
Obesity and overweight have become a major public health issue in developed countries in the 21st century. It is a disease that significantly affects metabolism and can lead to dysfunction across multiple systems in the human body. Excess body mass - particularly abdominal obesity - is a potential indicator for conditions such as cardiovascular disorders, type 1 diabetes, and musculoskeletal diseases. It is classified by an elevated body mass index (BMI). Body Mass Index of ≥30 kg/m2 is defined as obesity [1]. Approximately 50% of patients diagnosed with diabetes are obese. What is more, 25%–30% of those seeking bariatric surgery report emotional struggles related to depression. In the United Kingdom, 2.3%–2.6% of the healthcare budget is allocated to the treatment of people with obesity and its related complications. [2] A BMI of >25 kg/m2 is associated with a 30% higher overall mortality rate; among individuals with vascular disease, this increases to 40%, and for those with diabetes, 60%–120%. Furthermore, obesity has been connected to a greater risk of cancer [3]. In 1998, the National Institutes of Health officially recognized obesity as a disease. Later, in 2013, the American Medical Association also voted to define obesity as a medical condition that requires treatment and proactive prevention. These declarations have influenced healthcare policy; however, one-third of adult Americans continue to struggle with obesity [4], and globally, more than 43% of adults were overweight and 16% were struggling with obesity in 2022 [5].
Stigmatisation is a common phenomenon in contemporary society. It is a major source of social inequality and a key factor in the deterioration of social relationships, contributing to elevated stress levels and negatively affecting both mental and physical health [6]. Goffman, a Canadian-born American sociologist, described stigma as ‘an attribute that is deeply discrediting’ and observed that a person subjected to stigmatisation becomes ‘from a whole and usual person to a tainted, discounted one’. This phenomenon can be seen as a threat to one's self-confidence and is associated with lower educational attainment. Furthermore, it renders social life for both the stigmatized and the stigmatizers more difficult, dangerous, and unpredictable [7]. It often leads to prejudice, social disintegration, and depression [8].
Individuals struggling with obesity often fall victim to stigmatisation - a phenomenon that is becoming increasingly widespread. Over the past years, the rate of weight-based discrimination in the United States has rizen by a staggering 66%, with the prevalence of obesity stigmatisation now comparable in scale to racial discrimination [9]. Level of discrimination tends to increase with the severity of obesity; for instance, in Germany, 5.6% of individuals with normal weight or overweight reported experiencing stigmatisation, compared to 38% of those with class III obesity [10]. Weight-based stigmatisation affects nearly every aspect of life and can have both psychological and physiological consequences, including an elevated risk of diabetes, oxidative stress, increased C-reactive protein levels, and emotional issues such as depression, anxiety, and low self-confidence, which can lead to eating disorders [11]. Research has also shown that people with obesity face disadvantages in employment, perceive weight bias from friends and family, experience prejudiced treatment in healthcare settings, and encounter bias from teachers and peers [12]. Despite its widespread impact, obesity stigma remains an area in need of deeper scientific investigation.
Our paper aims to review the current scientific literature on selected determinants of obesity stigma, focusing on five key factors: sex, race, age, income, and education. The novelty of our study lies in analysing these major determinants collectively within a single paper. While most existing studies tend to examine only one determinant in isolation, we believe that adopting a holistic perspective is essential for fully understanding the nature and impact of obesity stigma in society.
For the present review, studies were sourced via the PubMed (MEDLINE) and Google Scholar databases. Included papers investigated one or more of the selected determinants of obesity stigma: sex, race, age, income, and education. Studies addressing weight bias and the general description of obesity were also considered. Only articles written in English were included. The exclusion criteria were secondary research articles, case reports, repeated publications, review papers, and articles written in languages other than English. Of the studies used to describe the selected determinants, 86% were published after 2013. The remaining 14%, published before 2011, were included because of the significance and value of their findings.
The screening was conducted manually by six researchers. In total, 2,047 studies were initially identified. Of these, 1,122 were further screened by reading abstracts. From this process, 38 studies were chosen for full-text analysis. Following a detailed examination of the full texts, 24 papers were excluded, resulting in a final selection of 14 studies (13,14,15,16,17,18,19,20,21,22,2 3,24,25,26).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) was used to conduct this review. The predefined search terms included combinations of the following: ‘weight bias’ or ‘obese stigma’ or ‘weight discrimination’ or ‘obesity prejudice’ AND ‘determinant’ or ‘sex’ or ‘gender’ or ‘race’ or ‘skin color’ or ‘ethnicity’ or ‘age’ or ‘senior’ or ‘income’ or ‘economic status’ or ‘education’ or ‘educational attainment’. Figure 1 presents the flow diagram of the review.
