
Tuberculosis (TB) caused by from infection with Mycobacterium tuberculosis (Mtb) continues to be a major contributor to global infectious disease-related morbidity and mortality. Despite decades of progress in diagnostics and treatment, TB continues to pose significant public health challenges, particularly in resource-limited settings [1]. According to the World Health Organization (WHO), TB remains among the top ten causes of death globally, with over 10 million people affected annually, many of whom remain undiagnosed or are not treated in time [2].
Traditional TB diagnostic models have relied heavily on centralized laboratory systems, which, although technically robust, often present substantial barriers to timely diagnosis. These systems typically require well-equipped facilities, cold-chain logistics, and highly trained personnel — resources that are often scarce in rural and underserved regions [3, 4]. Sample transport delays, high infrastructure costs, and long turnaround times have all been implicated in delayed case detection and ongoing transmission, particularly in high-burden countries [5, 6].
In recent years, the concept of decentralized or point-of-care (POC) testing has emerged as a promising strategy for improving TB diagnostic access and efficiency. By relocating diagnostic capabilities closer to the patient, decentralized approaches aim to overcome the logistical and infrastructural limitations of centralized testing [7, 8]. The global COVID-19 pandemic, while disruptive, also accelerated investments in diagnostic infrastructure, digital tools, and molecular technologies, inadvertently creating new opportunities to reimagine TB diagnostics through decentralized frameworks [9, 10].
An increasing number of studies have explored the utility of rapid diagnostic tests, automated molecular platforms, and community-based screening initiatives in decentralized settings [11,12,13,14]. However, despite these developments, the global implementation of decentralized TB diagnostics remains inconsistent. Challenges with quality assurance, financial sustainability, and community engagement, combined with skilled workforce shortages, continue to hinder widespread adoption [15,16,17,18].
While several reviews have addressed specific aspects of TB diagnostics or COVID-19's impact on laboratory systems [9, 10], there has yet to be a comprehensive synthesis of decentralized TB testing — including its enablers, barriers, and post-pandemic opportunities.
In light of this, this review aims to systematically examine the current landscape of decentralized TB diagnostic capacity in primary laboratories. Specifically, we (i) outline the limitations of centralized diagnostic systems; (ii) assess the benefits and practical challenges of decentralization; (iii) identify strategic opportunities enabled by technological and structural innovations post-COVID-19; and (iv) propose future directions to support sustainable and equitable TB diagnostic reform.
This narrative review synthesizes evidence on decentralized tuberculosis (TB) diagnostics, particularly in the post-COVID-19 context. Literature searches were conducted on PubMed, Scopus, and Web of Science and encompassed publications up to February 2025. The search strategy combined keywords such as “Tuberculosis,” “Decentralized testing,” “Point-of-care diagnostics,” and “COVID-19” using Boolean operators. Additional references were identified through manual screening of key papers.
Eligible studies included peer-reviewed articles focusing on TB diagnostic approaches in decentralized or primary laboratory settings. Original research, implementation studies, systematic reviews, and technical reports were included, while editorials, non-English-language articles, and studies unrelated to TB diagnostics or decentralization were excluded.
Initial screening based on titles and abstracts was conducted, with subsequent full-text evaluations for eligible studies. Relevant findings were extracted and organized thematically into five areas: centralized testing challenges, the benefits of decentralization, implementation barriers, technological enablers, and post-pandemic opportunities.
Additionally, we noted that most of the studies that were included were either observational, pilot implementation reports, or narrative reviews, as opposed to randomized controlled trials (RCTs) or large-scale prospective studies. This limits the overall methodological rigor and generalizability of our conclusions, and is explicitly acknowledged in the discussion.
Despite the technical accuracy and standardization associated with centralized tuberculosis (TB) diagnostic systems, several critical limitations hinder their effectiveness — especially in high-burden, resource-constrained settings. These limitations fall into three key domains: logistical delays, infrastructure and capacity constraints, and technical and diagnostic limitations.
