
Hemophilus influenzae is an aerobic gram-negative bacillus that can colonize the upper respiratory tract in humans, among others. However, it is rarely recognized as a cause of invasive infections in adults [1]. Because this is a fastidious bacterium and it only grows in vitro on enriched agar media (e.g., chocolate agar), its identification is impossible when only routinely used media are applied.
The aim of this study was to analyze the number and drug susceptibility profile of invasive infections caused by H. influenzae in the period from January 1, 2022 to May 31, 2024. The analysis focused on patients hospitalized at the Cardinal Stefan Wyszyński Regional Specialist Hospital in Lublin (WSS). A retrospective analysis of the microbiological test results from the hospital’s microbiology laboratory was conducted, focusing on invasive infections caused by H. influenzae. The number of infections recorded in the analyzed months (i.e., from January 1, 2022 to May 31, 2024) was compared.
The study group consisted of patients aged 18 to 87 years (15 men and 12 women). Among the evaluated group were patients with additional conditions such as hypertension, coronary artery disease, heart failure, chronic kidney disease, and non-insulin-dependent diabetes. Invasive infection was defined as the detection of H. influenzae in specimens such as cerebrospinal fluid (always), blood (always), deep wound infection (if monomicrobial), and bronchoalveolar lavage fluid (in radiologically confirmed community-acquired pneumonia, after exclusion of other possible causes of pneumonia), as well as in swabs taken by a physician from patients with acute sinusitis, otitis media, and/or acute pharyngitis (if monomicrobial), treated as an upper respiratory tract infection. A 5% risk of error was adopted in the study, so for p < 0.05, the differences were considered statistically significant. Calculations were performed using Statistica 13 software (StatSoft, Inc.). From October 1, 2023 to the end of May 2024, we observed a significantly higher number of invasive infections caused by this pathogen (3 cases per month vs. 0.095 cases per month; p<0.05) compared to the previous months analyzed (i.e., from January 1, 2022 to September 30, 2023). The increasing trend of invasive H. influenzae infections was also reported by the National Reference Center for Bacterial Infections of the Central Nervous System [2]. The available literature reports similar observations regarding both the increase in invasive H. influenzae infections and changes in the antibiotic susceptibility pattern. These changes were attributed by the authors to the SARS-CoV-2 pandemic [3].
At the Regional Specialist Hospital (WSS), from January 1, 2022 to September 30, 2023, H. influenzae was detected in specimens from three patients, two of whom required treatment, while the result in one patient was considered colonization. From October 1, 2023 to March 31, 2024, H. influenzae was detected in specimens from 24 patients; in 19 patients, it was necessary to start antibiotic therapy; and 5 patients had a co-infection that did not require treatment modification of the antimicrobial therapy already applied. The infections involved: lower and upper respiratory tracts in intubated patients; specimens obtained by bronchoscopy; while in others, swabs from the infected site were collected by a physician during examination (21 cases), blood culture (1 case), deep swab from a wound collected by a physician (1 case), and cerebrospinal fluid collected by a physician using a lumbar puncture method (1case) (see Figure 1). A concerning high increase in upper respiratory tract infections (acute pharyngitis, otitis media, and sinusitis) was also noted in patients treated on an outpatient basis.
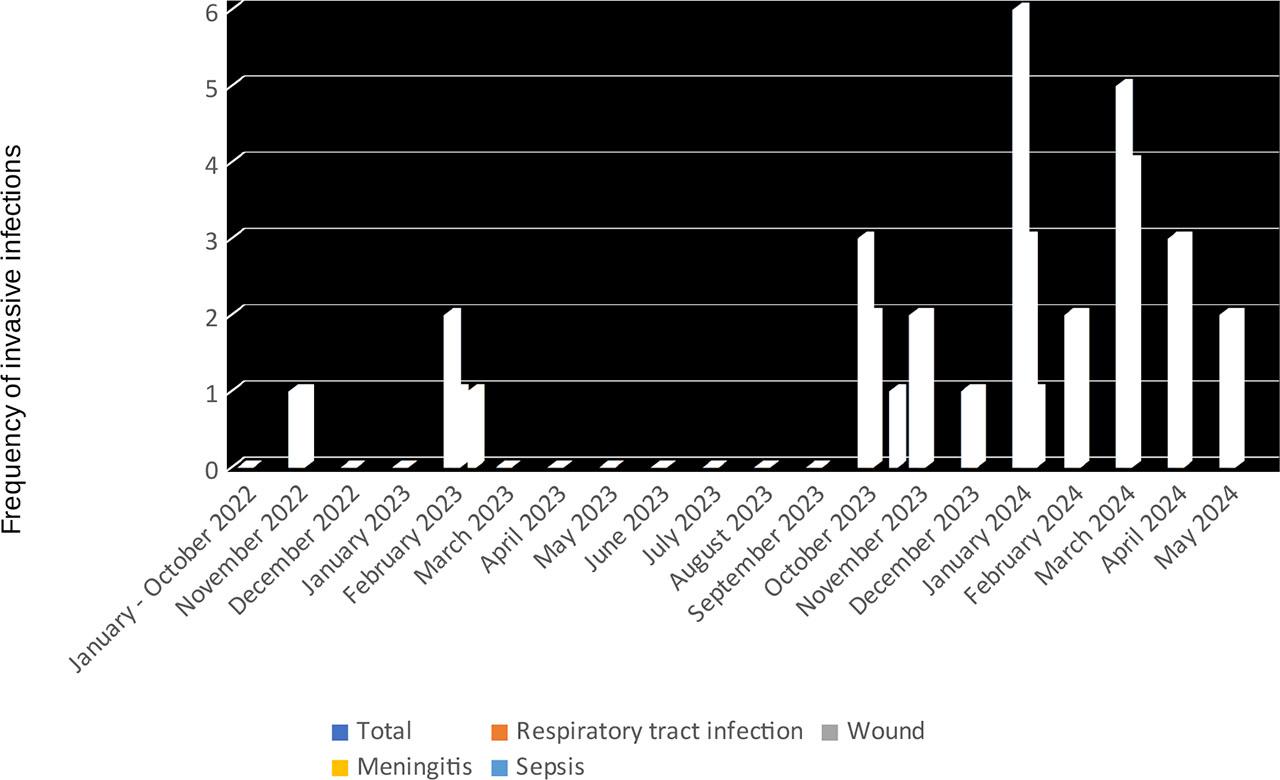
Frequency of invasive Hemophilus influenzae infections in individual months from January 2022 to May 2024, with consideration of the type of infection. The Y-axis shows the number of cases
Based on the performed antibiograms, the percentage of sensitivity to antibiotics (ampicillin, amoxicillin with clavulanic acid, cefotaxime, ciprofloxacin, and trimethoprim/sulfamethoxazole) was determined [4] (see Figure 2). The highest sensitivity was observed for ciprofloxacin and cefotaxime (100%). The tested strains (87.5%) were sensitive to trimethoprim/sulfamethoxazole, and for 68.75%, sensitivity was confirmed for amoxicillin with clavulanic acid, while the highest resistance rate was observed for ampicillin, with only 43.75% of the analyzed strains being sensitive.