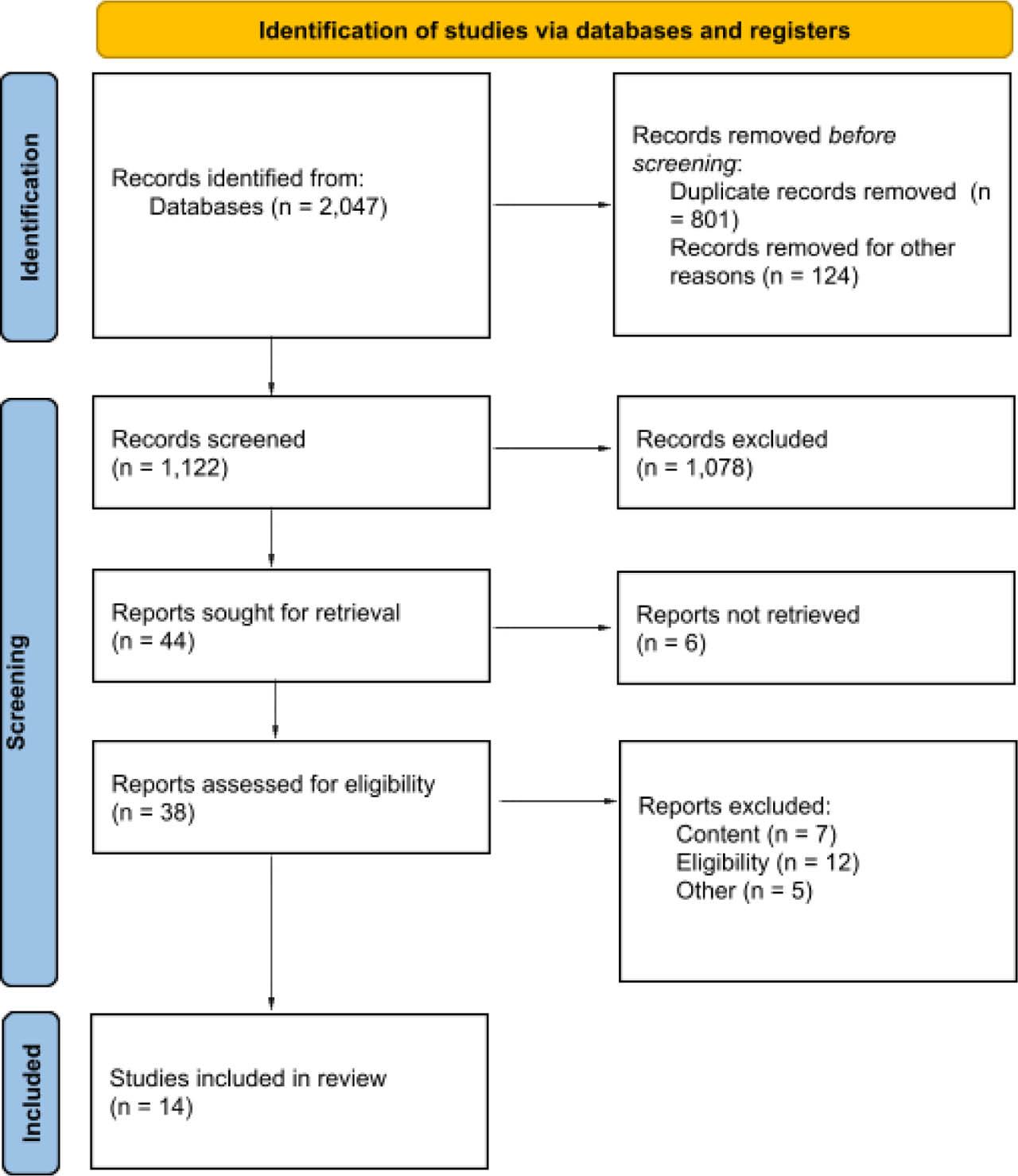
Flow diagram of the review
The included studies were separated into five groups and analyzed. Each one corresponds to one determinant: age, income, race, sex, and education. In our review, we examined the association between obesity stigma and the determinants that influence and exacerbate stigmatisation in various societies. The outcome measurements included, but were not limited to, odds ratios, hazard ratios, and correlations. Sex and/or gender dimensions of the research were defined by source studies used in the review.
The correlation between experiencing weight-based stigmatisation and low income was examined in a 2019 study from the United States. This study focused on a group of rural women with higher body weights living in the Midwest. In total, 25 women were interviewed. Female participants of the study had a BMI exceeding 30 kg/m2 and reported incomes of less than twice the federal poverty guideline. Some were also enrolled in income-based social assistance programmes. The interviews explored various aspects of weight-based discrimination, including bias in healthcare settings. Sixteen of the 25 participants reported experiencing prejudice in medical environments that they attributed solely to their weight. The study also discussed the effects of weight stigma, particularly in relation to healthcare. Reported consequences included avoidance of medical care due to previous negative experiences and a perception of being denied care [13].
Another study explored the associations among body perceived weight stigma, body weight, and mental health outcomes in women, emphasizing the role of race/ethnicity and socioeconomic status as intersecting factors. In contrast to the previous article, this study suggested that higher socioeconomic status may serve as a burden for overweight women [12]. In employment settings, women with obesity often face reduced job opportunities, unfair treatment in the workplace, and lower earnings compared with their non-obese peers. However, the statistics presented in the study indicate that women with household incomes below $25,000 and those earning between $50,000 and $75,000 have lower overall mental health scores than women with household incomes exceeding $75,000. Specifically, women in the lowest income bracket scored 3.50 units lower, while those in the middle-income range scored 1.40 units lower than women in the highest income group. These findings suggest that women from lower-income households are more likely to face mental health challenges, which is closely interlinked with experiences of weight-based discrimination [14].