One of the primary drawbacks of centralized TB testing is its dependence on transporting specimens from geographically peripheral health facilities to distant, often urban-based laboratories. In many low- and middle-income countries (LMICs), such transport systems are unreliable, resulting in prolonged turnaround times, sample degradation, and compromised diagnostic accuracy [5, 6]. Cold-chain requirements further increase operational complexity and cost, particularly in remote areas with limited infrastructure [3].
Centralized laboratories frequently experience diagnostic backlogs due to the high volume of samples they process — especially amid growing demands linked to drug-resistant TB cases. These bottlenecks can delay the initiation of treatment, increase patient loss between follow-ups, and contribute to ongoing community transmission [19, 20]. In settings with limited staffing and equipment, these delays are further compounded by workforce shortages and uneven access to adequate biosafety-level facilities [4, 21].
Although molecular platforms in centralized labs have improved detection speed, many of them are limited in diagnostic breadth, particularly in detecting emerging or rare drug resistance mutations [21]. Conventional culture-based methods, though comprehensive, are time-intensive and demand high technical expertise. In addition, certain sample types (e.g., stool in pediatric TB) require immediate processing, which is often unfeasible in centralized workflows [20, 22].
Decentralized diagnostic approaches offer multiple advantages over traditional centralized testing systems, particularly in improving TB detection in underserved, high-burden regions. These benefits can be grouped into four primary domains: timeliness of diagnosis, accessibility and equity, health system efficiency, and patient-centered care.
Relocating diagnostic services closer to the point of care significantly reduces delays associated with specimen transport and laboratory backlog. In decentralized settings, patients can often receive results within hours rather than days or weeks, enabling faster initiation of treatment and improving infection control at the community level [8, 12]. This is particularly important for controlling transmission in densely populated or high-mobility regions.
Decentralized testing enables greater access to TB diagnostics in rural, remote, and marginalized populations. By lowering geographic and infrastructural barriers, it enhances diagnostic coverage and equity, particularly in areas where centralized laboratory access is impractical or unaffordable [7, 14, 23]. These models often rely on portable platforms or mobile units, which are adaptable to varied field conditions.
Shifting routine diagnostic tasks to peripheral laboratories alleviates pressure on overburdened central facilities. This redistribution of workload improves the efficiency of laboratory networks and enables central labs to focus on more complex diagnostics, such as drug-resistance profiling and culture-based testing [24, 25]. As a result, both central and peripheral systems can function more effectively within an integrated diagnostic network.
Decentralized diagnostics facilitate greater community trust and engagement by embedding services within local health systems. Studies have linked decentralized care models to improved patient satisfaction, higher rates of treatment adherence, and greater continuity of care — especially when services are culturally-tailored and delivered by trusted local providers [14, 26]. These models also empower primary care providers to take a more active role in TB control.
Decentralized diagnostics improve patient satisfaction by reducing travel time, costs, and waiting times. Studies in Ethiopia and Guinea have found that community-based decentralized services have led to higher treatment adherence and completion rates [14, 16]. Considering patient perspectives is essential for designing people-centered TB diagnostic systems.
A comparative summary of centralized and decentralized TB diagnostic models — highlighting differences in logistics, infrastructure, personnel needs, and scalability — is presented in Table 1.
Comparative Features of Centralized vs. Decentralized Tuberculosis (TB) Diagnostic Models
| Dimension | Centralized Testing | Decentralized Testing |
|---|---|---|
| Test Location | National or regional central laboratories | Primary care settings or point-of-care (POC) sites |
| Turnaround Time | Days to weeks | Minutes to hours |
| Infrastructure | High-complexity set-up with biosafety and cold chain | Low-resource adaptable, portable platforms |
| Sample Logistics | Requires long-distance transport, cold chain | On-site testing, minimal logistics |
| Human Resources | Requires highly-trained laboratory specialists | Operable by general health workers with minimal training |
| Diagnostic Access | Limited in rural and remote areas | High accessibility across decentralized regions |
| Operational Cost | High fixed and variable costs | Lower marginal cost after implementation |
| Scalability | Limited by central lab capacity | Highly scalable across diverse health system levels |
| Patient Perspective | Indirect; limited engagement | Higher satisfaction, reduced travel costs, better adherence |
| Socio-cultural adaptability | Low (standardized protocols, limited cultural tailoring) | High (adaptable to local context, community involvement) |
While decentralized TB testing presents substantial benefits for improving access and timeliness, its widespread implementation remains constrained by multiple interdependent challenges. These barriers fall into five principal categories: quality assurance, human resources, infrastructure, financial sustainability, and community engagement.
