General data: The gender, age, body mass index, course of disease, jaw position (upper jaw or lower jaw), and tooth position (anterior tooth, premolar, or molar) of the patients were recorded. (2) Periodontal indexes: Patients' plaque index and gingival index were evaluated before treatment. Plaque index was scored 0–4 points according to the thickness of dental plaques, and higher scores indicated thicker dental plaques [10]. Gingival index was scored from 0 to 4 points based on the severity of gingival inflammation, with higher scores signifying more serious gingival inflammation [11]. (3) Treatment-related indicators: The number of root canals (single, double, or multiple), coronal restoration materials (resin or inlay), root canal filling time, root filling status (≤2 mm, >2 mm, or overfilling), repair status (non-repair, post repair, porcelain crown, or composite crown), presence or absence of coronal microleakage, secondary caries, instrument fracture, and retreatment were investigated. Instrument fracture was defined as the presence of a fractured endodontic instrument fragment that remained inside the canal and could not be removed during treatment, and was therefore left in situ. Retreatment refers to a second root canal procedure performed during the 3-, 6-, or 12-month follow-up period for cases showing persistent periapical inflammation or insufficient radiographic improvement, and therefore represents a postoperative intervention. (4) Indicators for periapical radiograph signs: The periapical index (PAI) before treatment was examined, in addition to periapical radiograph signs X, Y, L, and H before treatment and at 3, 6, 12 months after treatment.
After treatment, the patients were followed up through outpatient visits for totally 12 months until June 2024, and the healing of tooth apexes was recorded within 12 months after treatment. The criteria for determining the healing of tooth apexes were as follows [12]: (1) absence of clinical symptoms, including no pain, swelling, sinus tract, or tooth mobility, with restoration of normal function; (2) radiographic evidence of periapical repair, defined as a clear reduction in the size or density of the periapical radiolucency and reformation of normal trabecular structure. A periapical shadow that showed no detectable change in size or radiodensity during the 12-month follow-up was classified as nonhealing, as it did not meet the criterion of radiographic improvement. Patients who met the aforementioned criteria were included in a healed group (n = 74), and the remaining patients, including those with unchanged or enlarged radiolucencies, were allocated to an unhealed group (n = 26).
SPSS 22.0 software was applied for the processing of statistical analysis. The normality of continuous variables was assessed using the Shapiro–Wilk test. Normally distributed continuous data were presented as mean ± standard deviation (x ± s). Between-group comparisons were implemented via independent-samples t-test, and comparisons across multiple time points within groups were carried out via repeated-measures analysis of variance. Count data were expressed by rates (%) and compared between groups through χ 2 test or Fisher's exact test. The factors contributing to nonhealing of tooth apexes in patients suffering from chronic periapical periodontitis after root canal-based management were analyzed by a multivariate logistic regression model. In addition, multicollinearity test was adopted to determine the presence or the absence of collinearity among diverse influencing factors, with tolerance >0.1 and variance inflation factors <10, indicating no collinearity among these factors. The model was re-sampled 1,000 times via the Bootstrap method for internal validation, and assessed by Nagelkerke R 2 for its goodness of fit. The threshold of significance was determined as α = 0.05.
According to the periapical radiograph signs of 100 patients with chronic periapical periodontitis, X was 2.67 ± 0.78 mm, 1.39 ± 0.45 mm, 0.98 ± 0.39 mm, and 0.45 ± 0.18 mm; Y was 1.68 ± 0.56 mm, 1.34 ± 0.42 mm, 0.84 ± 0.31 mm, and 0.27 ± 0.12 mm; L was 0.71 ± 0.20 mm, 0.48 ± 0.21 mm, 0.25 ± 0.13 mm, and (0.07 ± 0.02) mm; and H was 2.35 ± 0.70 mm, 1.80 ± 0.64 mm, 0.69 ± 0.32 mm, and 0.06 ± 0.03 mm before treatment and at 3, 6, and 12 months after root canal treatment, respectively. At 3, 6, and 12 months after treatment, X, Y, L, and H were significantly reduced in sequence by comparison to those before treatment, with statistically significant differences (p < 0.05).