The effects of weight stigma among individuals with lower socioeconomic status were also examined in a 2022 study aimed at understanding obesity discrimination among youth in low- and middle-income countries. Adolescents aged 15–19 years from Brazil, South Africa, and Indonesia took part in the study. The findings revealed that in each of these countries, the number of adolescents reporting experiences of weight-based discrimination was alarmingly high. Both male and female participants expressed dissatisfaction with their weight and reported internalising weight bias. A significant majority (71.8%) indicated that weight stigma had negatively impacted their mental health. Another major concern was the influence of negative weight perceptions on eating behaviour, reported by 23.1% of participants. Only a small proportion (5.1%) stated that weight-related comments had motivated positive health behaviours, such as engaging in regular exercise [15]. The findings from studies on income are summarized in Table 1.
Studies on the relationship between obesity stigma and income
| No. | Methodology | Results | Citation |
|---|---|---|---|
| 1 | Subjects: Twenty-five rural, low-income women—earning less than twice the poverty guidelines established by the Department of Health and Human Services or enrolled in a social assistance programme—currently or previously classified as obese (BMI >30 kg/m2). | Sixteen women reported experiencing obesity stigma in healthcare settings; all participants described encountering some form of weight-related stigma. | [13] |
| Main outcome measures: Data were obtained through face-to-face interviews using semi-structured protocols. Researchers coded the interviews using NVivo 11 software. Finally, all codes were compared to identify patterns that emerged as key themes. | |||
| 2 | Subjects: A sample of adults aged 35–89 years participated in a random-digit telephone survey (1,641 men and 2,203 women, including 1,086 Black Americans). | The study demonstrated that individuals with an income below $25,000 were more negatively affected by weight discrimination. Additionally, women with household incomes below $25,000 and between $50,000 and $75,000 reported lower aggregate mental health scores than those with household incomes exceeding $75,000. | [14] |
| Main outcome measurements: The SF-36, EuroQol, Quality of Life Scale, Health and Activity Limitation Index, and Health Utilities Index were used. | |||
| 3 | Subjects: Adolescents aged 15–19 years from low- or middle-income countries—Brazil, South Africa, and Indonesia (522 male and 678 female participants). For participants under 18 years of age, parental consent was obtained. Researchers used a national database to identify families with adolescents, then contacted them using a randomized method. | In South Africa, 73.3% of females and 64.7% of males reported experiencing weight stigma; in Brazil, these figures were 92.6% and 75.9%, respectively; and in Indonesia, these figures were 46.2% and 53.8, respectively. Overall, the majority of adolescents (71.8%) indicated an adverse effect of weight bias on their mental health. | [15] |
| Main outcome measurements: Researchers conducted a computer-assisted telephone interviewing survey, followed by qualitative thematic data analysis and statistical analysis using SPSS v.23. | |||
BMI, body mass index; SPSS, Statistical Package for the Social Sciences
A study involving 32 women—8 of whom were obese and 24 who had bariatric surgery and as a result lost weight—explored their experiences of stigmatisation in various formal and informal settings. The findings indicated that age significantly influences the nature of weight-based stigmatisation. Younger women who were overweight encountered different challenges than older women with similar body mass. For the younger group, the stigma was particularly pronounced in social contexts, especially in interactions with friends, family, and members of the opposite sex. Women who had lost weight reported that they were no longer perceived as ‘asexual’ or ‘one of the boys’. This shift in perception was closely tied to improved self-esteem and confidence, leading to notable changes in behaviour; avoidance and social isolation were no longer dominant coping strategies. By contrast, older women cited health concerns as the primary motivation for undergoing gastric sleeve surgery and losing weight. They expressed satisfaction with their improved physical capabilities and the reduced concern among family members about their well-being. Interestingly, older women with excess body mass reported feeling less discriminated against than their younger counterparts [16].
Studies show that obesity is highly stigmatized across all age groups. However, the severity of stigmatisation appears to vary significantly with age, with adults generally demonstrating more tolerance than children. This difference may be attributed to adults' broader life experiences, which often lead to a deeper understanding of the range of factors that contribute to obesity, including genetic, psychological, and metabolic influences. Additionally, the higher prevalence of obesity among adults makes excess weight less uncommon and, consequently, more socially acceptable within this group. These findings underscore the importance of early education and awareness across all age groups and suggest a potential developmental trend in which stigmatising attitudes towards obesity decrease from childhood to adulthood [17].
Research conducted among Korean women indicates that younger adults are more likely to overestimate their weight, regardless of their actual BMI, whereas older individuals with obesity frequently have a lower perception of their weight and may not see the need for weight reduction. This trend reflects the heightened sensitivity to obesity stigma among young women. Studies show that women with a healthy weight who perceive themselves as people with obesity are at a higher risk for developing psychological problems. Younger adults are more susceptible to societal beauty standards, which place a strong emphasis on thinness. For young women, achieving an ideal body image is primarily motivated by the desire for social acceptance. By contrast, for older women, the motivation to reach a normal weight is more strongly tied to concerns about the serious health consequences of obesity [18]. The findings from studies on age are summarized in Table 2.