Ensuring consistent diagnostic accuracy across a distributed network of primary laboratories remains a key challenge. Decentralized settings often lack comprehensive internal quality control (IQC) systems, regular external quality assessments (EQA), and standardized proficiency testing frameworks [15]. Without robust quality assurance protocols, test results may be unreliable, potentially undermining clinical decision-making and surveillance accuracy.
Although many decentralized testing platforms are designed for simplified use, successful implementation still relies on a skilled and retained workforce. Staff in remote laboratories require training in biosafety, equipment maintenance, and result interpretation [10, 16]. However, workforce shortages, limited career development opportunities, and high attrition rates in rural areas continue to impede program sustainability [17].
Primary laboratories may lack the basic physical and operational infrastructure necessary to support decentralized diagnostics. Stable power supply, clean water, biosafety conditions, and waste management systems are often insufficiently developed [25, 27]. Additionally, weak supply chains complicate the reliable delivery and storage of diagnostic reagents and consumables, especially in geographically isolated regions.
While decentralized models can reduce long-term costs by improving access and reducing delays, their initial setup and maintenance costs are significant. These include expenses for equipment procurement, personnel training, facility upgrades, and inventory management systems [15, 28]. Many low-income countries face challenges in securing sustained funding, particularly when donor support is short-term or fragmented.
Although initial investment and maintenance costs are high, studies show that decentralization can reduce long-term costs by shortening delays in diagnosis, lowering transmission rates, and improving adherence, all of which improve overall cost-effectiveness [15, 23].
A lack of community awareness and persistent social barriers may limit the uptake of decentralized services. Factors such as stigma, low TB literacy, and lack of trust in health-care systems contribute to under-utilization, even where services exist [18, 29]. Furthermore, logistical factors (such as distance to clinics or indirect costs), as well as cultural factors, may dissuade individuals from seeking diagnosis unless proactive, community-based engagement is undertaken.
Social stigma, low health literacy, and cultural misconceptions significantly limit the uptake of decentralized TB diagnostics, especially in marginalized groups. These factors can lead to delayed testing and treatment. Community education campaigns and culturally-adapted engagement strategies are essential for addressing these barriers [18, 29].
Decentralized TB diagnostics face multiple interrelated implementation challenges that span technical, infrastructural, financial, and social domains. A visual synthesis of these barriers is presented in Figure 1.
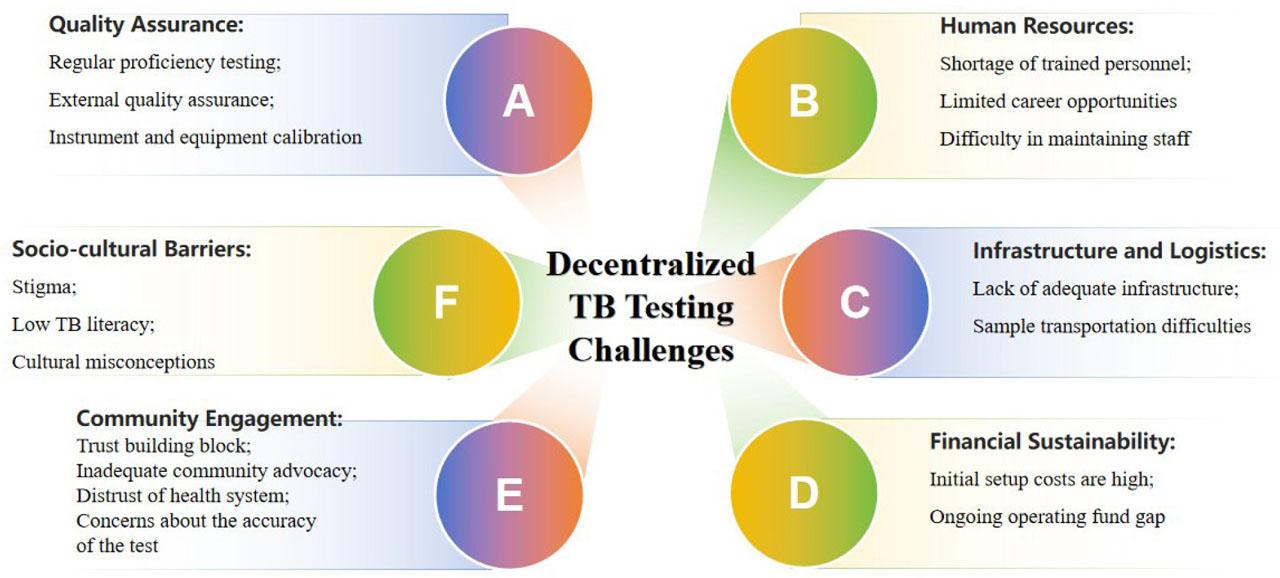
Six-Domain Challenges in Decentralized TB Diagnostic Implementation