Through comparing patients' clinical data between the two groups, it was discovered that the proportions of patients with coronal restoration materials of inlay, coronal microleakage, and instrument fracture were distinctly elevated, while those of root filling ≤2 mm and retreatment during follow-up were conspicuously diminished in the unhealed group relative to the healed group (p < 0.05). However, no statistically significant differences could be inspected in the rest indicators between the two groups (p > 0.05) (Table 1).
Clinical data of the two groups of patients
| Group | Healed (n = 74) | Unhealed (n = 26) | t/χ 2 | p |
|---|---|---|---|---|
| Gender, n (%) | 0.041 | 0.84 | ||
| Male | 41 (55.41) | 15 (57.69) | ||
| Female | 33 (44.59) | 11 (42.31) | ||
| Age (year) | 42.58 ± 6.82 | 43.02 ± 7.11 | 0.28 | 0.78 |
| Body mass index (kg/m2) | 22.86 ± 2.02 | 23.18 ± 1.14 | 0.764 | 0.446 |
| Course of disease (month) | 5.62 ± 1.13 | 5.81 ± 1.22 | 0.722 | 0.472 |
| Jaw position, n (%) | 0.094 | 0.76 | ||
| Upper jaw | 43 (58.11) | 16 (61.54) | ||
| Lower jaw | 31 (41.89) | 10 (38.46) | ||
| Tooth position, n (%) | 1.385 | 0.5 | ||
| Anterior tooth | 27 (36.49) | 8 (30.77) | ||
| Premolar | 25 (33.78) | 7 (26.92) | ||
| Molar | 22 (29.73) | 11 (42.31) | ||
| PAI grade, n (%) | 4.168 | 0.124 | ||
| Grade 3 | 22 (29.73) | 5 (19.23) | ||
| Grade 4 | 38 (51.35) | 11 (42.31) | ||
| Grade 5 | 14 (18.92) | 10 (38.46) | ||
| Plaque index (point) | 1.65 ± 0.48 | 1.81 ± 0.55 | 1.407 | 0.163 |
| Gingival index (point) | 2.24 ± 0.79 | 2.41 ± 0.86 | 0.922 | 0.359 |
| Number of root canals, n (%) | 3.015 | 0.221 | ||
| Single | 28 (37.84) | 5 (19.23) | ||
| Double | 20 (27.03) | 9 (34.62) | ||
| Multiple | 26 (35.14) | 12 (46.15) | ||
| Coronal restoration materials, n (%) | 4.582 | 0.032 | ||
| Resin | 49 (66.22) | 11 (42.31) | ||
| Inlay | 25 (33.78) | 15 (57.69) | ||
| Root canal filling time (s) | 81.42 ± 13.56 | 82.78 ± 12.95 | 0.445 | 0.657 |
| Root canal filling status, n (%) | 0.001a | |||
| ≤2 mm | 65 (87.84) | 15 (57.69) | ||
| >2 mm | 8 (10.81) | 7 (26.92) | ||
| Overfilling | 1 (1.35) | 4 (15.38) | ||
| Repair status, n (%) | 0.434a | |||
| Nonrepair | 16 (21.62) | 8 (30.77) | ||
| Postrepair | 23 (31.08) | 4 (15.38) | ||
| Porcelain crown | 17 (22.97) | 6 (23.08) | ||
| Composite crown | 18 (24.32) | 8 (30.77) | ||
| Coronal microleakage, n (%) | 9.591 | 0.002 | ||
| No | 46 (62.16) | 7 (26.92) | ||
| Yes | 28 (37.84) | 19 (73.08) | ||
| Secondary caries, n (%) | 1.206 | 0.272 | ||
| No | 66 (89.19) | 21 (80.77) | ||
| Yes | 8 (10.81) | 5 (19.23) | ||
| Instrument fracture, n (%) | 10.534 | 0.001 | ||
| No | 59 (79.73) | 12 (46.15) | ||
| Yes | 15 (20.27) | 14 (53.85) | ||
| Retreatment during follow-up, n (%) | 4.476 | 0.034 | ||
| No | 46 (62.16) | 9 (34.62) | ||
| Yes | 28 (37.84) | 15 (57.69) |
“Retreatment during follow-up” refers to a second root canal procedure performed during the 3-, 6-, or 12-month follow-up period in cases showing persistent periapical pathology. It is a postoperative intervention.
aFisher’s exact text.