Studies on the relationship between obesity stigma and age
| No. | Methodology | Results | Citation |
|---|---|---|---|
| 1 | Subjects: Patients with a BMI of ≥35 kg/m2 who had never undergone bariatric surgery, and patients who had undergone LAGB and lost at least 50% of their excess weight. | Among the 32 women—8 with obesity (BMI of ≥35 kg/m2) and 24 who had lost 50% of their excess weight following bariatric surgery—the main shared themes included social impact and isolation, health implications, self-confidence, and experiences of unkind behaviour. | [16] |
| Main outcome measures: Audio recordings were made and transcribed during all focus group sessions. | |||
| 2 | Subjects: The study included 356 college students (mean age of 20.6 years; an average BMI of 23.3 kg/m2), 56% of whom were female. In terms of ethnicity, 54.3% were White, 23.3% Asian, 8.9% African American, 6.9% Hispanic, 1.4% Native American, and 2.9% identified as other; 2.3% of participants did not specify ethnicity. | Adults were less stigmatized than children, with men scoring 4.34 and women 3.85, compared with girls at 5.15 and boys at 4.77 (higher scores indicate greater stigmatisation). | [17] |
| Main outcome measures: A questionnaire featuring drawings of individuals with various types of disabilities. Participants were asked to select the one they liked best. Data were analysed using one-way ANOVA. | |||
| 3 | Subjects: Data were obtained from the 2016 Korean Study of Women's Health-Related Issues (K-Stori), a nationally representative, population-based, cross-sectional survey aimed at evaluating health awareness and needs among women at various life stages: adolescence (ages 14–17), childbearing (ages 19–44), pregnancy and postpartum (ages 19–44), perimenopause (ages 45–64), and older adulthood (ages 65–79). | Younger Korean women, more influenced by societal beauty standards, were more likely to engage in weight control, while older women with obesity generally showed little intention to lose weight. | [18] |
| Main outcome measures: Descriptive statistics of socio-demographic variables were analyzed and compared across age groups. Categorical variables were examined using the chi-square test, while continuous variables were analyzed with one-way ANOVA. To evaluate the accuracy of body weight perception, the weighted Kappa coefficient was calculated. | |||
BMI, body mass index; ANOVA, one-way analysis of variance; LAGB, laparoscopic adjustable gastric banding
In 2014, Hilbert et al. conducted a study to establish population norms and assess the psychometric properties of the Weight Bias Internalization Scale (WBIS) using a representative German sample. Internalized weight stigma has been found to play a key role in both the development of stigmatising attitudes and the experience of discrimination. The final research sample included 1,092 participants - 514 women and 578 men - with an average BMI of 28.30 kg/m2. Notably, 85.8% of participants reported having less than 12 years of education. Those with lower levels of education were found to have significantly higher WBIS scores than those with higher educational backgrounds [19].
A similar study examined the occurrence, intensity, social and demographic associations of weight stigma internalisation among three separate adult groups in the United States. A total of 3,504 adults completed self-reported surveys assessing demographic information, current weight status, dieting behaviours, past exposure to weight-related bias, and internalisation of weight stigma. More than 80% of participants reported having a high level of educational attainment. Despite this, the results indicated a heightened vulnerability to elevated weight bias internalisation among adults with lower levels of education [20].
A Spanish study conducted in 2023 assessed the extent of ostracism and the frequency of discrimination associated with obesity within the Spanish population, along with the main determinants influencing these experiences. In total, 1,018 participants were recruited for a multicentre observational study. Three surveys were used to measure negative attitudes towards individuals with obesity: the Antifat Attitudes Scale (AFA), the Stigmatizing Situations Inventory (SSI), and the WBIS. Notably, education levels did not show a statistically important correlation with the results of any of the questionnaires [21]. The findings from studies on education are summarized in Table 3.
Studies on the relationship between obesity stigma and education
| No. | Methodology | Results | Citation |
|---|---|---|---|
| 1. | Subjects: A sample representative of the German population was recruited using a Kish selection grid. Participants provided their own weight and height measurements for BMI calculation. Respondents who were not classified as overweight or obese, or who provided incomplete data, were excluded from the analysis. The final study sample consisted of 1,092 participants. | Participants with lower levels of education had substantially higher WBIS scores compared to those with higher educational attainment. (<12 years: M = 2.68, SD = 1.18; ≥12 years: M = 2.47, SD = 1.25; p < 0.05). | [19] |
| Main outcome measures: WBIS, BDI-PC, and SSS-8. Scores from the scales were analysed and interpreted. | |||
| 2. | Subjects: The first sample consisted of 456 members of the Obesity Action Coalition. The second sample included 519 individuals recruited via Mechanical Turk (MTurk—a platform on which businesses and researchers hire remote workers to complete small tasks, such as surveys, data labelling, and content moderation, for micro-payments). The third sample comprized 2,529 individuals from a national online survey panel conducted by Survey Sampling International, LLC. In all, 3,504 participants completed self-report measures and surveys. | The results indicated that adults with a high BMI and lower levels of education are more vulnerable to elevated weight bias internalisation. Education demonstrated a negative association with bias internalisation (B = −0.07; p = 0.019). | [20] |
| Main outcome measures: Modified WBIS; statistical analyses were conducted. | |||
| 3. | Subjects: In total, 1,018 participants were enlisted from 13 obesity units in Spain. | Education did not show a significant correlation with obesity stigma across the three questionnaires. | [21] |
| Main outcome measures: AFA, SSI, and WBIS; statistical analyses were conducted. | |||
BMI, body mass index; BDI-PC, Beck Depression Inventory for Primary Care; SSS-8, Somatic Symptom Scale-8; AFA, Antifat Attitudes Scale; SSI, Stigmatizing Situations Inventory; WBIS, Weight Bias Internalization Scale; M, mean; SD, standard deviation
A study conducted in Germany among 692 randomly selected adults (aged ≥18 years) examined the correlation between sex and experiencing weight-related stigma. The analysis focused on differences in societal perceptions of weight, considering sex, socio-economic status, and their potential interdependencies. Various aspects of stigma were assessed using scales measuring fear of overweight, emotional reactions to individuals with overweight, and the tendency to maintain social distance. The study found that men who were overweight experienced more negative emotional responses and demonstrated a stronger inclination toward social distancing. These findings suggest that, within German society, the male sex is significantly associated with more negative perceptions of being overweight. In light of intersectionality theory, the study highlights how weight stigmatisation may reinforce or exacerbate existing social inequalities [22].
