
Gastric cancer is a lethal tumor that occurs in the stomach, usually arising from the mucosal cells within the wall of the stomach [1]. There have been many cases of gastric cancer in recent years, but its exact etiology is still incompletely understood, and it is mostly thought to be related to dietary habits, bacterial infections, and genetic factors [2]. For early gastric cancer, radical surgery can remove the lesion in time, which is of great significance to enhance the survival period and improve the outcome of patients [3]. Therefore, early diagnosis and intervention are the key to preventing and treating gastric cancer. Endoscopic submucosal dissection (ESD) is a minimally invasive surgery suitable for the treatment of early gastric cancer, in which the resection operation of diseased tissue in the submucosal layer is carried out through endoscopy to achieve curative effect [4]. Although ESD has been widely used in clinical treatment worldwide and has shown unique advantages, there are still some patients with gastric cancer who relapse after treatment, which affects the prognosis and survival. In this context, screening and follow-up of gastric cancer patients after ESD can help timely detection and re-treatment of tumor recurrence.
The role of long non-coding RNA in the pathological process of tumors has become a hot topic for scientists. In the exploration of gastric cancer, Luo et al. noted that lncRNA EIF3J-DT mediates the activity of gastric cancer cells and tumor progression and was related to the chemotherapy sensitivity and prognosis of patients [5]. Zhang et al. also reported that lncRNA CRYM-AS1 is involved in the survival and tumor deterioration of gastric cancer patients and is a potential biomarker for gastric cancer treatment [6]. LncRNA LAMTOR5-AS1 (LAMTOR5-AS1) is located on chromosome 1p13.3, which was revealed to be a candidate factor for risk prediction, diagnosis and prognosis of different cancers [7, 8]. For example, LAMTOR5-AS1 was prominently expressed in prostate cancer and contributed to the early identification of patients [9]. Meanwhile, there is an association between LAMTOR5-AS1 and colorectal cancer, and its abnormally high expression may affect patient survival and prognosis [10]. However, the predictive role of LAMTOR5-AS1 in gastric cancer is unclear.
Herein, this study focused on early gastric cancer patients undergoing ESD treatment, which evaluated the diagnostic potential of LAMTOR5-AS1 in patients with postoperative recurrence, and further explored the possible molecular underpinnings of gastric cancer patients, aiming to provide a basis for the clinical studies of postoperative recurrence markers in patients with early gastric cancer.
Patients with early gastric cancer who underwent ESD in West China Hospital/West China School of Nursing, Sichuan University from 2020 to 2021 were selected as the research targets. Another 130 persons who underwent gastric biopsy and were confirmed to be normal by pathological examination were randomly chosen to serve as the controls. The inclusion requirements were as follows: 1) a pathological diagnosis of gastric cancer with surgical features for ESD resection. 2) No antitumor treatment such as immunotherapy, targeted therapy, chemotherapy, or radiotherapy before participating in the study. 3) Patients volunteered to enroll in this study and had complete clinical data. Patients with one of the following items were excluded: 1) Patients were complicated with autoimmune diseases or other malignant tumors. 2) Patients with previous gastrectomy or other major surgical procedures. 3) Patients are not suitable for ESD treatment due to their condition.
The research received ethical clearance from the institutional review board of West China Hospital/West China School of Nursing, Sichuan University, and all participants provided informed consent in writing.
Gastric tissue samples from patients in the control group were collected as control samples, and tissues obtained from patients with early gastric cancer after ESD were collected as experimental samples. All tissue samples were briefly washed and stored in an ultra-low temperature refrigerator for further use.
Venous blood (5 mL) was collected from gastric cancer patients and controls in the fasting state. Serum samples were isolated after centrifugation at 3000 rpm for 5 min. Carcinoembryonic antigen (CEA), carbohydrate antigen 199 (CA199), carbohydrate antigen 242 (CA242), and carbohydrate antigen 724 (CA724) were determined by a completely automated immunoassay analyzer (Abbott Laboratories, USA).
All patients who received ESD were followed up for three years. The recurrence of the patients was recorded in time by telephone communication and regular outpatient review. Clinically, recurrence was defined as the return of tumor lesions at or within 1cm of the original resection site six months after surgery.
Gastric cancer cells (MKN-74) were purchased from the Chinese Academy of Sciences (Shanghai, China). These cells were cultivated in RPMI-1640 medium (Corning, USA) with 10% FBS, and the acclimatization conditions were set at 5% CO2, 37°C.