The apical radiographic signs in both two groups of patients before and after treatment were compared. The results manifested that X, Y, L, and H in the two groups were not statistically significantly different before treatment (p > 0.05). At 3, 6, and 12 months after treatment, the indicators for periapical radiograph signs in the two groups were markedly reduced in sequence relative to those before treatment, and the reductions were significantly greater in the healed group in contrast with the unhealed group (p < 0.05) (Table 2).
Periapical radiograph signs before and after treatment (x ± s, mm)
| Group | n | X | |||
|---|---|---|---|---|---|
| Before treatment | 3 months after treatment | 6 months after treatment | 12 months after treatment | ||
| Healed | 74 | 2.65 ± 0.74 | 1.31 ± 0.41* | 0.89 ± 0.33*# | 0.37 ± 0.11*#△ |
| Unhealed | 26 | 2.72 ± 0.81 | 1.62 ± 0.49* | 1.24 ± 0.42*# | 0.66 ± 0.24*#△ |
| t | 0.405 | 3.149 | 4.323 | 8.262 | |
| P | 0.686 | 0.002 | <0.001 | <0.001 | |
| Group | n | Y | |||
|---|---|---|---|---|---|
| Before treatment | 3 months after treatment | 6 months after treatment | 12 months after treatment | ||
| Healed | 74 | 1.66 ± 0.51 | 1.26 ± 0.39* | 0.76 ± 0.25*# | 0.21 ± 0.08*#△ |
| Unhealed | 26 | 1.75 ± 0.58 | 1.58 ± 0.47* | 1.08 ± 0.36*# | 0.45 ± 0.16*#△ |
| t | 0.747 | 3.408 | 4.974 | 9.904 | |
| P | 0.457 | 0.001 | <0.001 | <0.001 | |
| Group | n | L | |||
|---|---|---|---|---|---|
| Before treatment | 3 months after treatment | 6 months after treatment | 12 months after treatment | ||
| Healed | 74 | 0.69 ± 0.21 | 0.44 ± 0.19* | 0.21 ± 0.15*# | 0.05 ± 0.02*#△ |
| Unhealed | 26 | 0.75 ± 0.18 | 0.58 ± 0.20* | 0.37 ± 0.12*# | 0.11 ± 0.03*#△ |
| t | 1.298 | 3.188 | 4.91 | 11.458 | |
| P | 0.197 | 0.002 | <0.001 | <0.001 | |
| Group | n | H | |||
|---|---|---|---|---|---|
| Before treatment | 3 months after treatment | 6 months after treatment | 12 months after treatment | ||
| Healed | 74 | 2.31 ± 0.69 | 1.72 ± 0.60* | 0.63 ± 0.26*# | 0.05 ± 0.02*#△ |
| Unhealed | 26 | 2.47 ± 0.72 | 2.01 ± 0.67* | 0.85 ± 0.39*# | 0.10 ± 0.04*#△ |
| t | 1.006 | 2.056 | 3.232 | 8.253 | |
| P | 0.317 | 0.042 | 0.002 | <0.001 | |
*p < 0.05 vs before treatment, # p < 0.05 vs at 3 months after treatment, and Δ p < 0.05 vs at 6 months after treatment.
Considering the timeliness, cost-effectiveness, prediction accuracy, and data stability of early indicators, the indicators for periapical radiograph signs manifesting statistically significant differences between the healed and unhealed groups at 3 months after treatment and the indicators with between-group differences of statistical significance in Table 1 were regarded as independent variables, and the healing status of tooth apexes (healing =0, non-healing =1) at 12 months after treatment was set as a dependent variable. A multivariate logistic regression model was then constructed to identify independent predictors of nonhealing. The results depicted that the use of inlay as the coronal restoration material, root filling >2 mm and overfilling, coronal microleakage, instrument fracture, and increases in X, Y, L, and H at 3 months after treatment emerged as risk factors for nonhealing of tooth apexes in patients with chronic periapical periodontitis at 12 months after root canal treatment. In contrast, retreatment during follow-up was identified as a protective factor (p < 0.05) (Table 3).