The study conducted by van Zutven et al. explored how concerns about weight and body shape affect psychological well-being in an Australian population sample of women and men, including individuals with and without obesity. The findings showed that such concerns significantly influenced key outcomes, including social support, life satisfaction, and psychological distress for both sexes. Notably, binge eating was found to mediate the association between obesity and life satisfaction in men only, indicating that disordered eating behaviors may adversely impact their overall well-being. However, binge eating alone was not independently associated with psychosocial impairment. An important contribution of the study lies in its insights into obesity stigma and its psychological effects. It found that weight and shape concerns - often intensified by societal stigma - are linked to increased distress and lower life satisfaction in individuals with obesity. The study also underscored a gendered dimension to obesity stigma, revealing that men with obesity who engage in binge eating report lower life satisfaction, possibly due to growing societal and media pressures that promote a muscular male body ideal. These findings indicate that obesity stigma significantly affects men as well, particularly as cultural expectations around male body image continue to evolve [23].
Wee et al. examined in their study the influence of various quality of life (QOL) domains on health utility and revealed sex-specific aspects of obesity stigma. QOL factors were generally less predictive of health utility among men, with the notable exception of Hispanic men, for whom work life accounted for 12% of the variance after controlling for demographics and BMI. In comparison, for women, work life was a more substantial contributor, explaining more than 20% of the range in health status valuation. Social stigma and sexual life for women emerged as key QOL domains affecting health utility. Specifically, social stigma alone accounted for 6% of the difference in health utility, aside from BMI and demographic factors. These findings highlight the differing impact of obesity stigma across sexes. In women, social stigma plays a significant role in shaping perceived health utility, which may strongly influence decisions to pursue weight loss treatments such as bariatric surgery. The study underscores the importance of developing targeted interventions that address social stigma and impairments in sexual function to improve well-being and health outcomes among women with high Body Mass Index [24]. The findings from studies on sex are summarized in Table 4.
Studies on the relationship between obesity stigma and sex
| No. | Methodology | Results | Citation |
|---|---|---|---|
| 1 | Subjects: A total of 692 adults, randomly selected. | Men reported experiencing greater stigmatisation than women. | [22] |
| Main outcome measures: Data were collected through computer-assisted telephone interviews. Analyses were conducted using SPSS v.22, and Mann–Whitney U tests were used to assess the significance of mean differences between groups. | |||
| 2 | Subjects: Women and men in the general population were classified as obese or non-obese; group sizes were as follows: women—obese (n = 276), non-obese (n = 1,220); men—obese (n = 169), non-obese (n = 769). | For both sexes, weight and shape concerns, and physical health, equally mediated the link between obesity and psychosocial outcomes—including psychological distress, life satisfaction, and social support. Binge eating had a modest effect, reaching significance only for men's life satisfaction. | [23] |
| Main outcome measures: To determine whether the effects of mediators on the relationship between obesity and outcomes differ by sex, a moderated mediation analysis was conducted. | |||
| 3 | Subjects: A total of 337 primary care patients with moderate to severe obesity, recruited from four diverse primary care practices in Greater Boston. | Among women, social stigma and sexual life were significant contributors to health status, while work life emerged as a notably more influential factor for men. | [24] |
| Main outcome measures: Descriptive analyses were conducted to profile health utility and QOL scores by sex and race/ethnicity. Separate multivariable linear regression models for each sex and race/ethnicity subgroup explored the relationships between demographic characteristics, BMI, QOL domains, and health utility. Changes in model R2 following the addition of each variable were analysed to assess the relative importance of each factor. | |||
BMI, body mass index; QOL, quality of life; SPSS, Statistical Package for the Social Sciences
A study by Chao et al. explored the public perspective of bariatric surgery, focusing on the perspectives of Black individuals within the broader context of the obesity epidemic and its associated stigma. Using semi-structured interviews with participants - most of whom were Black and had not considered bariatric surgery - the researchers investigated deeply ingrained stigmatising beliefs about obesity and personal identity. The findings revealed that many participants internalized societal stigma, perceiving obesity as a personal failure rooted in a lack of willpower. Consequently, weight loss methods considered socially acceptable were those involving discipline, such as diet and exercise, while bariatric surgery was often viewed as an illegitimate ‘shortcut’. This study underscores how obesity stigma not only shapes attitudes toward treatment options but also reinforces barriers to care, further entrenching the stigma itself [25].