Negative control (si-NC), LAMTOR5-AS1 siRNA (si-LAMTOR5-AS1), and miR-331-3p inhibitor/mimic were designed and provided by RiboBio (Shanghai, China). The transfection assay was performed with the participation of lipofectamine 3000 (Thermo Fisher, USA), and the treatment time was 48h.
The total RNA in the samples was extracted with TRIzol reagent, and the quality and integrity of the RNA were verified. cDNA was synthesized by Primer Script RT Master Mix Kit (TaKaRa, Japan). The RT-qPCR reaction system was configured with a CellDirect One-Step RT-qPCR kit (Thermo Fisher Scientific, USA), and gene amplification was performed on an RT-qPCR instrument (Baller, USA). GAPDH and U6 were the internal parameters for LAMTOR5-AS1 and miR-331-3p.
The binding site of LAMTOR5-AS1 to miR-331-3p was cloned into pmirGLO plasmid (Invitrogen, USA) to construct a wild-type plasmid (WT-LAMTOR5-AS1), while the mutated site was cloned to construct a mutant plasmid (MUT-LAMTOR5-AS1). The constructed plasmid was co-transfected with miR-331-3p inhibitor/mimic in MKN-74 cells, and the luciferase activity of LAMTOR5-AS1 was measured on a dual-luciferase reporter system (Promega, USA).
The cells to be tested were seeded in 96-well plates, which were placed in a constant temperature incubator at 37°C for cell incubation. CCK-8 reagent (Dojindo, Japan) was added to each well at 0, 1, 2, and 3 days of incubation, and incubation was continued for 2h. The absorbance of each well was measured using a microplate reader, and the wavelength was set at 450 nm. According to the absorbance measurement results, the proliferation level of gastric cancer cells was calculated.
Cells were suspended in RPMI 1640 medium and added to the upper chamber of the Transwell membrane, noting the generation of bubbles. Then, medium and FBS were added to the lower chamber. Transwell plates were placed in an incubator and cultured under appropriate conditions. The migrated cells were fixed and stained after 48 hours of treatment, and the results were counted under a microscope. The number of invading cells was assessed after Matrigel treatment of the Transwell chamber.
Statistical analyses were performed with SPSS 20.0 software and GraphPad Prism 10.0. Count data were represented by n (%), measurement data were presented as mean ± standard deviation (SD), and difference comparisons were analyzed using Student’s t-test (two groups) and one-way ANOVA (three or more groups). Correlation analysis was performed with the Chi-square test on the low-LAMTOR5-AS1 and high-LAMTOR5-AS1 group, as well as on the recurrence group and recurrence-free group. The diagnostic significance of LAMTOR5-AS1 was assessed by ROC analysis. Binary logistic regression was used to evaluate the independent risk factors for recurrence after ESD. Targeting relationship of LAMTOR5-AS1 and miR-331-3p predicted by ENCORI online database. P < 0.05 indicates the statistical significance.
LAMTOR5-AS1 was obviously upregulated in gastric cancer patients (1.62) relative to control individuals (1.00) in Figure 1a. The abnormally high expression of LAMTOR5-AS1 could discriminate early gastric cancer with relatively high sensitivity (82.31%) and specificity (85.38%), and the AUC was 0.9076 (P < 0.0001, cut off value = 1.308, Figure 1b). Moreover, the levels of CEA, CA199, CA242 and CA724 in gastric cancer patients were markedly higher than in control individuals, and the differences were significant (P < 0.001, Supplementary Table 1).

Expression and predictive ability of LAMTOR5-AS1. (a) LAMTOR5-AS1 was markedly upregulated in gastric cancer. (b) LAMTOR5-AS1 expression helps to distinguish gastric cancer patients from control individuals (AUC = 0.9076). (c) LAMTOR5-AS1 level was enhanced in the recurrent group. (d) Predictive potential of LAMTOR5-AS1 expression in early gastric cancer patients for recurrence after ESD (AUC = 0.8147). ***P < 0.001
Patients were grouped as low-LAMTOR5-AS1 group and high-LAMTOR5-AS1 group with the average LAMTOR5-AS1 expression as the cutoff. Overexpression of LAMTOR5-AS1 showed a significant association with the generation of recurrence (P = 0.025), T1b stage of TNM staging (P < 0.001) and the occurrence of lymph node metastasis (P = 0.008) in gastric cancer patients (Table 1).