Note: The implementation of decentralized tuberculosis (TB) diagnostic testing is hindered by interconnected challenges spanning six critical domains (A–F): A. Quality Assurance: Requires regular proficiency testing, external quality assurance, and instrument/equipment calibration to ensure diagnostic accuracy [13,25,35]; B. Human Resources: Includes shortages of trained personnel, limited career development opportunities, and difficulties in retaining staff [14,24]; C. Infrastructure and Logistics: Encompasses inadequate infrastructure, sample transportation difficulties, and operational logistics challenges [1,7]; D. Financial Sustainability: Entails high initial setup costs, gaps in ongoing operational funding, and long-term sustainability concerns [19,23]; E. Community Engagement: Involves trust-building barriers, insufficient community advocacy, and concerns regarding test accuracy [16,18]; F. Socio-Cultural Barriers: Encompasses social stigma, low health literacy, and cultural misconceptions that limit service uptake [18,24,29]
The COVID-19 pandemic has triggered an unprecedented transformation in diagnostic infrastructure and public health systems, offering new opportunities to scale decentralized tuberculosis (TB) testing. Six key strategic enablers are emerging as pivotal for the long-term sustainability and effectiveness of decentralized diagnostic models.
Pandemic-driven investments have significantly improved basic laboratory readiness, including biosafety facilities, ventilation systems, and waste-disposal mechanisms. These upgrades create a stronger foundation for localized TB testing, especially in primary care facilities and rural laboratories that were previously under-resourced [9].
The adoption of Electronic Health Records (EHRs), Laboratory Information Systems (LIS), and mobile data platforms has enhanced real-time data sharing, remote monitoring, and test reporting efficiency. These digital tools support integrated care pathways and allow decentralized facilities to connect with national TB surveillance systems, improving response coordination [30, 31].
AI-driven tools are increasingly used for radiograph interpretation, pattern recognition, and drug-resistance prediction, enabling frontline staff to make informed decisions without relying on central expertise. These tools expand access to specialist-level diagnostic support in low-resource settings and facilitate early detection of multidrug-resistant TB (MDR-TB) [32, 33].
Portable molecular platforms, such as the Xpert MTB/RIF Ultra and loop-mediated isothermal amplification (LAMP) assays, offer high sensitivity, rapid turnaround, and low training requirements. These assays enable reliable TB diagnosis at the point of care and are adaptable to settings with limited laboratory infrastructure [12, 34].
Advancements in device design have led to semi-automated and miniaturized testing systems, such as battery-operated analyzers and droplet digital PCR. These devices reduce human error, improve portability, and lower the technical barriers to decentralized implementation, especially in remote or mobile clinics [35, 36].
Governments and global health actors are fostering interconnected laboratory networks that enable harmonized protocols, shared resources, and rapid dissemination of innovations. Programs like India's National Tuberculosis Elimination Program (NTEP) exemplify how policy integration and digital platforms can accelerate the adoption of decentralized TB diagnostics and ensure quality assurance across facilities [37, 38].