A study by Brewis et al. examined weight stigma, which has been well documented in high-income, industrialized societies—regions often referred to as the global north, including North America, Europe, and Australia, and largely dominated by white populations. In these societies, weight bias is linked with significant psychological distress, discrimination, and negative health behaviours, which can further exacerbate issues such as depression and weight gain. Traditionally, such stigma has been viewed as specific to cultures that place a high value on thinness. However, recent evidence indicates that obesity stigma is also emerging in countries classified as middle - and low-income - the global south. Signs of this include high levels of both implicit and explicit weight stigma, ethnographic evidence of anti-obesity beliefs, the spread of ‘obesity talk’, and reports of mental and material damage due to discrimination caused by weight. Notably, this stigma persists even in regions where severe malnutrition remains a pressing concern [26].
In a cross-sectional study, Wee et al. examined the effects of obesity-related social stigma and other quality of life factors among primary care patients with moderate to severe obesity. A total of 337 patients aged 18 to 65 years, each with a BMI of 35 kg/m² or higher, were included from various primary care practices in the Greater Boston area. Health utility - reflecting patients' assessment of their current health and weight status - was measured using a series of standardized gambling scenarios. Impact of Weight on Quality of Life-lite tool was used to evaluate obesity-specific QOL domains. The findings revealed that the influence of QOL factors on well-being varied across demographic groups. Social stigma emerged as a significant contributor to reduced utility among Caucasian patients. Impaired sexual function was notable for African American women, though its impact appeared less pronounced. For Hispanic patients, work life was a key factor, accounting for more than 20% of the variation in utility. Interestingly, overall QOL scores were less effective at explaining variation in utility than specific individual domains [24]. The findings from studies on race are summarized in Table 5.
Studies on the relationship between obesity stigma and race
| No | Methodology | Results | Citation |
|---|---|---|---|
| 1 | Subjects: Thirty-two participants, of whom 88% identified as female, 72% as Black, 3% as Hispanic, 3% as Pacific Islander, 3% as mixed race, and 19% as White. | Participants internalized the social stigma surrounding obesity, perceiving it as a personal failure attributed to a lack of willpower. Stigma emerged as the primary reason individuals declined bariatric surgery. The study suggests that healthcare providers could play a pivotal role in increasing the acceptance of bariatric surgery by shifting the social narrative away from stigmatising obesity and toward prioritising health. | [25] |
| Main outcome measures: The researchers likely employed thematic analysis to identify and examine patterns within the interview data. This process involved coding transcripts, identifying recurring themes, and interpreting the findings within the broader context of existing literature on obesity stigma and perceptions of bariatric surgery. | |||
| 2 | Subjects: Ethnographic studies conducted across regions of the global north and south. | Weight stigma, widely prevalent in the United States and other regions of the global north, has a substantial negative impact on both emotional and physical health. Early evidence also suggests the presence and spread of weight stigma in various regions of the global south. | [26] |
| Main outcome measures: | |||
| In Brazil, curvier body types were considered attractive in the early 2000s but were no longer viewed as desirable by 2015. | |||
| In Western Polynesia, larger body sizes continue to be culturally valued. | |||
| Compared to the United States, the United Kingdom, and New Zealand, American Samoa, Mexico, and Paraguay exhibited a higher prevalence of anti-fat norms. | |||
| 3 | Subjects: A sample of 337 patients with moderate to severe obesity was recruited from four distinct primary care practices across Greater Boston | Obesity-related social stigma had a disproportionately negative impact on the well-being of Caucasian patients. Weight-related work impairments were especially significant among Hispanic patients. Among African American women, impaired sexual function also contributed to reduced well-being, although its impact appeared modest. | [24] |
| Main outcome measures: Descriptive statistics were used to characterize health utility and quality-of-life scores by race/ethnicity and sex. Multivariable linear regression models, categorized by sex and race/ethnicity, assessed the impact of demographic factors, BMI, and QOL domains on health utility. Changes in model R2 with the addition of each variable were analysed to determine the relative importance of each factor. | |||
BMI, body mass index; QOL, quality of life
The reviewed studies offer a comprehensive overview of the various mechanisms underlying weight-based stigma and its impact across diverse demographic groups. The evidence highlights the widespread nature and significant consequences of weight stigma, affecting individuals across different income levels, age groups, educational backgrounds, sexes, and racial or ethnic identities.
The role of income in weight-based discrimination is substantial. Research consistently shows that weight bias tends to be more prevalent among people with lower income status, particularly within healthcare settings, and they are at elevated risk of experiencing a variety of emotional distress linked to stigmatisation.