Relationship between LAMTOR5-AS1 and clinical indicators in patients with gastric cancer
| Case (n/%) | Low LAMTOR5-AS1 (n = 63) | High LAMTOR5-AS1 (n = 67) | P | |
|---|---|---|---|---|
| Age (years) | 0.852 | |||
| ≤ 55 | 56/43.08 | 28/44.44 | 28/41.79 | |
| > 55 | 74/56.92 | 35/55.56 | 39/58.21 | |
| Sex | 0.660 | |||
| Male | 85/65.38 | 40/63.49 | 45/67.16 | |
| Female | 45/34.62 | 23/36.51 | 22/32.84 | |
| Tumor size (cm) | 0.054 | |||
| ≤ 5 | 65/50.00 | 26/41.27 | 39/58.21 | |
| > 5 | 65/50.00 | 37/58.73 | 28/41.79 | |
| Differentiation | 0.227 | |||
| Well, moderate | 61/46.92 | 33/52.38 | 28/41.79 | |
| Poor | 69/53.08 | 30/47.62 | 39/58.21 | |
| Recurrence | 0.025 | |||
| No | 113/86.92 | 59/93.65 | 54/80.60 | |
| Yes | 17/13.08 | 4/6.35 | 13/19.40 | |
| TNM stage | <0.001 | |||
| T1a | 50/38.46 | 38/60.32 | 12/17.91 | |
| T1b | 80/61.54 | 25/39.68 | 55/82.09 | |
| Lymph node metastasis | 0.008 | |||
| Negative | 65/50.00 | 39/61.90 | 26/38.81 | |
| Positive | 65/50.00 | 24/38.10 | 41/61.19 |
LAMTOR5-AS1 expression was higher in the recurrence group (1.99) than in the recurrence-free group (1.57) after ESD treatment (Figure 1c). Upregulation of LAMTOR5-AS1 also has a high value in predicting recurrence after ESD in early gastric cancer (AUC = 0.8147, sensitivity = 66.37%, specificity = 82.35%, P < 0.0001, cut off value = 1.709, Figure 1d).
Patients undergoing ESD were categorized into a recurrence group (n = 17) and a recurrence-free group (n = 113) according to whether they had a recurrence of gastric cancer (Table 2). Compared with the no recurrence group, patients in the recurrence group had significant differences in tumor poor differentiation (P = 0.009), T1b stage of TNM staging (P = 0.015), and the occurrence of lymph node metastasis (P = 0.019). Furthermore, high LAMTOR5-AS1 expression (P = 0.007), the increased of tumor size (P = 0.012), tumor poor differentiation (P = 0.018) and T1b stage of TNM staging (P = 0.026) were found to be independent risk factors affecting recurrence after ESD for early gastric cancer by Binary Logistic regression analysis (Table 3).
Comparison of the general data of the two groups of patients
| Indicators | Case (n/%) | Recurrence group (n = 17) | Recurrence-free group (n = 113) | P |
|---|---|---|---|---|
| Age (years) | 0.772 | |||
| ≤ 55 | 56/43.08 | 8/47.06 | 48/42.48 | |
| > 55 | 74/56.92 | 9/52.94 | 65/57.52 | |
| Sex | 0.542 | |||
| Male | 85/65.38 | 10/58.82 | 75/66.37 | |
| Female | 45/34.62 | 7/41.18 | 38/33.63 | |
| Tumor size (cm) | 0.069 | |||
| ≤ 5 | 65/50.00 | 5/29.41 | 60/53.10 | |
| > 5 | 65/50.00 | 12/70.59 | 53/46.90 | |
| Differentiation | 0.009 | |||
| Well, moderate | 61/46.92 | 3/17.65 | 58/51.33 | |
| Poor | 69/53.08 | 14/82.35 | 55/48.67 | |
| TNM stage | 0.015 | |||
| T1a | 50/38.46 | 2/11.76 | 48/42.48 | |
| T1b | 80/61.54 | 15/88.24 | 65/57.52 | |
| Lymph node metastasis | 0.019 | |||
| Negative | 65/50.00 | 4/23.53 | 61/53.98 | |
| Positive | 65/50.00 | 13/76.47 | 52/46.02 |
Binary logistic regression analysis of recurrence of early gastric cancer after endoscopic submucosal dissection
| Indicators | OR | 95% CI | P-value |
|---|---|---|---|
| LAMTOR5-AS1 | 0.088 | 0.015 - 0.516 | 0.007 |
| Age (years) | 0.549 | 0.155 - 1.948 | 0.353 |
| Sex (male/female) | 1.085 | 0.297 - 3.969 | 0.902 |
| Tumor size (cm) | 0.169 | 0.042 - 0.677 | 0.012 |
| Differentiation | 0.173 | 0.040 - 0.739 | 0.018 |
| TNM stage | 0.138 | 0.024 - 0.789 | 0.026 |
| Lymph node metastasis | 2.411 | 0.589 - 9.862 | 0.221 |
The ENCORI online bioinformatics website predicted the presence of binding sites between LAMTOR5-AS1 and miR-331-3p, and the luciferase activity assay provided experimental validation for the targeting interaction between them (Figure 2a). miR-331-3p was reduced in gastric cancer tissues and in the recurrence group (Figure 2b and 2c). In Figure 2d, LAMTOR5-AS1 and miR-331-3p levels in tissues were negatively correlated by Pearson correlation analysis (r = −0.5818, P < 0.0001). Additionally, the knockdown of LAMTOR5-AS1 resulted in a decrease in LAMTOR5-AS1 expression and an enhancement in miR-331-3p levels in the cells, while cotransfection with si-LAMTOR5-AS1 and miR-331-3p inhibitor restored the miR-331-3p expression (Figure 2e and 2f).