Factors contributing to non-healing of tooth apexes in patients analyzed using multivariate logistic regression model
| Indicator | β | SE | Wald χ 2 | p | OR (95%CI) |
|---|---|---|---|---|---|
| Coronal restoration materials | |||||
| Resin (reference) | 1 | ||||
| Inlay | 1.123 | 0.536 | 4.387 | 0.011 | 3.074 (1.075–8.790) |
| Root filling status | <0.001 | ||||
| ≤2 mm (reference) | 1 | ||||
| >2 mm | 1.328 | 0.472 | 7.911 | <0.001 | 3.773 (1.496–9.517) |
| Overfilling | 1.363 | 0.501 | 7.396 | <0.001 | 3.908 (1.464–10.433) |
| Coronal microleakage | |||||
| No (reference) | 1 | ||||
| Yes | 1.437 | 0.425 | 11.425 | <0.001 | 4.208 (1.829–9.679) |
| Instrument fracture | |||||
| No (reference) | 1 | ||||
| Yes | 0.936 | 0.611 | 2.345 | 0.032 | 2.550 (0.770–8.445) |
| Retreatment | |||||
| No (reference) | 1 | ||||
| Yes | −0.875 | 0.624 | 1.965 | 0.039 | 0.417 (0.123–1.416) |
| X at 3 months after treatment | 1.048 | 0.563 | 3.465 | 0.017 | 2.852 (0.946–8.598) |
| Y at 3 months after treatment | 1.266 | 0.528 | 5.747 | 0.002 | 3.547 (1.260–9.983) |
| Lat 3 months after treatment | 0.97 | 0.582 | 2.778 | 0.025 | 2.638 (0.843–8.254) |
| Hat 3 months after treatment | 0.685 | 0.657 | 1.086 | 0.046 | 1.984 (0.547–7.190) |
Multicollinearity test was conducted on the factors contributing to nonhealing of tooth apexes in patients at 12 months after root canal treatment obtained from analysis with the multivariate logistic regression model. It was demonstrated that the tolerance of each factor was >0.2, the variance inflation factor was <5, and no multicollinearity was detected among the nine indicators, suggesting that they are fairly stable as the independent variables for model establishment (Table 4).
Multicollinearity test results
| Indicator | Tolerance | Variance inflation factor |
|---|---|---|
| Coronal restoration materials | 0.216 | 4.63 |
| Root filling status | 0.384 | 2.604 |
| Coronal microleakage | 0.275 | 3.636 |
| Instrument fracture | 0.421 | 2.375 |
| Retreatment | 0.506 | 1.976 |
| X at 3 months after treatment | 0.372 | 2.688 |
| Y at 3 months after treatment | 0.481 | 2.079 |
| L at 3 months after treatment | 0.515 | 1.942 |
| H at 3 months after treatment | 0.602 | 1.661 |
Restricted cubic spline was employed to analyze the relationship between periapical radiograph signs and nonhealing risk of tooth apexes in patients at three months after root canal treatment. It was uncovered that the nonhealing risk of tooth apexes climbed with the increases in X, Y, L, and H, and X > 1.48 mm (A), Y > 1.42 mm (B), L > 0.52 mm (C), and H > 1.95 mm (D) were positively correlated with the nonhealing risk of tooth apexes (p < 0.05) (Figure 1).