The reviewed studies highlight consequences such as weight dissatisfaction, disordered eating, mental health disorders, and low self-confidence - issues that are common within the population affected by elevated Body Mass Index, but especially pronounced among those with lower incomes. Prejudice in medical environments is particularly concerning, as it can take many forms, from dismissing or overlooking patients' concerns to outright denial of care. Such experiences further marginalize individuals and contribute to ongoing disparities in health and well-being.
Preventing weight-based discrimination, particularly in healthcare settings, requires a multifaceted strategy. Educating healthcare professionals about the consequences of weight bias and how significant is treating patients with compassion. Another key approach is to promote a holistic perspective on health utility and personal welfare rather than focusing solely on weight. Public health campaigns should promote understanding of the harmful effects of weight stigmatisation and challenge prevailing stereotypes. Furthermore, research highlights that weight bias disproportionately affects low-income populations. Addressing these specific issues faced by these communities is vital and ensures equitable access to appropriate support and resources. Tailored interventions that consider the intersection of income and weight stigma are necessary to reduce disparities and promote more inclusive healthcare practices.
Very few individuals living with overweight or obesity have likely gone through life without hearing at least one unkind comment about their body. Society often attributes obesity to internal factors such as overeating or a lack of exercise, overlooking the far more complex reality of the condition. Younger individuals, particularly adolescent girls, tend to be more sensitive to others' opinions. Many report that their motivation to lose weight is driven more by a desire for social acceptance or attention from the opposite sex than by health concerns. By contrast, older individuals are more likely to pursue weight loss for health-related reasons.
Adults generally cope with stigma more effectively than teenagers, largely because of greater life experience and a more realistic understanding of social cruelty. Additionally, obesity tends to be less stigmatized among adults because excess weight is more common and socially accepted in this group. Adults are often less focused on physical appearance and more inclined to judge others based on character, which may contribute to a more tolerant social environment.
Stigmatized individuals are often excluded from social life, which can further damage their self-confidence and increase feelings of insecurity. This social isolation may further proceed to serious mental distress such as eating disorders, depression and even self-harm.
While it may be impossible to eliminate weight-based stigma across all age groups - because we cannot control the actions of others - there are meaningful steps that can be taken. Children may exhibit unkind behaviour, often reflecting a lack of proper guidance at home. It is therefore essential to raise awareness in public, especially parents, about the complicated nature of experiencing obesity. It is frequently rooted in psychological and eating disorders, not simply in overeating or a lack of willpower. Raising awareness is crucial because many people remain unaware of the harm caused by bullying and stigma, both of which can severely hinder an individual's efforts to regain their health. Education should also extend to those living with obesity. Government support is vital in this regard - funding for dietitians, gyms, swimming pools, and other accessible fitness facilities would help ensure that all individuals, regardless of income, can improve their health in a supportive environment.
Both Hilbert et al. [19] and Puhl et al. [20] showed that an individual's level of educational attainment influences their experience of weight stigma. This was reflected in higher WBIS scores among individuals with obesity who had lower levels of education than among individuals with higher educational qualifications.
Stigmatisation has a profound effect on those subjected to it, impacting both mental and physical health. Hilbert et al. [19] provided evidence of this through their findings, which revealed a positive correlation between WBIS scores and both the Somatic Symptom Scale-8 (SSS-8) and the Beck Depression Inventory for Primary Care (BDI-PC). Overweight individuals with lower education levels not only had higher WBIS scores, but those scores were also linked with increased mood disorders and somatic complaints. These results underscore how obesity stigma can contribute to both psychological distress and physical symptoms, including abdominal discomfort.
Preventing obesity discrimination requires a comprehensive approach that combines education and broader social change to promote greater acceptance and understanding of the diversity of human bodies. The reviewed studies demonstrated that individuals with obesity and lower levels of education face greater stigmatisation than those with higher educational attainment. It is important to recognize that every level of education holds value. Challenging and dismantling stereotypes associated with lower educational attainment is essential, and this can be effectively addressed through targeted social campaigns that foster empathy, inclusion, and respect.
The reviewed studies reveal that society imposes stricter standards on women regarding physical appearance, placing greater pressure on them to remain thin. This societal pressure often results in harsh criticism and discrimination in both private and professional spheres. While men also face stigma related to obesity, its manifestations differ; social expectations surrounding male appearance tend to be less rigid, leading to a generally lower level of stigmatisation compared to women.
Nonetheless, the emotional and societal consequences of weight stigma are significant for both sexes. However, women are particularly vulnerable to experiencing low self-confidence, depression, and anxiety, whereas men may struggle with issues related to identity and self-worth. Effectively addressing obesity stigma requires recognising and addressing these sex-specific experiences and promoting more inclusive and accepting societal attitudes.
Media and popular culture play a key role and should work to promote body diversity, helping to reduce the pressure to conform to unrealistic beauty standards. School-based education and social campaigns must emphasize that a person's value is not determined by appearance, and that self-acceptance is crucial to mental well-being.
Men need support in redefining masculinity in ways that break away from stereotypes tied to physical strength and dominance. Campaigns targeting male audiences should promote healthy habits without resorting to ridicule or stigmatisation. It is essential to reinforce the idea that health encompasses not just physical appearance, but also mental and emotional well-being.
In summary, effectively combating the stigmatisation of obesity requires comprehensive educational, cultural, and social efforts that acknowledge and address the distinct experiences of both sexes. Only through such an inclusive approach can we foster a society in which all individuals feel accepted and respected, regardless of their appearance.