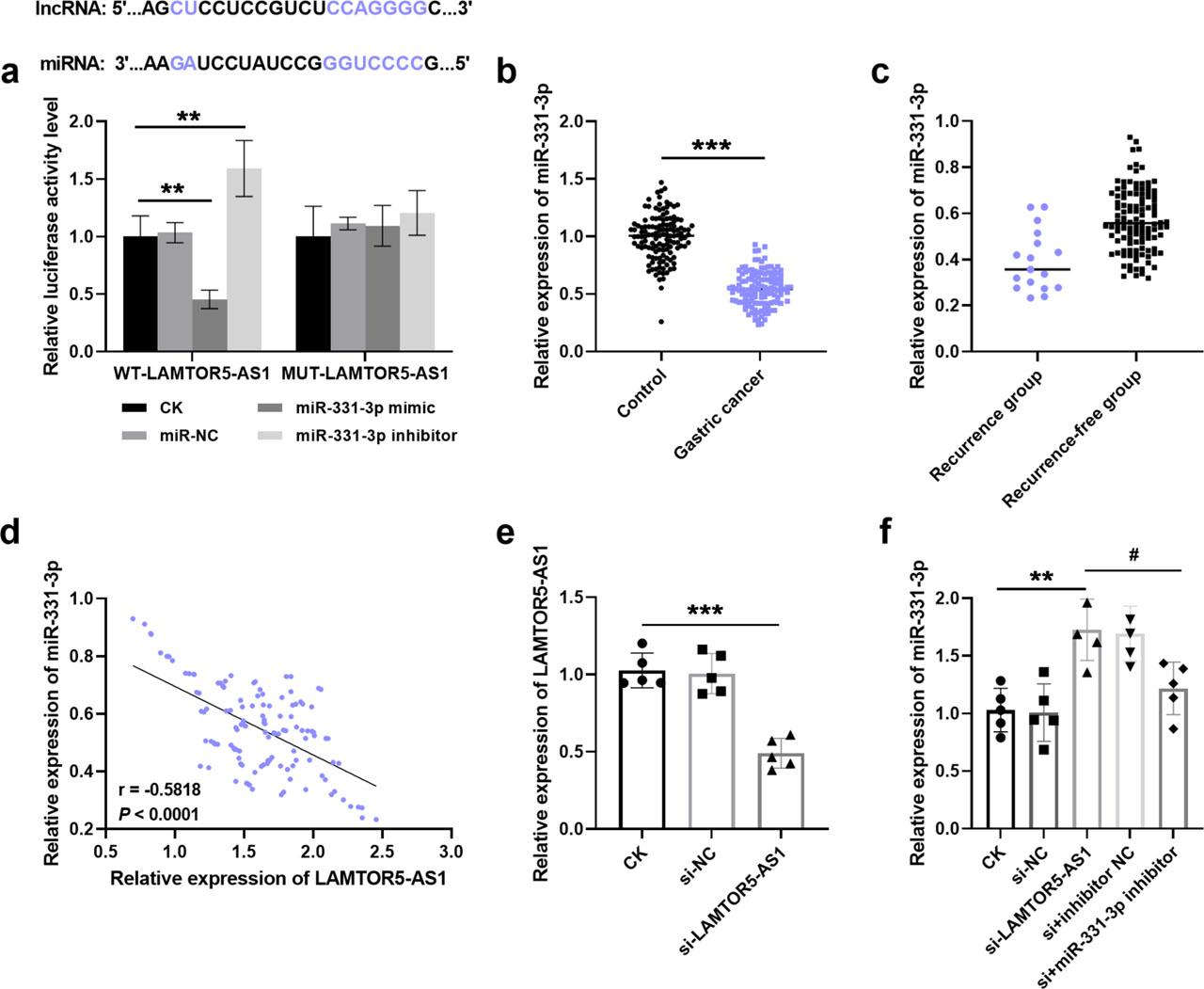
The targeting relationship between LAMTOR5-AS1 and miR-331-3p. (a) LAMTOR5-AS1 directly targets miR-331-3p in gastric cancer. (b) miR-331-3p was decreased in gastric cancer tissue. (c) miR-331-3p expression was downregulated in the recurrence group. (d) Regulatory relationship between LAMTOR5-AS1 and miR-331-3p (r=−0.5818, P < 0.0001). (e) Transfection efficiency of silencing LAMTOR5-AS1 in cells. (f) Expression of miR-331-3p in cells after transfection with silencing LAMTOR5-AS1 and miR-331-3p inhibitor. **P < 0.01, ***P < 0.001, vs CK; #P < 0.05, vs si-LAMTOR5-AS1
The transfection of si-LAMTOR5-AS1 into gastric cancer cells resulted in a reduction of their proliferation rate, while miR-331-3p knockdown reversed the downward trend of cell proliferation (Figure 3a). In addition, the downregulation of LAMTOR5-AS1 reduced the cell migration (Figure 3b) and invasion (Figure 3c) capacity, which was attenuated by the involvement of si-LAMTOR5-AS1 and miR-331-3p inhibitor. It is implied that silencing LAMTOR5-AS1 may ameliorate the development of gastric cancer, whereas miR-331-3p knockdown counteracted the suppressive efficacy of downregulating LAMTOR5-AS1 on gastric cancer.