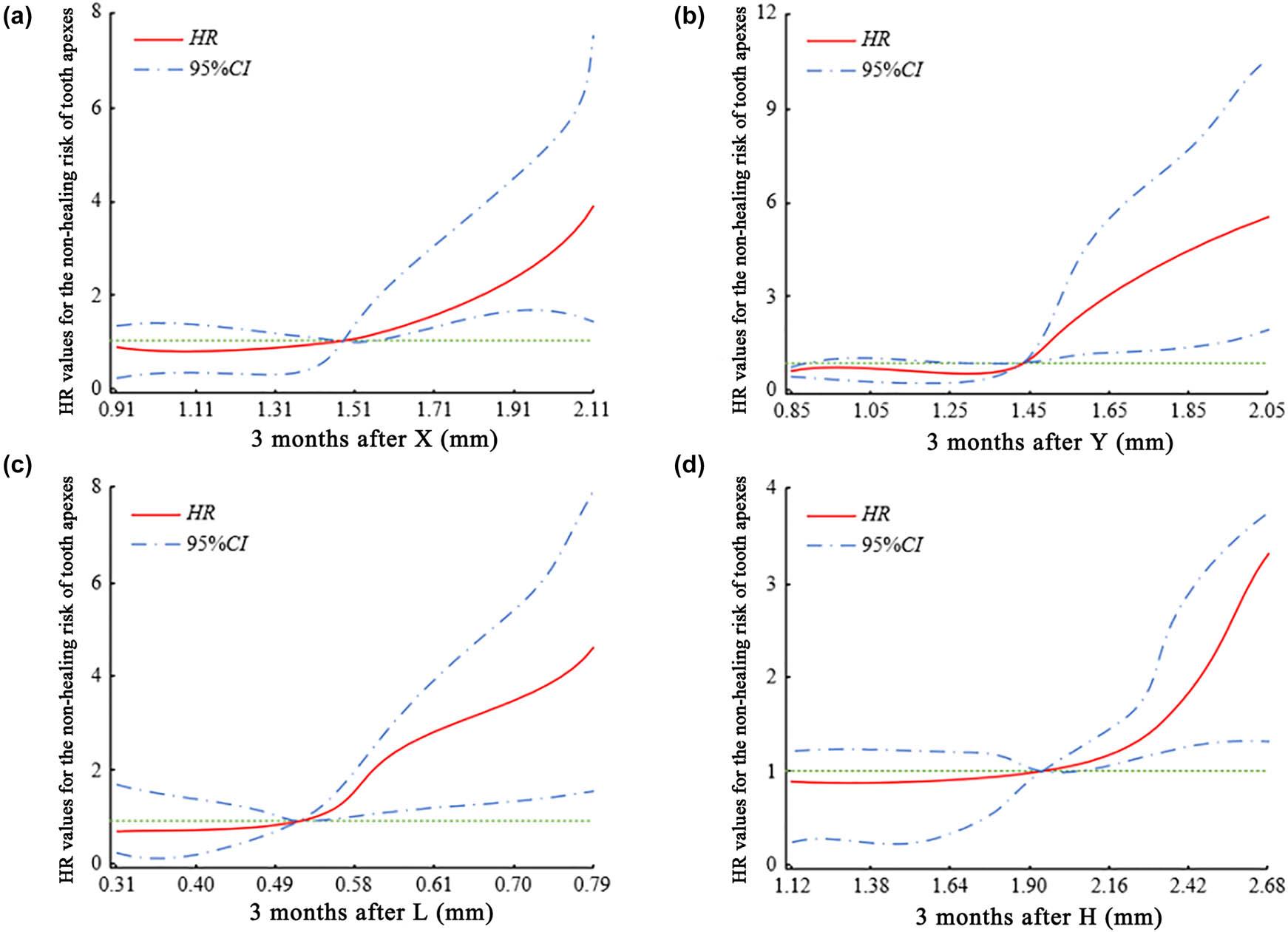
Dose–response relationship between periapical radiograph signs and non-healing risk of tooth apexes at 3 months after root canal treatment analyzed by restricted cubic spline. The red solid line represents the adjusted hazard ratio (HR), and the blue dashed lines indicate the corresponding 95% confidence intervals (95% CI). The green dotted horizontal line denotes HR = 1 as the reference level. Radiographic variables include the (a) maximum horizontal diameter (X), (b) vertical diameter (Y), (c) horizontal length of alveolar bone resorption (L), and (d) vertical height of alveolar bone resorption (H)
The multivariate logistic regression model was constructed by using the independent variables significantly associated with non-healing of tooth apexes after root canal treatment. The final predictive equation for the probability of nonhealing at 12 months was as follows: p = 1/(1 + e-Z ), where Z = 3.754–1.123 × inlay restoration (no = 0, yes = 1) −1.328 × root filling >2 mm/1.363 × overfilling (no = 0, yes = 1) −1.437 × coronal microleakage (no = 0, yes = 1) −0.936 × instrument fracture (no = 0, yes = 1) + 0.875 × retreatment (no = 0, yes = 1) −1.048 × X at 3 months −1.266 × Y at 3 months −0.970 × L at 3 months −0.685 × H at 3 months. Using p = 0.85 as the optimal cutoff value, the model achieved a maximum Youden index was 0.734, with a prediction accuracy of 87.3%, sensitivity of 85.9%, and specificity of 88.4% (Table 5). Internal validation using the bootstrap method (1,000 resamples) demonstrated high consistency between prevalidation and postvalidation performance metrics. In addition, the model showed good goodness of fit, with Nagelkerke R 2 = 0.601, indicating acceptable stability and explanatory power (Table 