These enablers, shaped by the response to COVID-19 and subsequent diagnostic system investments, collectively support the transition toward a more inclusive and sustainable TB diagnostic model. A visual summary of these strategic domains is provided in Figure 2.
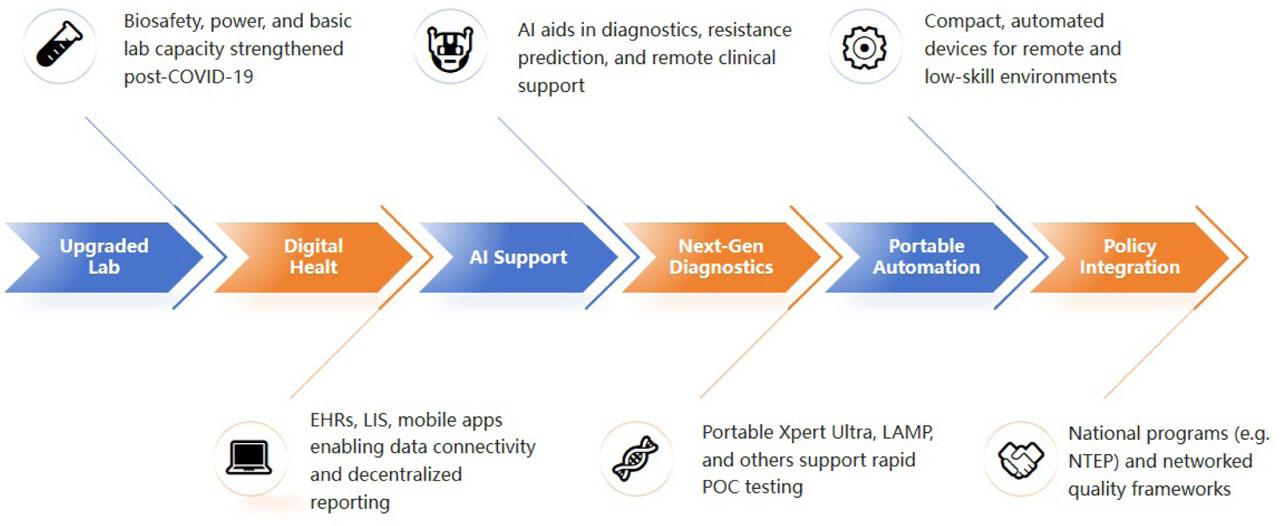
Strategic enablers of decentralized TB diagnostics in the post-pandemic context. Six domains are facilitating the transition from centralized to decentralized TB diagnostic models: enhanced laboratory infrastructure, digital connectivity, artificial intelligence, portable molecular platforms, miniaturized automation, and policy-driven diagnostic networks. These enablers work synergistically to promote accessibility, accuracy, and sustainability in TB testing
Abbreviations: EHRs: Electronic Health Records; LIS: Laboratory Information Systems; AI: Artificial Intelligence; LAMP: Loop-mediated Isothermal Amplification; NTEP: National Tuberculosis Elimination Program
To maximize the long-term impact of decentralized tuberculosis (TB) diagnostic systems, sustained policy support and targeted strategic investments are essential. Based on recent evidence and post-COVID infrastructure gains, seven future directions are proposed to strengthen decentralized TB diagnostic capacity and support its integration into national health systems.
Governments should formally incorporate decentralized testing models into national TB control strategies, ensuring consistent funding, standard operating procedures, and integration with referral networks. This will promote system-wide scalability and policy continuity beyond pilot or donor-driven programs.
To safeguard diagnostic accuracy across primary care settings, countries must establish national regulatory frameworks mandating internal quality control (IQC), external proficiency testing (EQA), and standardized training for decentralized testing sites.
Blended financing models — combining domestic health budgets, international aid, and public-private partnerships — should be explored to support the initial investment and long-term operational sustainability of decentralized platforms, particularly in low- and middle-income countries [28].