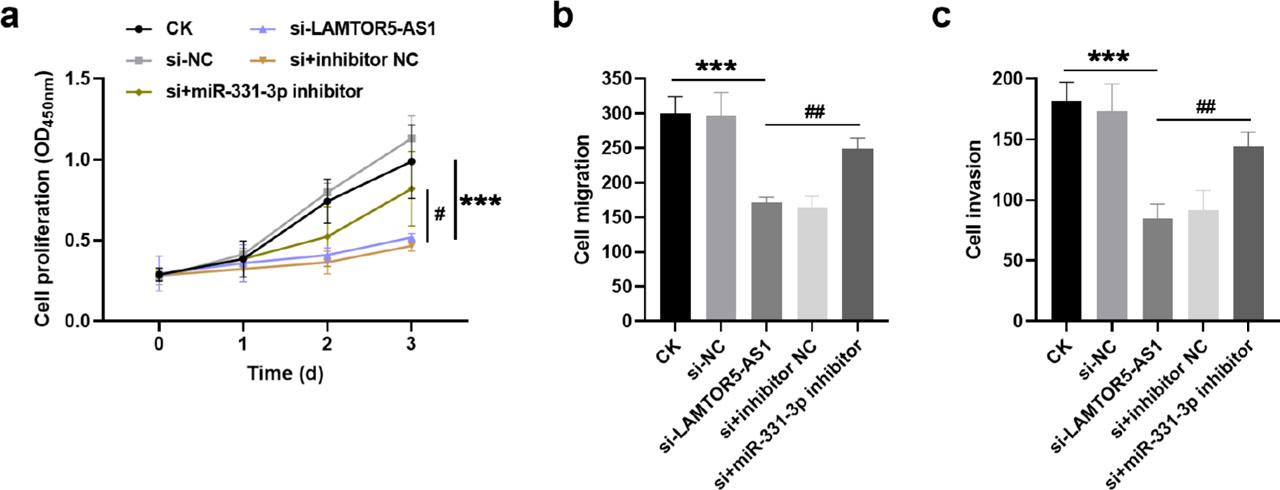
Effect of LAMTOR5-AS1 sponge miR-331-3p on gastric cancer cell proliferation (a), migration (b), and invasion (c). si-LAMTOR5-AS1 suppressed cell activity, which was reversed by miR-331-3p inhibitor. ***P < 0.001, vs CK; #P < 0.05, ##P < 0.01, vs si-LAMTOR5-AS1
The lesions of early gastric cancer are confined to the mucous membrane layer or submucosa, and the abnormalities of gastric mucosa can usually be directly observed through gastroscopy, which improves the detection rate of gastric cancer [11]. Studies have shown that the survival rate of patients with early gastric cancer can reach more than 90% within five years if timely intervention is carried out. ESD can completely dissect the gastric lesions and has the characteristics of less trauma, less bleeding and short recovery period [12]. Additionally, the cure rate of ESD for gastric cancer patients is significantly up-regulated compared to traditional endoscopic mucosal resection [13]. Unfortunately, recurrence still occurs in a portion of patients treated with ESD, threatening the prognostic survival of patients.