6). The discriminative ability of the model was assessed using the receiver operating characteristic (ROC) curve. The logistic regression model demonstrated excellent performance, yielding an area under the ROC curve of 0.892 (Figure 2). This finding is consistent with the high sensitivity and specificity observed at the optimal probability threshold (0.85), further supporting the strong predictive capability of the model.
Performance of prediction model at different probability levels on non-healing of tooth apexes after root canal treatment
| Probability | Accuracy (%) | Sensitivity (%) | Specificity (%) | False positive rate (%) | False negative rate (%) | Youden index |
|---|---|---|---|---|---|---|
| 0.95 | 78.1 | 90.0 | 75.7 | 24.3 | 10.0 | 0.657 |
| 0.9 | 84.5 | 88.5 | 83.8 | 16.2 | 11.5 | 0.723 |
| 0.85 | 87.3 | 85.9 | 88.4 | 11.6 | 14.1 | 0.734 |
| 0.8 | 88.9 | 81.5 | 91.2 | 8.8 | 18.5 | 0.727 |
| 0.75 | 90.0 | 78.1 | 93.2 | 6.8 | 21.9 | 0.714 |
| 0.7 | 90.4 | 76.9 | 94.0 | 6.0 | 23.1 | 0.709 |
| 0.65 | 90.6 | 75.0 | 94.9 | 5.1 | 25.0 | 0.700 |
| 0.6 | 90.1 | 72.0 | 95.3 | 4.7 | 28.0 | 0.673 |
| 0.55 | 90.5 | 69.2 | 96.0 | 4.0 | 30.8 | 0.653 |
| 0.5 | 90.0 | 65.4 | 96.6 | 3.4 | 34.6 | 0.620 |
| 0.45 | 89.7 | 62.5 | 96.8 | 3.2 | 37.5 | 0.593 |
| 0.4 | 89.0 | 60.0 | 97.0 | 3.0 | 40.0 | 0.570 |
| 0.35 | 88.5 | 57.7 | 97.3 | 2.7 | 42.3 | 0.550 |
| 0.3 | 87.8 | 55.0 | 97.5 | 2.5 | 45.0 | 0.525 |
| 0.25 | 87.0 | 52.0 | 97.8 | 2.2 | 48.0 | 0.498 |
| 0.2 | 85.6 | 48.0 | 98.1 | 1.9 | 52.0 | 0.460 |
| 0.15 | 83.2 | 42.0 | 98.6 | 1.4 | 58.0 | 0.406 |
| 0.1 | 81.0 | 30.0 | 99.1 | 0.9 | 70.0 | 0.291 |
| 0.05 | 78.6 | 10.0 | 99.6 | 0.4 | 90.0 | 0.106 |
Validation of stability of prediction model through crossing method