National and regional training programs should focus on building and retaining skilled diagnostic personnel through certification schemes, career progression opportunities, and incentives for rural deployment [10, 16].
Health systems must prioritize the interoperability of electronic health records (EHRs), laboratory information systems (LIS), and telemedicine platforms with TB diagnostic tools. Scaling up AI-based image analysis and decision support systems will further enhance diagnostic reach and precision [30, 32].
Culturally-adapted community engagement strategies should be implemented to reduce stigma, improve TB literacy, and facilitate early testing uptake. Mobile testing units, outreach programs, and community health workers can play a key role in increasing service utilization [18, 29].
Countries should participate in regional and global laboratory networks to facilitate rapid technology transfer, the harmonization of testing protocols, and shared learning from successful implementation models — for example, India's NTEP and Zambia's diagnostic optimization strategies [38].
To translate decentralized diagnostic strategies into sustainable practice, coordinated actions across policy domains and system levels will be required. These are summarized in Table 2.
Policy and Action Matrix for Decentralized TB Diagnostic Implementation
| Future Direction | Policy Focus | Implementation Level |
|---|---|---|
| Institutionalization in NTPs | Health Policy | National |
| Regulatory & Quality Frameworks | Regulation & Standards | National |
| Sustainable Financing | Health Economics | National/International |
| Capacity Building for Workforce | Human Resources | Regional/National |
| Integration of Digital & AI Tools | Digital Health | National/Facility |
| Community-Centered Models | Public Engagement | Local/Community |
| Global Collaboration | Global Health | Regional/Global |
| Evidence quality and research | Promote high-quality RCTs, prospective studies | National/International |
| Patient-centered design | Incorporate patient feedback and satisfaction measures | Local/Community |
| Regional adaptation | Tailor strategies to local context | National/Regional |
Abbreviations: NTPs: National Tuberculosis Programs; AI: Artificial Intelligence
Decentralization strategies must be tailored to local contexts. For example, India's NTEP successfully integrates digital tools and national networks; sub-Saharan African countries prioritize mobile clinics; and China explores AI-driven diagnostic tools in urban community settings. Policymakers should adapt strategies to regional epidemiology, infrastructure, and health system capacity.
While this review provides a comprehensive synthesis of decentralized TB diagnostics, several methodological limitations warrant consideration. The evidence base primarily comprises observational studies, small-scale pilots, and implementation reports, rather than randomized controlled trials (RCTs) or large prospective cohort studies. This reliance on lower-tier evidence introduces potential selection bias, as many studies were conducted at optimized demonstration sites rather than routine care settings. The predominance of short-term evaluations (< 3 years) further limits assessment of long-term sustainability and cost-effectiveness.
Most notably, the absence of multicenter RCTs comparing centralized versus decentralized models precludes definitive causal inferences about health outcomes. Current evidence cannot conclusively determine whether observed improvements in diagnostic access reflect true strengthening of a system rather than redistribution of existing capacity. Additionally, heterogeneity in outcome measures (e.g., varying definitions of “turnaround time”) complicates cross-study comparisons. Future research should prioritize controlled trials with standardized metrics and longitudinal designs to better characterize operational impacts and cost-benefit ratios across different health system contexts.
Tuberculosis (TB) diagnostics is entering a new era, propelled by the synergistic impact of infrastructure upgrades, digital health innovations, and next-generation molecular technologies. Together, these advances lay the groundwork for a decentralized diagnostic ecosystem that is more responsive, equitable, and technically robust — particularly in resource-limited and high-burden settings.
Decentralized TB testing promises earlier case detection, reduced transmission, and greater health system efficiency. However, realizing this potential will depend on overcoming persistent challenges related to quality assurance, workforce shortages, and financial sustainability, while embedding diagnostic services within patient-centered, community-supported frameworks.
Looking ahead, success will require integrated policy support, sustained investment, and cross-sector collaboration to institutionalize decentralized diagnostics as a core component of national TB programs. By aligning strategic opportunities with public health priorities, we can accelerate progress toward universal diagnostic access and move closer to the long-term goal of eliminating tuberculosis as a global health threat.