A large body of literature demonstrated the presence of aberrant non-coding RNA expression in the development of gastric cancer [ 14, 15, 16]. LAMTOR5-AS1 is an antisense transcription product of the LAMTOR5 gene, which was first found to be associated with breast cancer metastasis [10, 17]. Meanwhile, LAMTOR5-AS1 was elucidated to be upregulated in osteosarcoma cells to improve the level of oxidative stress by regulating NRF2 expression [18]. The LAMTOR5-AS1 was positively expressed in non-small cell lung cancer, indicating poor prognosis and affecting tumor progression through the sponge miR-506-3p/E2F6 axis, was also demonstrated by Chen and colleagues [19]. In this study, PCR experiments verified that LAMTOR5-AS1 was overexpressed in the tissue of gastric cancer patients, which was similar to most of the evidence. LAMTOR5-AS1 also had high sensitivity and specificity in distinguishing gastric cancer patients from healthy individuals, implying that LAMTOR5-AS1 has the potential to serve as a diagnostic indicator for early gastric cancer. Furthermore, LAMTOR5-AS1 was noted to be upregulated in the recurrence group, suggesting that elevated LAMTOR5-AS1 may be a predictor and risk factor for recurrence after ESD in gastric cancer.
The regulatory mechanisms of gastric cancer are complex, in which the growth of cancer cells are biological aspects directly related to the lesion [20, 21]. LncRNAs have attracted more and more attention by binding miRNAs to mediate the biological function of tumor cells and the development of malignant tumors. For example, lncRNA HCP5 sponge miR-3619-5p to promote gastric cancer generation and drug resistance, which brings a new direction for improving the cure of gastric cancer [22]. lncRNA MIAT was introduced to accelerate the growth and metastasis of gastric cancer cells by mediating the miR-331-3p/RAB5B axis, thus affecting the progression of gastric cancer [23]. Notably, miR-331-3p was a tumor suppressor ncRNA, which was downregulated in cervical cancer, breast cancer and lung cancer [ 24, 25, 26]. Importantly, miR-331-3p was also identified to be involved in gastric cancer progression, as confirmed by several in vitro cell experiments [27, 28]. The research presented here has identified miR-331-3p as a target of LAMTOR5-AS1 and was negatively regulated by it. The expression of miR-331-3p was decreased in gastric cancer tissue, and it also showed a downward trend in the recurrence group, suggesting that low expression of miR-331-3p may be related to the recurrence and poor prognosis of gastric cancer patients. Meanwhile, cellular experiments elucidated that silencing LAMTOR5-AS1 suppressed the growth, migration and invasion of gastric cancer cells, while co-transfection of si-LAMTOR5-AS1 and miR-331-3p inhibitor counteracted the effect of LAMTOR5-AS1 on cell viability. The above results suggest that LAMTOR5-AS1 knockdown mediates the growth of gastric cancer cells and may slow down the deterioration of pathological features by targeting miR-331-3p, and the LAMTOR5-AS1/miR-331-3p axis may be a relevant molecular mechanism involved in the development and recurrence after treatment of early gastric cancer.
This study still has some shortcomings. On the one hand, the samples included in this experiment are limited, and the number of samples needs to be increased in future explorations. On the other hand, a longer observation period is needed to evaluate the prognosis of the patients.
In conclusion, LAMTOR5-AS1 expression was increased in early gastric cancer and was associated with recurrence after ESD. LAMTOR5-AS1 was a risk factor for recurrence after ESD in patients with early gastric cancer and has a predictive value for post-treatment recurrence, which may affect the pathological process of gastric cancer through sponge miR-331-3p.