| Accuracy (%) | Sensitivity (%) | Specificity (%) | False positive rate (%) | False negative rate (%) | |
|---|---|---|---|---|---|
| Model (cut-off = 0.85) | 87.3 | 85.9 | 88.4 | 11.6 | 14.1 |
| Bootstrap internal validation (1,000 resamples) | 86.8 | 84.9 | 88.0 | 12.0 | 15.1 |
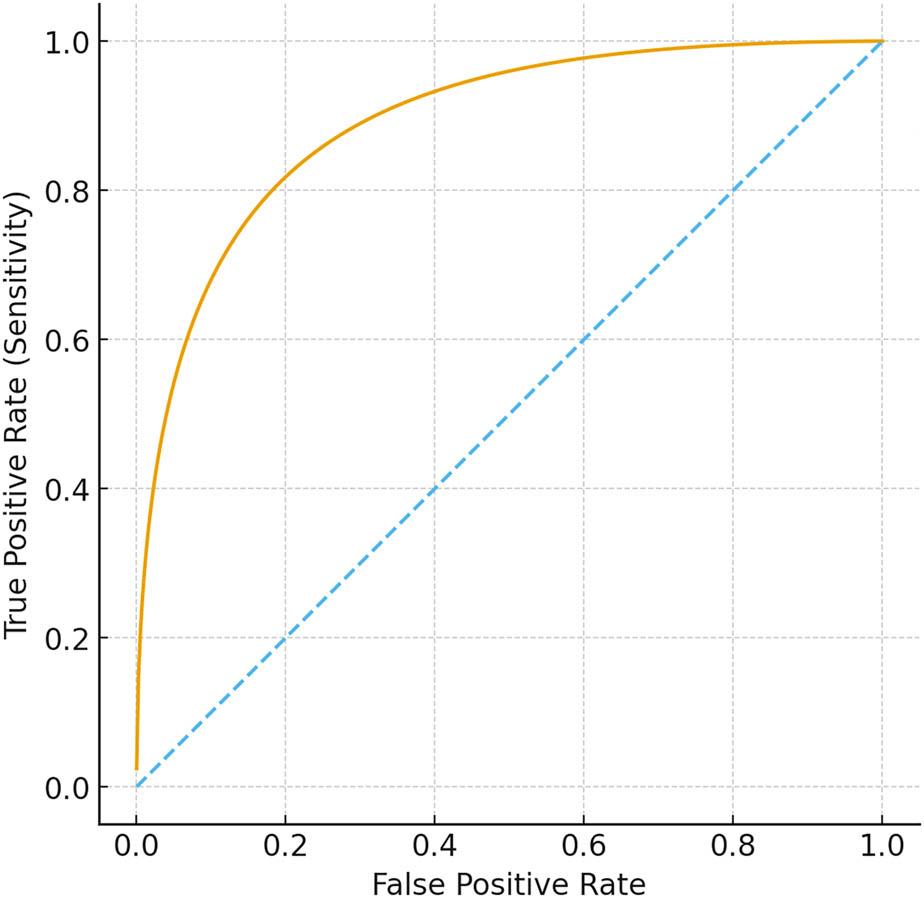
ROC curve for the multivariate logistic regression model predicting nonhealing at 12 months after root canal treatment
Chronic periapical periodontitis is a common endodontic condition in which radiographic evaluation plays a key role in assessing treatment response [13,14]. Although periapical radiographs are routinely used in clinical practice, previous studies have mainly focused on long-term healing rates or general prognostic factors, and few have examined the quantitative value of early radiographic changes as predictors of treatment outcomes. The present study addressed this gap by systematically evaluating periapical radiograph sign changes at 3, 6, and 12 months after root canal treatment and identifying early radiographic indicators associated with nonhealing.
The research results of Siddique et al. [15] presented prominent decreases in the periapical radiograph signs X, Y, L, and H in patients with combined periodontic–endodontic lesions after root canal treatment. Similarly, X, Y, L, and H were found to have sharp decreases in patients victimized by chronic periapical periodontitis following root canal-based management in the present study, and they tended to decrease with time after treatment. This progressive reduction reflects the gradual repair of periapical bone defects and the regression of inflammatory lesions, in line with existing evidence showing that successful endodontic therapy leads to continuous radiographic improvement during the first year [16].