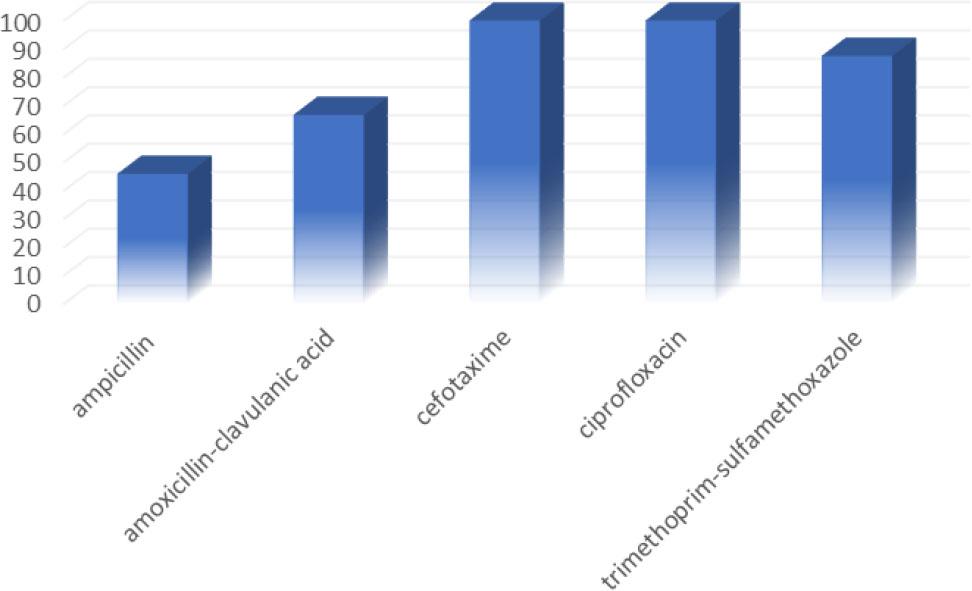
Antibiotic susceptibility of the tested strains of Hemophilus influenzae (n=24). The Y-axis shows the percentage of sensitivity to specific antibiotics (X-axis) determined for all tested strains during the period from October 1, 2023 to May 31, 2024
H. influenzae is increasingly being identified as a cause of invasive infections. The majority of infections involved both the lower and upper respiratory tracts (87.5%). Other infections included blood (4.17%), deep wound infection (4.17%), and meningitis (4.17%). In the case of an infection caused by this bacterium, it is always necessary to perform antibiotic susceptibility testing in order to apply appropriate antibiotic therapy. Due to the high percentage of resistant strains, ampicillin and amoxicillin with clavulanic acid are not antibiotics that can be used in empirical treatment. For such purposes, third-generation cephalosporins (cefotaxime or ceftriaxone) should be used, and if possible, therapy should be de-escalated as soon as susceptibility results are obtained. In cases of contraindications to the use of beta-lactams in treatment, trimethoprim/sulfamethoxazole or ciprofloxacin can be used. Only third-generation cephalosporins and ciprofloxacin showed 100% sensitivity among the tested strains. The selection of appropriate antibiotics is particularly important for patients whose identification was made solely by molecular methods (multiplex PCR) without obtaining culture. In such a situation, determining the susceptibility profile is not possible, and one should rely on the analysis of available data regarding H. influenzae susceptibility and treatment recommendations [5]. It is important to note that not all antibiotics dedicated to treating H. influenzae infections are available in oral form, which is significant when treating patients on an outpatient basis. Available in oral form (tablets) are amoxicillin—it can be used if in vitro sensitivity to ampicillin is confirmed, amoxicillin with clavulanic acid, ciprofloxacin, and trimethoprim/sulfamethoxazole.
The profile of local invasive infections can be highly dynamic. It is necessary to systematically analyze and report the microorganisms that most often occur as the etiological agent of such infections, as well as those that have been found to increase significantly. To establish recommendations for empirical antibiotic therapy, it is essential to determine the antibiotic susceptibility profile of such microorganisms. In this study, a more than 31-fold increase in invasive infections caused by H. influenzae was observed.