The reviewed studies underscore the complex relationship between race and obesity stigma, illustrating how these factors influence well-being and shape perceptions of weight-loss interventions. Chao et al. [25] found that Black individuals often internalize obesity stigma, perceiving it as a personal failure, which in turn discourages them from viewing bariatric surgery as a valid medical intervention. Brewis et al. [26] observed that obesity stigma is not confined to high-income societies; it is also emerging in countries with middle- and lower socioeconomic status. The spread of weight-related stigma in these regions—despite the continued presence of malnutrition—suggests a global shift in body image ideals. Cultural and economic influences increasingly prioritize thinness, even in contexts where food insecurity remains a serious concern. Wee et al. [24] further demonstrated that obesity stigma manifests differently across racial and ethnic groups. For Caucasian patients, social stigma has the most pronounced impact on well-being. Among African American women, impaired sexual function plays a notable role, while work-related challenges are especially significant for Hispanic patients. These results point out the critical role of culturally sensitive approaches to addressing weight bias and improving medical status across diverse communities.
The findings from these studies carry important implications for both clinical practice and public policy. Healthcare providers should develop tailored interventions that address the specific challenges experienced by different racial groups affected by obesity stigma. Culturally sensitive approaches that acknowledge these unique experiences may enhance the effectiveness of weight management programmes and promote more equitable healthcare outcomes.
Policymakers, meanwhile, should consider the broader health-related social factors that contribute to stigma associated with obesity - particularly within the context of racial disparities. Initiatives aimed at reducing obesity stigma, such as public health campaigns that promote self-acceptance and actively challenge harmful stereotypes, could be an important factor in improving quality of life for individuals with high Body Mass Index, especially within marginalized communities.
Understanding the relationship between obesity stigma and factors such as race, sex, income, education, and age can support the delivery of more personalized and equitable healthcare. Recognising that certain groups may face more intense stigma enables healthcare providers to offer targeted support, counselling, and interventions that are sensitive to each patient's social and cultural context. This approach may include supporting community-based programmes that address the social determinants of health, promoting educational initiatives to challenge obesity stigma, and advocating for workplace or school policies that foster inclusive, supportive environments for individuals living with obesity.
Future research should prioritize the inclusion of more diverse populations and further explore the global dimensions of obesity stigma, particularly in the global south. Broader and more representative samples are needed to capture the varied experiences of different communities. Future studies must analyse subjects by both race and sex to produce more accurate and reliable findings. Our review highlights that individuals facing different determinants of obesity stigma - such as race, income, education, sex, and age - experience a range of psychological challenges and are stigmatized in distinct ways. To develop practical solutions, each group must be examined separately and provided with tailored strategies to combat stigma. Additionally, future research should focus on patients who seek treatment for obesity through bariatric surgery or medication. As shown in the study by Chao et al. [25], individuals considering or undergoing bariatric surgery often face additional layers of stigma, which may lead to weight regain or deter them from pursuing treatment altogether. It is therefore crucial to identify ways to support and encourage individuals with obesity to seek care, ensuring that stigma does not obstruct their path to improved health.
The reviewed studies provide valuable conclusions into the complex correlation between weight bias and key demographic factors. Our review focused on five primary determinants that we consider most influential in the mechanism of obesity stigma: age, education, sex, race, and income. To ensure relevance and accuracy, we included only studies published in the 21st century, offering a contemporary perspective on the issue. To date, no other research group has conducted a review that brings together these specific determinants in a single analysis, making our work both original and innovative. Given that obesity stigma remains a significant public health concern, we believe our findings can contribute meaningfully to the development of future campaigns and strategies aimed at reducing obesity and the stigma associated with it.
This review has several limitations, including variability in study designs, sample sizes, and cultural contexts, which may influence the consistency and generalisability of the findings. Additionally, many results were based on self-reported, subjective data, which may be affected by individual perceptions and biases. Nonetheless, these studies highlight the importance of incorporating patient perspectives and recognising demographic differences when evaluating the impact of obesity-related QOL dimensions.
Obesity stigma continues to be a critical public health concern with extensive negative implications across different demographic groups. Lower socioeconomic status is strongly associated with increased exposure to weight bias, particularly in healthcare settings, contributing to elevated risks of mental health challenges such as low self-esteem. Younger individuals - especially girls - are more vulnerable to stigma because of societal pressures surrounding physical appearance, while adults tend to cope more effectively owing to greater life experience and self-acceptance. People with lower educational attainment experience higher levels of obesity stigma, which correlate with increased symptoms of depression and somatic complaints. Women are subjected to stricter societal standards regarding body image, resulting in greater stigmatisation and psychological distress compared with men, who tend to experience stigma in ways more closely tied to identity and self-worth. Black individuals often internalize obesity stigma, perceiving it as a personal failing and viewing bariatric surgery as an illegitimate solution, which discourages them from seeking medical treatment.
Understanding the mechanisms and influence of obesity stigma is crucial for developing effective interventions aimed at reducing stigma and improving health outcomes for individuals experiencing obesity. Advanced research in future is essential to deepen our understanding of how obesity stigmatisation operates in society and how best to address it.