However, not all lesions healed, highlighting the need to identify early prognostic markers. Our results showed that patients in the unhealed group exhibited significantly larger X, Y, L, and H values throughout follow-up, and importantly, the 3-month measurements were strong predictors of 12-month healing, as evidenced by the high overall predictive accuracy (86.96%). This finding is clinically meaningful, as it suggests that the lack of early radiographic improvement may indicate persistent infection or incomplete debridement. The previous study similarly reported that early radiographic stagnation often correlates with poorer healing [17]. In contrast, we found no differences in lesion size between groups, which aligns with reports by Azim et al. [18] and Li et al., indicating that the pretreatment lesion size alone is not a reliable predictor of healing.
In addition to radiographic findings, several treatment-related factors were associated with nonhealing. Root filling >2 mm, overfilling, coronal microleakage, and retained instrument fragments were identified as independent risk factors, findings that are in agreement with the previous studies [18,20,21,22]. Overextended fillings may irritate periapical tissues, and coronal microleakage permits bacterial re-entry, both of which hinder healing. Retained instrument fragments may prevent adequate cleaning of the canal and contribute to persistent infection. Conversely, retreatment during follow-up was a protective factor, likely because it re-establishes canal patency and allows for improved debridement, emphasizing its value in managing early signs of non-healing.
It is illuminated that coronal restoration materials of inlay was in relation to poor prognosis of patients with cracked teeth following root canal-based management [19]. In this study, coronal restoration materials of inlay was discovered to be a risk factor for nonhealing of tooth apexes in patients. The possible reason is that as an indirect repair means, inlay is characterized by a relatively large amount of tooth preparation and prolonged border line design, which may increase the risk of subsequent caries to a certain extent. Additionally, the probability of infections will be incremented if the inlay fails to reach the optimal sealing efficiency and the patients do not form postoperative habits like regular disinfection and good oral hygiene, thereby posing impacts on the healing of tooth apexes.
Despite these encouraging results, the study has limitations. First, the small sample size and retrospective design might result in selection bias. Second, the follow-up period was limited to 12 months. Although early radiographic healing within the first year is widely used as an indicator of treatment response, longer observation periods (≥24 months) are recommended by some clinical guidelines to confirm the final success of root canal treatment. Therefore, our findings mainly reflect early healing outcomes rather than long-term prognosis. Third, the model was not externally validated, so its predictive value for the healing of tooth apexes in patients of different races, from different regions, and treated in hospitals of different levels was not clarified. Finally, the indicators included in this study were not comprehensive enough, and there might be omission of important indicators. In the future, therefore, multicenter prospective studies with larger sample sizes and longer follow-up durations are warranted to further validate these results and enhance the clinical applicability of the model.
There were significant decreases of periapical radiograph signs in patients victimized by chronic periapical periodontitis following root canal-based management, suggesting gradual repairing and healing of periapical tissues after treatment, and reflecting the effectiveness of root canal treatment. Moreover, coronal restoration materials of inlay, root filling >2 mm and overfilling, coronal microleakage, instrument fracture, and increases in X, Y, L, and H at 3 months after treatment emerged as risk factors for, and retreatment following surgery functioned as a protective factor against non-healing at 12 months after root canal treatment in patients suffering from chronic periapical periodontitis. Monitoring periapical radiograph signs and identifying other risk factors after root canal treatment can help dentists make more accurate assessment of patients' prognoses in the early stage of root canal treatment, so that timely intervention measures can be taken to improve clinical efficacy.
Xiaohui Hu and Xiaoli Zhou designed this study and wrote the manuscript.
Xiaohui Hu https://orcid.org/0009-0001-0836-0700
Xiaoli Zhou https://orcid.org/0009-0007-5169-8540
This study was approved by the ethics committee of our hospital (No. JN. No20210432c0040912[113]).
The authors have no potential conflicts of interest to declare.